
Abstract
Depression is now recognised worldwide as a major public health issue and there have been recent attempts to better quantify its burden upon individuals and society. Traditionally mortality has been used as the main measure of health burden, but it has been recognised increasingly that this seriously underestimates the burden of mental illnesses such as depression. Indeed, the World Health Organization has described depression as an ‘unseen burden’ [1], and the Global Burden of Disease study reported that when measured by Disability Adjusted Life Years (DALY), unipolar major depression ranked fourth in 1990 and would rise to second by 2020 in terms of the overall burden of all diseases in the world. Furthermore, in terms of disability alone, which is defined as the restriction or lack of ability to perform an activity in the manner or range considered normal for a human being [2], unipolar major depression ranked first in 1990, afflicting 51 million people and contributing 10.7% of the total years lived with disability from all causes [1].
Similar findings have been reported from Australia. A burden of disease and injury study [3] found that in 1996 depression ranked fourth in terms of disease burden in Australia, contributing 3.7% of the total burden, and it ranked first in terms of years of life lost due to disability, contributing 8%, which is comparable to the worldwide estimate. Furthermore, the recent National Survey of Mental Health [4,5] confirmed the importance of depression and its associated disablement in the Australian community.
It has also been demonstrated in the primary care setting that those who suffer depressive disorders experience disability and diminished physical and mental functioning similar to patients with chronic diseases such as arthritis and diabetes [6,7]. Mood disorders have been shown to account for substantially more reduction in quality of life than do more common medical disorders such as hypertension and cardiac disease [8].
Most research to date in this area has drawn its samples from primary care or convenience settings, meaning findings may not be generalisable to one whole population. It is also difficult to prioritise and target groups with public health policy and interventions unless studies are conducted with representative population groups. Therefore, this study was designed to ascertain the prevalence of major depression in a representative sample of the South Australian population and to describe participants' use of health services and health related quality of life (HRQoL). Post-hoc hypotheses were tested as to possible differences between those with major depression, those with other depressive conditions and those who were not depressed.
Method
Data were gathered in 1998 using a Health Omnibus Survey of both metropolitan and rural South Australians at least 15 years of age. The Health Omnibus Survey is a user-pays survey for health organisations which in 1998 included areas such as asthma, arthritis, osteoporosis, diabetes, incontinence and risk factors (blood pressure, cholesterol, smoking, body mass index). The metropolitan sample was based on the collectors' districts (each about 200 dwellings) used by the Australian Bureau of Statistics in the 1996 census. Ten dwellings were chosen in each, by selecting every fourth household from a random starting point. Only one interview was conducted per household and, when more than one person over the age of 15 resided in that household, the respondent was the person who last had a birthday.
The rural sample was selected from towns with a population of 1000 or more in the 1996 Census, using the same procedure as for the metropolitan area. This sample frame comprises about 80% of the South Australian rural population.
The survey was conducted by experienced interviewers. For reliability purposes re-interviews for selected questions were conducted on a random 5% of each interviewer's work. Data were weighted according to benchmarks derived from the 1996 Australian Bureau of Statistics Census to provide estimates that would represent the South Australian population in terms of age, sex and region (metropolitan, non-metropolitan).
Depression assessment was undertaken using the mood module of the Primary Care Evaluation of Mental Disorders (PRIME-MD) instrument, which has demonstrated reliability and validity in primary health care settings [9,10]. It consists of 16 questions related to symptoms of depression experienced nearly every day for the last 2 weeks (categorised yes/no), and was embedded in the broader Health Omnibus Survey. Scoring to determine depression ‘caseness’ was undertaken at the data analysis stage using the PRIME-MD method for detection of DSM-III-R diagnoses. The PRIME-MD allows the identification of individual mood disorders, but for the purposes of these analyses, respondents were classified as having major depression, other depressions and no depression.
Indicators of severity were use and frequency of use of a range of services in the last month, measured as consultations with specific professionals and other community/hospital services, previous and current use of antidepressant medication and number of days unable to work or carry out normal duties in the last month because of ill health. A South Australian socioeconomic status indicator was determined using the Australian Bureau of Statistics' socioeconomic index of disadvantage based on postcode of residence [11].
