
Abstract
Cannabis is the most widely used illicit drug among individuals with psychotic disorders [1–3]. Estimates of the prevalence of cannabis use in studies of psychotic patients published from 1990 to today vary widely. One study reported that the prevalence of lifetime cannabis abuse in this group is 8% [2] while another has estimated that 86% of inpatients with psychosis have experimented with cannabis over the course of their lifetime [4].
Intoxication following cannabis ingestion has been associated with transient psychotic symptoms such as paranoid ideation, auditory or visual hallucinations, depersonalization or derealization in a significant percentage of cannabis users [5–7]. The relationship between cannabis use and the development of a psychotic disorder is less clear.
The strongest evidence linking cannabis use with the onset of a psychotic illness involves over 45 000 Swedish army conscripts. After controlling for other predictors such as psychiatric diagnosis, parental divorce, alcohol and solvent use, this study found that heavy cannabis use was a significant, if relatively modest, risk factor for the subsequent development of schizophrenia in the subject group [8]. One interpretation of these results is that heavy cannabis use may increase the risk of later development of psychosis [6, 9]. The role of other factors in explaining the link between cannabis use and psychotic disorders in this study, such as premorbid personality, adverse peer relationships, childhood adversity or social disadvantage was neglected in the study and cannot be dismissed [10–13]. It is also noted that the average duration of follow-up of this cohort was 15 years with schizophrenia developing at any time during this period. Therefore, the study provides information relating to the long-term impact of cannabis use on the development of schizophrenia but does not provide a great deal of information about cannabis use as a proximal risk factor. Nevertheless, this is the best study to date suggesting a link between cannabis use and psychotic illness.
Once a psychotic illness has been established, it seems likely that cannabis use, particularly if moderately heavy, can contribute to the exacerbation or maintenance of the existing disorder. Various studies have reported that ongoing cannabis use is associated with relapse of illness, greater intensity and duration of psychotic symptoms and increased frequency of hospitalization [14–17].
An alternative explanation for the association between cannabis use and psychosis is that the onset, maintenance and escalation of cannabis use could itself be a consequence of psychotic illness – the level of cannabis use might increase in response to positive symptoms and play a contributory causal role in further exacerbating symptoms [18]. This ‘self-medication’ hypothesis is not supported by evidence that substance use generally commences prior to the onset of positive psychotic symptoms [19–21]. It is acknowledged, however, that negative symptoms often predate the emergence of positive symptoms, and individuals in this stage of illness could be attempting to address negative symptoms.
The current study investigated the association between baseline level of cannabis use and psychotic status one year later in a group of individuals at known very high risk of early conversion to psychosis. It was hypothesized that cannabis use would constitute a risk factor for conversion to acute illness in the year after recruitment to the study.
Method
Setting
The Personal Assessment and Crisis Evaluation (PACE) Clinic is a specialist clinical research program for adolescents and young adults at ‘ultra’ high risk (UHR) of developing a psychotic disorder [22–26], taking referrals from the health, education and welfare services within the Melbourne metropolitan area. This study is a component of a large programme of research addressing issues of identifying young people at high risk of psychosis, characterizing the transition from high risk to acute psychosis and developing appropriate preventive interventions for this population [22–24]. Local research and ethics committees approved the design and aims of this study.
Subjects
Subjects were recruited into this study from consecutive admissions to the PACE Clinic. All referrals to the Clinic between March 1995 and January 1999 were screened for inclusion. The rationale and history of the development of the PACE Clinic as well as the referral and screening process associated with the Clinic have been described in a number of earlier publications [24–31]. Essentially the UHR subjects must meet at least one of the following groups: (i) Trait and State Risk Factor Group (have a first degree relative with a psychotic disorder or the identified patient has a schizotypal personality disorder in addition to a significant decrease in functioning during the previous year); (ii) Attenuated Psychotic Symptoms Group (have experienced subthreshold, attenuated forms of positive psychotic symptoms during the past year); or (iii) Brief Limited Intermittent Psychotic Symptoms Group (have experienced episodes of frank psychotic symptoms that have not lasted longer than a week and have been spontaneously abated). Subjects must also be aged between 14 and 30 and have not experienced an acute psychotic episode or taken neuroleptic medication. Operationalized criteria for the three intake groups are listed in Table 1.
