
Abstract
The Personal Assessment and Crisis Evaluation (PACE) Clinic was established in 1994 to develop strategies for the identification of young people at imminent risk of developing a psychotic disorder and to develop interventions for this ‘ultra-high’ risk (UHR) group which will prevent or delay the onset of illness. As the PACE Clinic was the first clinical research program to attempt to intervene in the early stages of psychotic disorders before diagnostic criteria are met, criteria for the identification of the UHR population needed to be developed from first principles. The present paper describes the development and validation of criteria for identifying the target group.
The prevention of psychotic disorders such as schizophrenia is obviously a worthwhile goal. These disorders have historically been associated with huge costs for the sufferer, their family and friends, and society at large [1]. Progress in this area was hampered for a long time on two fronts: (i) who should be the target of preventive interventions; and (ii) what would constitute an appropriate preventive approach? Obviously the issue of identifying the target UHR group had to be addressed first and this was the early objective of research at PACE. We have since moved into the development of preventive interventions for the UHR population [2].
The problematic concept of the psychotic prodrome
A prodromal state commonly precedes the acute phase of a psychotic episode. This phase of mental state change from premorbid state to the onset of frank psychotic symptoms typically extends for an average of 2–5 years [03–05] and is associated with significant levels of psychosocial impairment and disability. A broad range of symptoms has been attributed to this phase of illness from attenuated or low-grade psychotic symptoms, which are immediately suggestive of an emerging psychosis, to nonspecific symptoms such as sleep disturbance and amotivation [6].
DSM-III-R [11] prodromal symptoms for schizophrenia
Some prospective approaches to designing preventive interventions are equally impractical. Largescale, population-based preventive measures would be very costly and of dubious ethical standing, given the low base rate of these disorders in the population. A natural alternative would be to focus on people who, for various reasons, are thought to have increased risk of developing these disorders. The most obvious target group is individuals with a family history of disorder. Various studies have been conducted that monitor people with a family history of illness over time from childhood with the aim of detecting the onset of psychotic disorder if it occurs [12–15]. Such ‘high risk’ studies are also costly and the transition rate to psychosis may not be very high. Additionally, the development of psychosis is not limited to individuals with a family history of disorder.
A second approach has been the development of instruments for detecting subtle changes in thinking style and perceptual change, which may be precursors of frank psychosis [16–18]. The predictive utility of these scales, however, has not been adequately assessed to date.
Indicated prevention
In light of the difficulties mentioned earlier, our group decided to try another approach to identifying people at risk of psychosis. In the early 1990s a reformulation of the principles of intervention in psychiatric disorders was developed from the earlier ideas of Gordon [19], with particular emphasis on preventive interventions [20]. Within this reformulation of prevention, Mrazek and Haggerty noted that: ‘The best hope now for the prevention of schizophrenia lies with indicated preventive interventions targeted at individuals manifesting precursor signs and symptoms who have not yet met full criteria for diagnosis. The identification of individuals at this early stage, coupled with the introduction of pharmacological and psychosocial interventions, may prevent the development of the full-blown disorder’ (Mrazek and Haggerty, 1994, p. 154 [20], emphasis added). Indicated prevention was defined as ‘interventions … targeted to high-risk individuals who are identified as having minimal but detectable signs or symptoms foreshadowing mental disorder or biological markers indicating predisposition for mental disorder, but who do not meet … diagnostic levels at the current time’ (Mrazek and Haggerty, 1994, p. 154 [20]). With this in mind we set out to develop criteria to identify people in this high-risk symptomatic category. Thus, the anticipated time period to psychosis transition in the UHR population is much shorter than in traditional high-risk studies (i.e. New York High Risk Project [21] and Edinburgh High Risk Study [22]).
A ‘close-in’ strategy [23] was adopted to direct the development of intake criteria for the PACE Clinic. Essentially this means combining known risk factors to ‘close in’ on the target population. At this stage it should be noted that the PACE Clinic intake criteria are geared towards identifying young people at risk of developing psychosis, not simply schizophrenia. This is largely due to research indicating the high degree of ‘diagnosis shift’ that is associated with first-episode psychosis as the disorder progresses [24],[25]. Attempting to identify young people at risk of schizophrenia alone may therefore be short-sighted.