Two health-related quality of life (HRQoL) instruments were used to assess morbidity. The first was the Short-form Health Status Questionnaire (SF-36), consisting of 36 questions which measure eight dimensions of health: physical functioning, role limitations due to physical health, bodily pain, general health, vitality, social functioning, role limitations due to emotional health and mental health [12]. In addition physical and mental component summary scales can be derived. Scores range from 0 to 100, and higher scores indicate better functioning. The SF-36 has been validated for use in Australia [13] and both Australian and South Australian norms have been produced [14,15].
The second instrument, developed in Australia, was the Assessment of Quality of Life (AQoL) instrument [16,17], and consists of 15 items which measure five dimensions of health-related quality of life: illness, independent living, social relationships, physical senses and psychological wellbeing. Individual items can be summed to provide a score for each dimension and an overall score to compare HRQoL profiles in a similar manner to the SF-36. In addition, an algorithm based on multi-attribute utility theory using a multiplicative model is available which adds health state preference weights to the responses to provide a utility score for each dimension and an overall utility score. Each dimension is scaled from 0 to 1, with zero representing the worst HRQoL (death) and one representing full or normal health without handicap, impairment or disability.
Statistical analyses were undertaken using
For the SF-36 and AQoL,
Results
From the 4400 households selected, 111 were found to be vacant dwellings. From the remaining dwellings, 3010 interviews were conducted (70.2% response rate). Non-response was due to refusal (658), contact not being established after six visits (408), language barrier (73), the selected respondent being absent for the duration of the survey (71) and illness (69).
Of the 3010 respondents, 205 (6.8%) (8.2% females and 5.4% males) had major depression, 319 (10.6%) had other depressions and no mood disorder was detected in 2486 (82.6%) respondents.
Table 1 shows health services used in the last month, with lowest use among the non-depressed, highest use in those with major depression and intermediate use in the other depressed group. The differences in use were statistically significant for all services except hospital inpatient care, other medical specialist consultations and the use of alternative health care professionals.
Use of health services in the last month
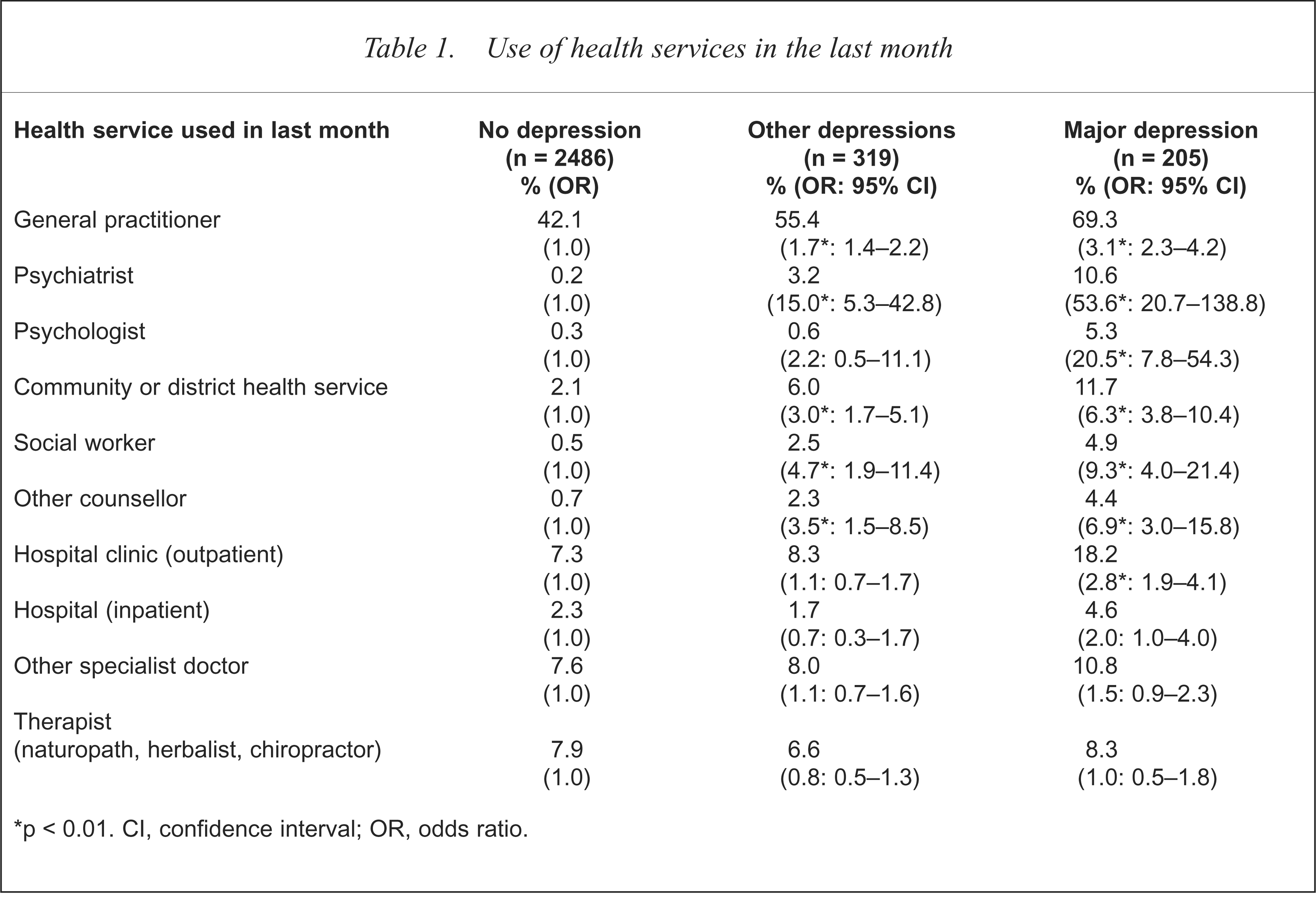
p < 0.01. CI, confidence interval; OR, odds ratio.
The mean number of attendances at health services in the last month for those with major depression was 3.8 (SD = 4.1) compared with 3.0 (SD = 3.4) for those with other depression and 2.2 (SD = 2.5) for those who were not depressed (F = 28.9, df = 2, p < 0.001). Only 20% of those with major depression had not attended a health service, compared with 26.1% of those with other depression and 47.2% of the not depressed. Of those with major depression, 39.5% had used services three or more times in the last month, compared with 21.3% and 13.3% of those with other depression and the not depressed.