Personal Assessment and Crisis Evaluation Clinic intake and acute psychosis criteria
The main outcome measure in this study was the development of psychosis according to criteria listed in Table 2. No subject included in this paper received antipsychotic medication unless acute levels of psychotic symptoms developed. All subjects received supportive psychotherapy and case-management depending on their needs.
Acute psychosis criteria developed by the Personal Assessment and Crisis Evaluation Clinic
Procedure
Potential subjects were assessed via a detailed clinical interview conducted by a consultant psychiatrist, a psychologist or both to determine whether they met intake criteria. All of these assessments were discussed at a consensus meeting at which at least one consultant psychiatrist was present. Subjects who met intake criteria were then approached regarding involvement in a study monitoring their clinical status, particularly focusing on the development of acute psychosis, over the subsequent 12-month period. Twelve months was chosen as the minimal follow-up period because a previous study of young people meeting UHR criteria has indicated a transition rate to acute psychosis of 40% in the first 12 months after recruitment and a decline in rate of transition after this [31]. The ‘psychotic status’ of some subjects after the initial 12-month period is known and longer term follow-up of all participants is anticipated. If acute levels of psychotic symptoms developed at some stage during the 12-month monitoring period, however, follow-up was ceased and appropriate treatment including antipsychotic medication was commenced. Once again this decision was confirmed by discussion at a consensus meeting at which a consultant psychiatrist was present. The duration of follow-up ranged from 4 to 1051 days with an average of 319.8 days (SD = 198.3).
For the purposes of this paper, cannabis dependence was defined according to DSM-IV criteria [32], utilizing the SCAN diagnostic instrument [33].
Statistical analysis
The statistical software SPSS for Windows 9.0 (SPSS, Chicago, USA) and S-PLUS for Windows 4.0 (MathSoft, Seattle, USA) were used to carry out the following analyses. The χ 2 test was used to assess if different categories of a variable differed in terms of the proportion of UHR subjects becoming psychotic within one year. Survival analysis was also applied to each variable to test for the association between a particular variable and the risk of psychosis, taking into account time to psychosis.
Throughout the study, results were considered statistically significant when the corresponding p-value was 0.05 or less by two-tailed analysis.
Results
Intake characteristics