When attempting to identify a specific target population in a prospective manner, it is to be expected that some ‘false positives’ and ‘false negatives’ will be identified unless the identifying criteria have 100%% specificity and sensitivity (Fig. 1). With this in mind, we consider our criteria as identifying an ‘at risk mental state’.
At-risk mental state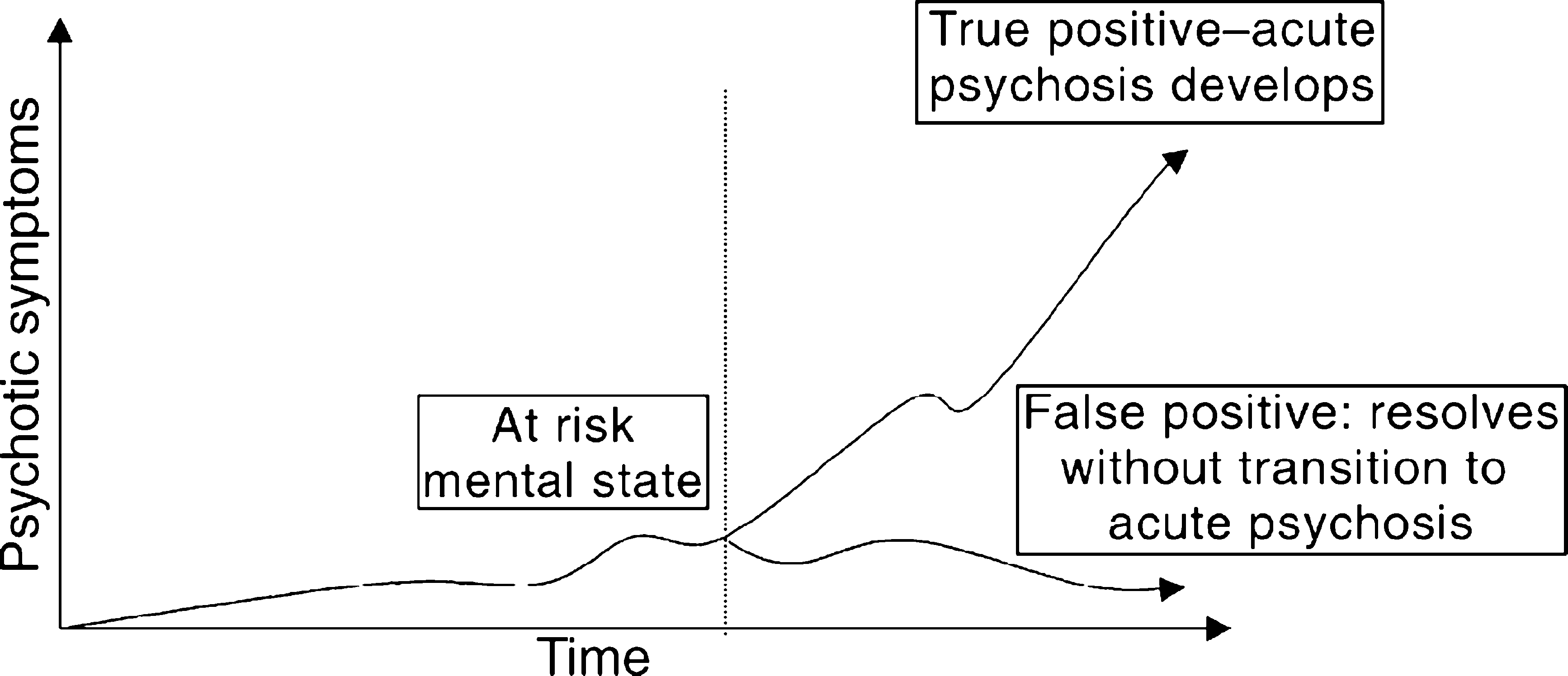
‘At-risk mental state’ criteria
As mentioned earlier, clinical observation and retrospective research informed the development of the ‘at-risk mental state’ criteria. Two strategies informed the development of this knowledge into criteria that had a practical application.