Of those with major depression, 39.0% had taken an antidepressant in the past compared with 24.1% and 9.9% of those with other depression and no depression (p < 0.001). Of those with major depression, 19% were currently using an antidepressant compared with 6.9% and 1.6% of those with other depressions and no depression (p < 0.001).
The number of days in the last month that respondents were unable to work or carry out their normal duties because of their health, is presented in Table 2. Those with major depression had significantly more days in which they were unable to carry out their normal activities than those with other depression or the not depressed. Those with major depression had an average of 4.4 (SD = 7.8) days absence compared with 1.5 (SD = 4.6) days for those with other depression and 0.6 (SD = 3.0) days for the not depressed (F = 100.3, df = 2, p < 0.001).
Days lost from work/normal duties in the last month due to ill health
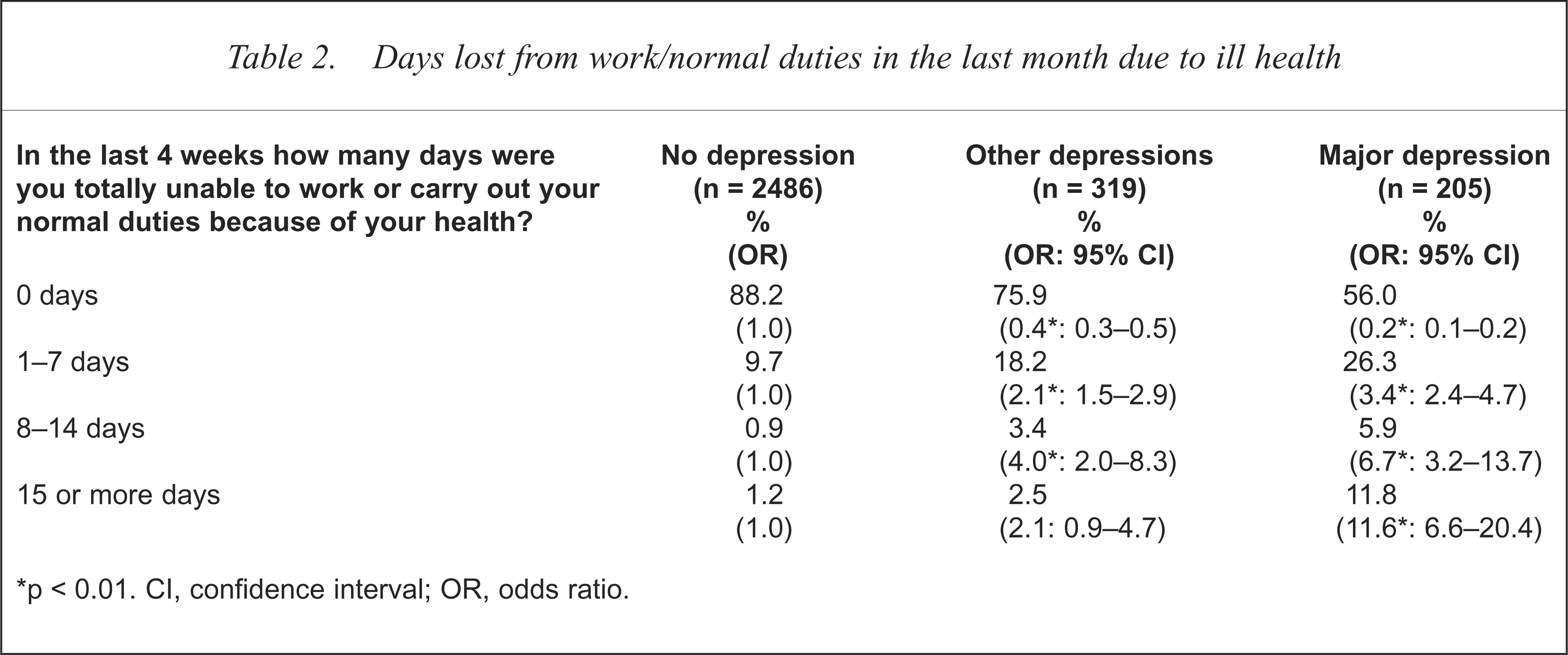
p < 0.01. CI, confidence interval; OR, odds ratio.
Those living in a low socioeconomic status area were twice as likely to have major depression than those in medium and high socioeconomic areas (χ2 = 33.2, df = 4, p < 0.001; see Table 3).
Depression category by socioeconomic status
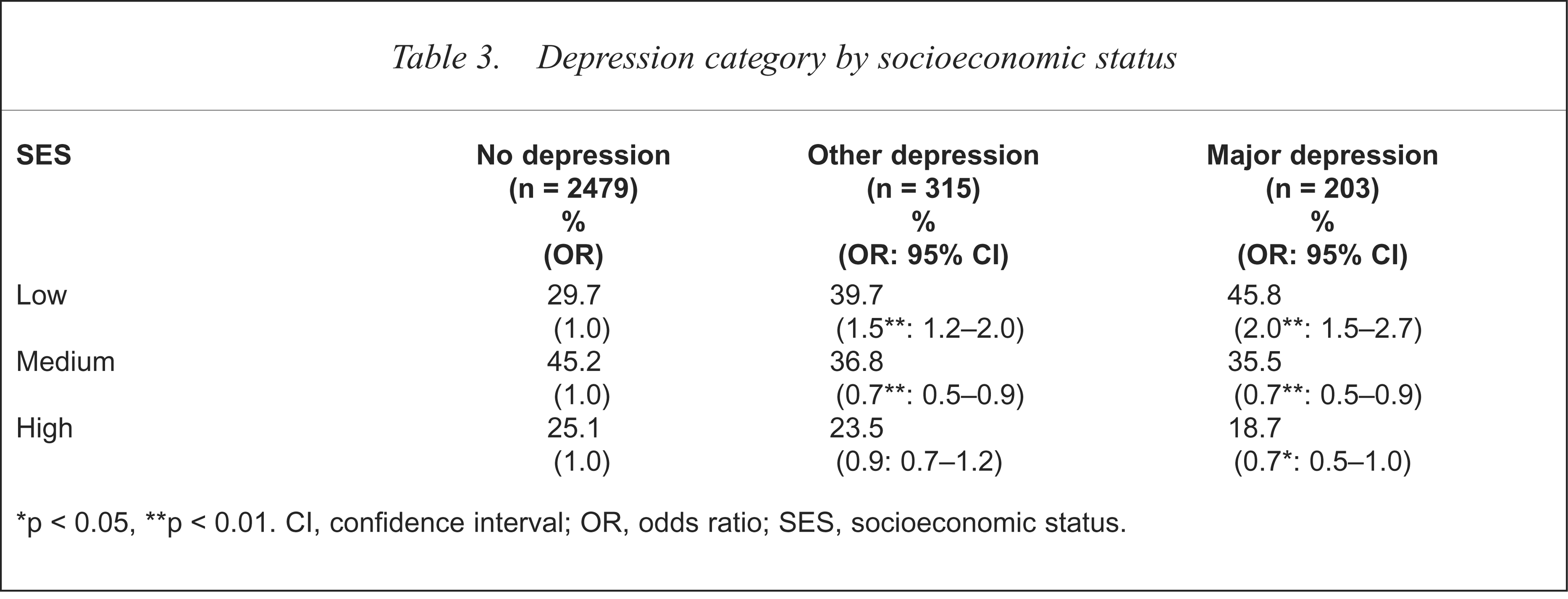
p < 0.05,
p < 0.01. CI, confidence interval; OR, odds ratio; SES, socioeconomic status.
The results of the SF-36 analysis are presented in Fig. 1. For each SF-36 subscale scores are shown for each of the depression categories compared with South Australian norms. Those with major depression scored significantly worse in terms of functioning for all dimensions than those with other depressions and those who were not depressed. The effect size for the major depression group can be described as large to very large [19]. Those with major depression scored lower than the 27th percentile on all dimensions, and as low as the 4th percentile on the mental health dimension. Once again, those with other depressions scored at an intermediate level of health-related quality of life.
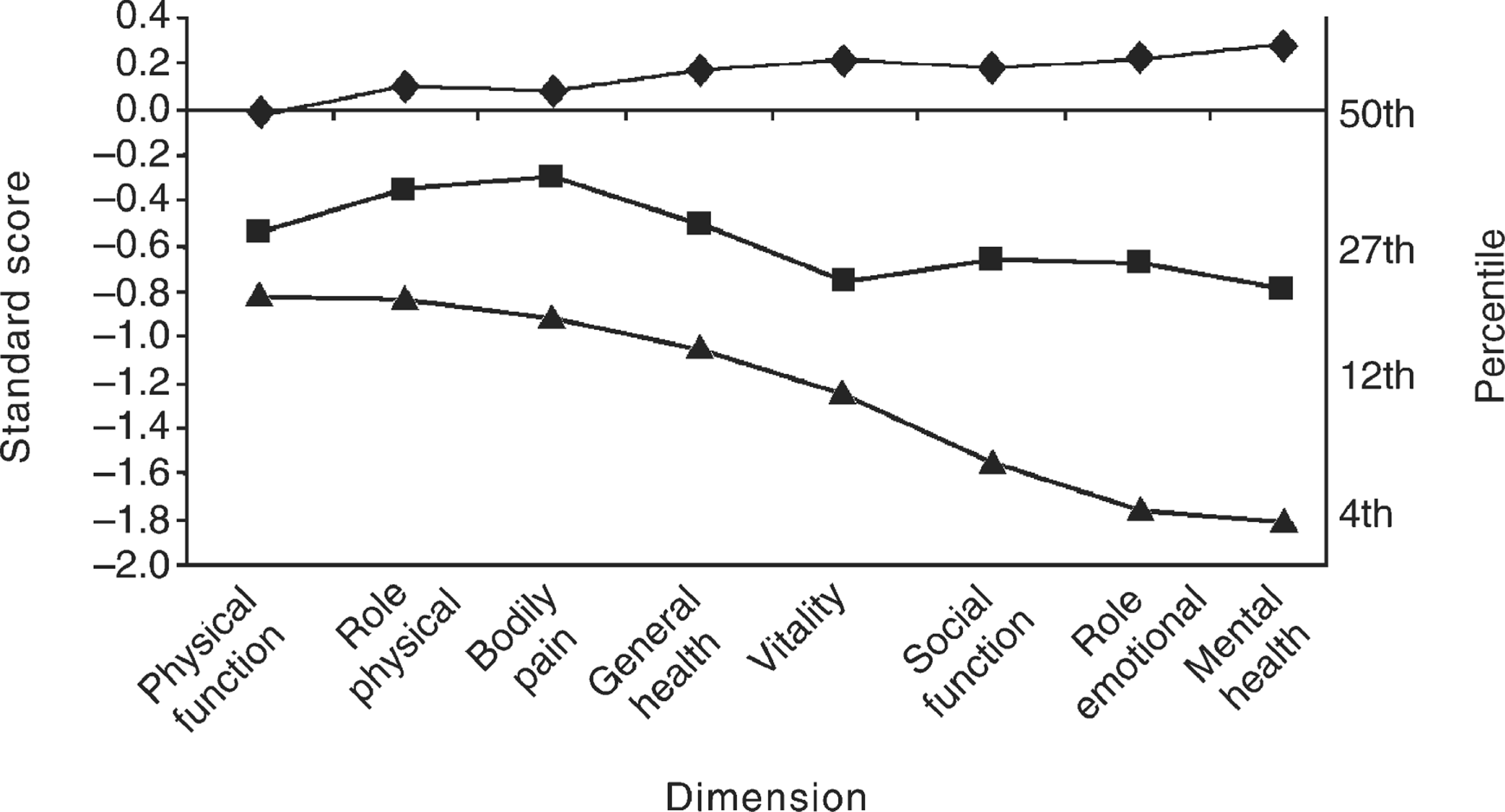
Short-form Health Status Questionnaire standard scores controlling for age, sex and socioeconomic status for people with no depression (n = 2486), other depressions (n = 319) and major depression (n = 205) compared with the general population. Standard score of 0.0, corresponding to 50th percentile, represents the general population. ▴, major depression; ▪, other depressions; ♦, no depression.
The AQoL results are presented in Fig. 2 with standard scores for each of the depression groups compared with the general South Australian population. There were significantly poorer utility scores on all dimensions for those with major depression compared with those with other depressions and those not depressed, except for the physical