The first strategy aimed to identify young people reporting mental state changes indicative of a possible psychotic prodrome. To reduce the likelihood of false positives being identified, nonspecific mental state changes such as depression, sleep disturbance or anxiety, were not included within this criteria. Instead the criteria focus on either low-grade or attenuated positive psychotic symptoms (the ‘attenuated’ group) or brief bursts of frank psychotic symptoms lasting less than a week and spontaneously resolving (the Brief Limited Intermittent Psychotic Symptoms (BLIPS) group).
The second strategy was one of combining trait risk factors of psychosis (a family history of psychotic disorder or a schizotypal personality disorder in the identified individual) with a mental state change that has lasted for at least a month and is associated with clear functional deterioration. This group is known as the ‘vulnerability’ group.
Two early studies conducted at the PACE Clinic are described below. The primary aim of these studies was to validate the ‘at-risk mental state’ criteria.
Study 1: Pilot Study
Pilot Study intake criteria
Twenty-one young people meeting ‘at-risk mental state’ criteria were monitored over a 24-month period, seven of whom developed a psychotic disorder over the follow-up phase. The Pilot Study was considered a precursor of a more ‘enriched’ study of prediction of transition with a broader range of variables. It enabled the case-finding mechanism and clinical structures of the PACE Clinic to be developed and tested; a familiarity with the clinical needs of the client group to be obtained; and the criteria to be reviewed and amended ([29]; McGorry PD et al., unpubl. data,). The 33%% transition rate to psychosis in the identified group within 24 months was an encouraging start. The study is presented in more detail in an earlier paper [29].
Study 2: Prediction Study
Prediction study intake criteria
Operationalised criteria for identifying onset of acute psychosis
Forty-nine young people meeting criteria for one or more of the intake groups listed in Table 3 were recruited to the study. Their mental state was monitored over the course of the following 12 months to determine the rate of transition to psychosis (identified according to the criteria given in Table 4). Forty-one percent of these young people developed a psychotic disorder within a year of recruitment, which indicates that the changes to the intake criteria between the Pilot and Prediction studies had enhanced the ability to identify the UHR population.
Discussion
The results of the two studies presented indicate that it is indeed possible to identify young people at risk of imminent psychosis with a relatively high degree of success. The rate of transition to psychosis of young individuals in the Prediction Study may still increase as they pass through the entire period of risk.
This is obviously the first step, albeit a crucial one, towards the prevention of psychosis. Many other steps along the way can be identified. The first is recruiting young people meeting these criteria to preventively orientated services. At PACE we have identified over 500 young people describing ‘at-risk mental state’ characteristics over the past 5 years – many of whom have consented to take part in research at the Clinic. We have cast our net wide to educate the youth, health and education sectors in the Melbourne metropolitan area of our existence and services we can offer to attract referrals [33]. More importantly, this approach to identifying the UHR population has been adopted in other sites within Australia (i.e. Psychological Assistance Service in Newcastle) and overseas (i.e. Prevention through Risk Identification, Management and Education, or PRIME, at Yale).
Second, the validity of other putative risk factors of psychosis that may serve to enhance identification of the UHR population needs to be assessed. As briefly described earlier, neurocognitive assessment and neuroimaging are included in the research protocol at PACE for this reason. Other potential screening factors include neurological soft signs [34] and minor physical abnormalities [35],[36]. Finally, appropriate preventive interventions obviously need to be developed and evaluated.
Footnotes
Acknowledgements
Colleen McFarlane, Mats Hallgren, and the late Arun Rakkar for assisting in recruiting and monitoring the PACE UHR cohorts. This research and the clinical research structure of the PACE Clinic were supported by project grants from the National Health & Medical Research Council, the Victorian Health Promotion Foundation Program grants, the Stanley Foundation and the Victor Hurley Research Foundation.