senses scale which showed no difference between major depression and other depressions. Compared with the general population, those with major depression scored lower than the 12th percentile on the overall AQoL utility score as well as on the social relationships and psychological wellbeing dimensions. Again, the effect size for the major depression group can be described as large to very large [19].
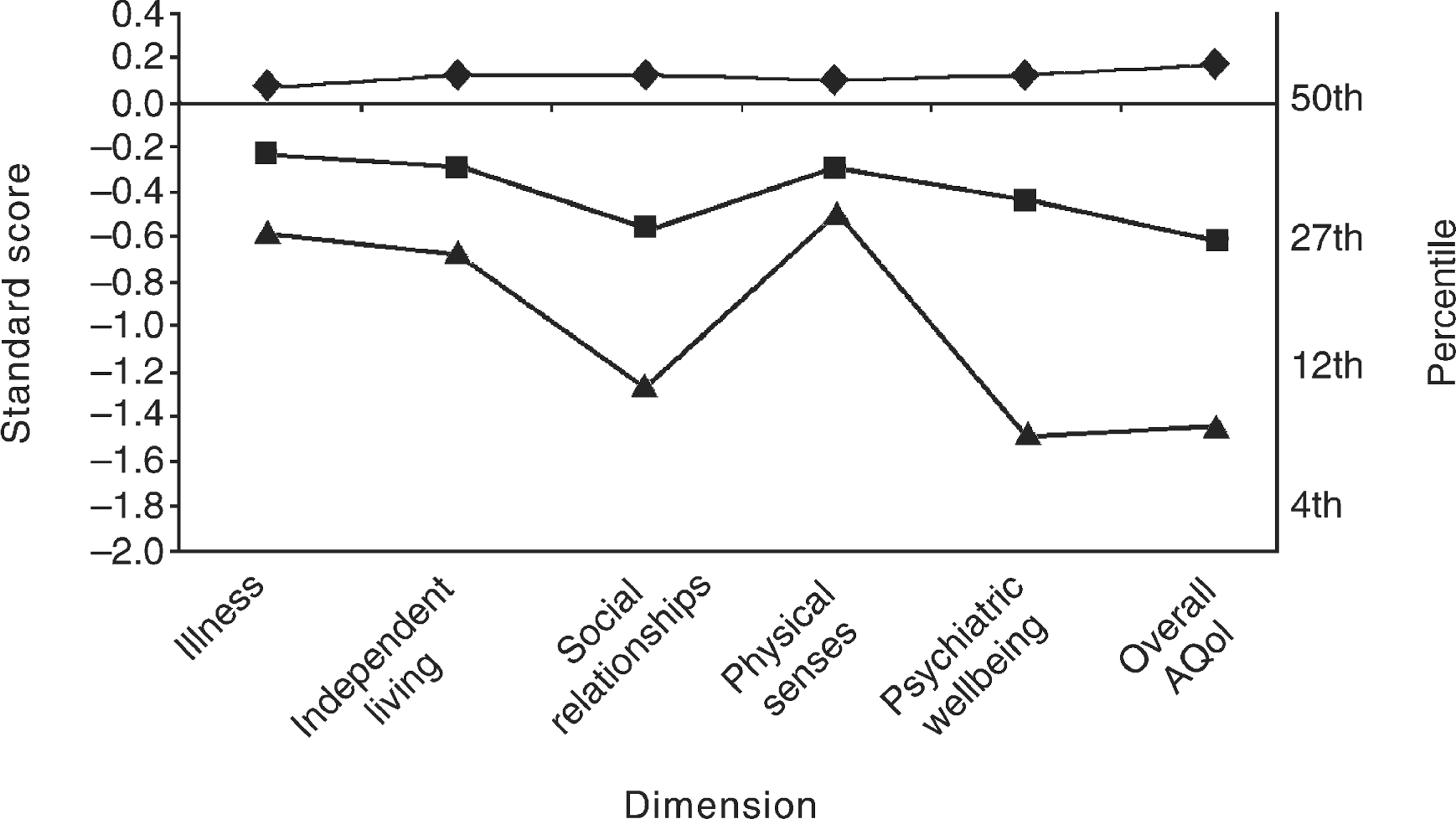
Assessment of Quality of Life standard scores controlling for age, sex and socioeconomic status for people with no depression (n = 2486), other depressions (n = 319) and major depression (n = 205) compared to the general population. Standard score of 0.0, corresponding to the 50th percentile, represents the general population. ▴, major depression; ▪, other depressions; ♦, no depression.
Discussion
These results, in a random and representative sample of the South Australian population, further substantiate the high level of morbidity associated with major depression reported in the Global Burden of Disease study [1], the Australian Burden of Disease and Injury report [3] and National Survey of Mental Health [4,5] and in clinical research [6–8]. Those in the community who were identified as having major depression had a considerable degree of morbidity, as indicated by their higher use of health services and by the amount of time they were unable to pursue their work or normal activities. They were also more likely to be living in areas of socioeconomic disadvantage. Furthermore, they had a markedly diminished level of physical and mental functioning and quality of life, as determined by their scores on validated measures. Indeed, these associations raise the possibility that these various burdens may also contribute to depression itself.
Those with major depression were most compromised in three dimensions of the SF-36: general mental health (a measure of the time the person was experiencing feelings of nervousness, anxiety and depression), role limitation due to emotional health problems preventing usual activities, and vitality (energy level). These findings are consistent with lower functional status on the SF-36 shown in other depression studies [20–22]. Thus, Reifler et al. reported that patients who screened positively for any mental disorder had markedly lower functional status than those screening negatively on all eight SF-36 subscales, and had greater utilisation of health services [20]. More specifically, Coulehan et al. found that major depression was associated with significant physical, psychological and social impairment, as measured by the SF-36 [21].
Similar findings were evident for the AQoL measure, particularly for the illness, social relationships and psychological wellbeing dimensions, as well as the overall score. For the major depression group the illness dimension showed greater use and reliance on medications and treatment, while the social relationships dimension indicated poor functioning in general as well as being compromised specifically due to the person's health.
Clearly, whichever measure is used, the personal burden of depression, let alone the economic cost to the community, is considerable. For example, the magnitude of the economic cost and the potential benefit of treatment of depression to the community can be gauged by considering the following scenario. For those with major depression, if adequate treatment could reduce the average 4.4 days per month inability to pursue usual work and other activities by just 2 days, if productivity were assumed to be $100 per day, and if one extrapolated from the 158 with major depression of those 2180 aged between 18 and 59 in the present 3010 subjects to the approximate 10.3 million persons Australia wide in the same age group who would be eligible to work [23], and assumed that only 60% of those would be in paid employment, then the community would be about one billion dollars better off in terms of productivity regained.
It is acknowledged that these figures do not take into account a number of other potentially confounding variables. Nevertheless, they are based on conservative estimates, and the enormity of the impact of depression on the community cannot be denied. A more detailed economic evaluation is soon to be undertaken, including a recent development of the AQoL which allows for the conversion of AQoL to DALY scores [24].
The cost of depression has been reviewed comprehensively in a recent World Psychiatric Association publication [25] which addressed both the direct and indirect costs upon individuals and society. It has been acknowledged that initial direct health-care costs would increase with more intensive programs of depression management [26]. However, there are persuasive data at the population level which confirm not only an improvement in the diagnosis and treatment of depression following educational programs, but also a community economic benefit [27]. Indeed, in supporting the need for an evidence-based approach, it has been noted that it may only be by increasing direct health-care costs that effective treatment will be achieved, thereby optimising health gains with a concomitant economic advantage to the community [26].
It is pertinent to reflect on the fact that although there are effective treatments for major depression, and although 69.3% of those with major depression had consulted general practitioners and 10.6% had consulted psychiatrists, only 19.5% of them were currently taking antidepressants, a figure very similar to the 18% reported in a large European survey [28]. These findings are consistent with previous reports of the less than adequate management of depression in general community groups [29,30] and in specific groups such as those at risk for suicidal behaviour [31,32].
Antidepressants are not the only treatment for major depression, and it may well be that other effective therapy such as cognitive–behavioural treatment was being used. In addition there is debate about the treatment effect size of antidepressants and the burden of side-effects [33]. Indeed, in our results it is of interest that although one-fifth (19.5%) of those with major depression were taking antidepressants, an identical proportion had had antidepressants in the past, with 39% stating that they had ever had such medication. This raises the question of why they were not being used at the time of assessment. Perhaps side-effects, lack of previous benefit or some other factors were operating to inhibit their current use.
Methodological shortcomings in the present study should be acknowledged. The PRIME-MD has previously been used as a primary care screening instrument, rather than in a general population sample. The recent Australian National Survey of Mental Health [3] reported a lower 12 months' prevalence of 5.8% for ‘depressive disorders’ based on ICD-10 diagnosis, although the 6.8% current (2 week) prevalence of major depression in this study is of the same order as other community studies using different methods of detection of major depression [34–39]. Nevertheless, we are mindful of the problems in defining clinical significance in epidemiological studies [40], and the fact that the detection of ‘case-ness’ in such studies does not necessarily equate with the need for treatment [41]. However, it can be asserted that those who were defined as having major depression using the PRIME-MD in this study had had significantly more treatment from a number of different professionals. They also had a greater degree of morbidity in their ability to pursue daily activities and work and they were markedly compromised in terms of their social functioning and quality of life.
There appear to be no specific concerns with the use of the SF-36 as it has been validated in several studies in Australia and local norms have been published [12–14]. However, the AQoL is less well established as a research instrument, although further reliability and validity data have been reported [15] and it is being refined further [24].
Notwithstanding these potential shortcomings, we consider that these South Australian results add to the increasing literature which has demonstrated the considerable burden that depressive illnesses, particularly major depression, impose on the community. They are also consistent with previous reports of shortcomings in the overall management of major depression and, clearly, there is the potential for improved health outcomes for those affected. Economic pressures from rising health-care costs and consumer expectations combined with the increasing societal burden of depression (a burden not distributed equally in the community) make it imperative that more research is conducted to demonstrate the cost-effectiveness of treatments for depression and allow for better estimates of the potential for reducing the burden.
Acknowledgements
This study was supported by grants from the University of Adelaide, Pfizer, Bristol-Myers Squibb Australia and Wyeth Australia. It was also made possible because of the South Australian Health Omnibus Survey conducted by the South Australian Department of Human Services Centre for Population Studies. Assistance with data analysis was provided by Catherine Chittleborough.