Mean age at first assessment of the 100 UHR subjects included in this study was 19.3 (SD = 3.5, range 14–28). Forty-nine of the subjects were male (49%). A range of scales was used to assess aspects of psychopathology and functioning at baseline. The mean (and SD scores) of 60.7 (14.0) and 75.5 (22.9), respectively, for the Global Assessment of Functioning [32] and Quality of Life Scale [34] indicate a significant level of impairment in global functioning. The cohort also reported moderate levels of global psychopathology (Brief Psychiatric Rating Scale [35]: mean 19.6, SD = 8.9). This is reflected in the mean Hamilton Rating Scale for Anxiety [36] and Hamilton Rating Scale for Depression [37] scores of 14.2 (7.5) and 17.2 (9.1), respectively (SD in brackets). Finally the mean score on the Scale for the Assessment of Negative Symptoms [38] was 18.5 (SD = 13.8).
The distribution of the UHR subjects between the three intake groups is shown in Figure 1.
Number of subjects meeting each intake criterion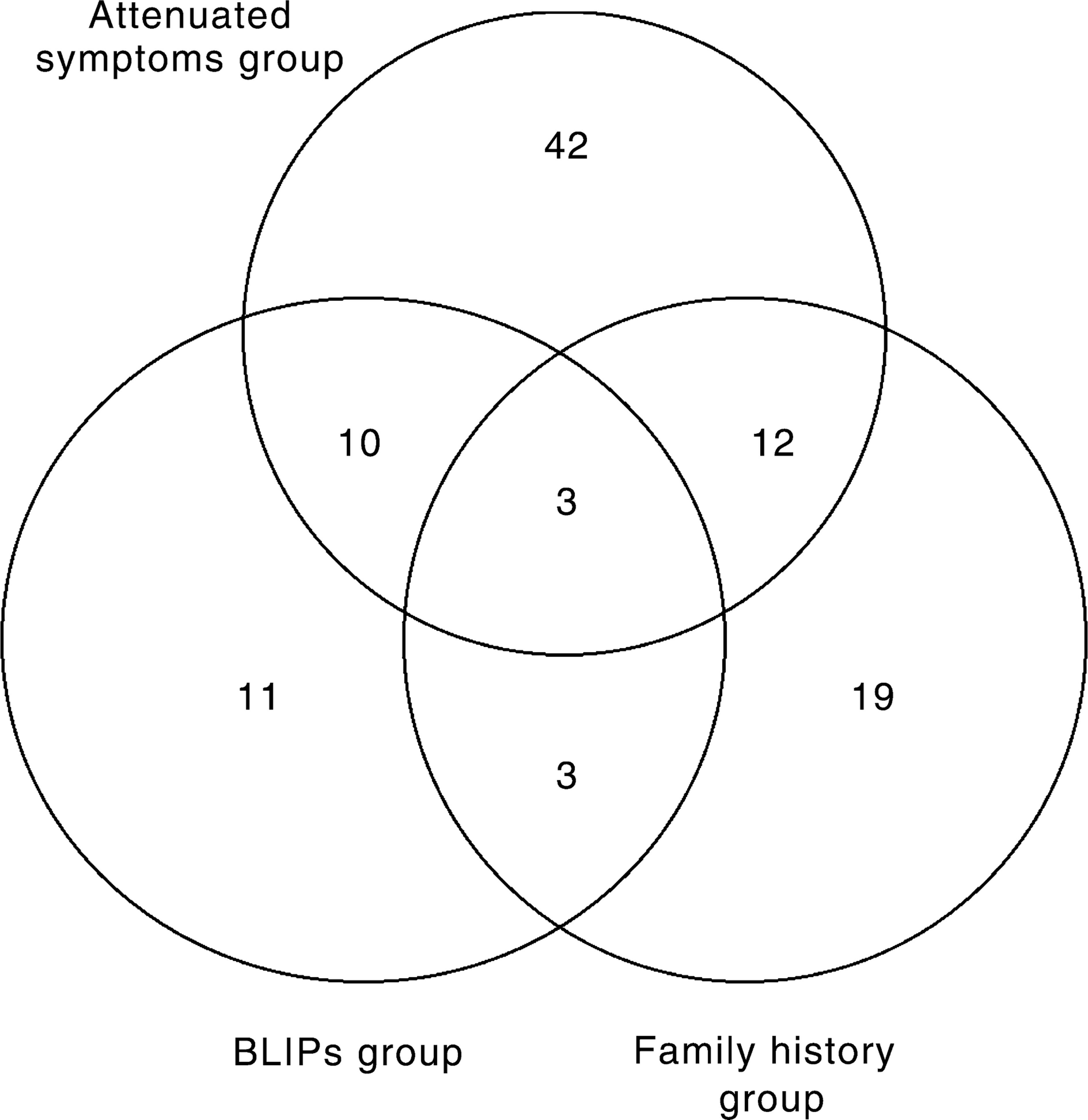
Transition to psychosis
At 6 months after intake, 24 of the 100 subjects (24%) had developed psychosis. By 12 months this had increased to 32 of the 100 subjects (32%). Another 5 subjects are known to have developed an acute psychosis after the initial 12 month follow-up period. All of these subjects have subsequently been treated with antipsychotic medication. As indicated earlier, the entire sample has not yet been followed up further than the initial 12-month period and there may be further cases still with psychosis onset after that point. It is anticipated that the relationship between cannabis use and development of psychosis after the initial 12-month period will be the subject of future analysis.
Substance use
At the time of entry to the study, 42 (42%) of the sample of 100 UHR subjects reported never using illicit drugs and 10 subjects (10%) said that they had used substances only once or twice in their lifetime. Eighteen (18%) met the criteria for a diagnosis of DSM-IV cannabis dependence in the previous year with 22% of subjects using cannabis at least once a month in the year prior to assessment. Data regarding cannabis use and other drugs is reported in Table 3. The use of drugs other than cannabis prior to recruitment to the PACE Clinic was minimal by this cohort and as a result was not included in any further analysis.
Drug use by the ultra high risk cohort (n = 100)
Thirty-five UHR subjects had used cannabis in the previous year, 13 of who (37%) became psychotic within one year. Of the remaining 65 subjects, 19 developed psychosis within 12 months (29%). Such a difference in rate of transition to psychosis between cannabis users and non-users was not statistically significant (χ 2 (1) = 0.65, p = 0.42).
A similar comparison of cannabis dependence indicated that, of those 18 subjects who had a diagnosis of cannabis dependence in the previous year, 7 (39%) became psychotic within one year. Twenty-five (31%) of those who were not dependent on cannabis became psychotic within a year. Once again, the difference in transition rate to psychosis was not significant (χ 2 (1) = 0.48, p = 0.49).
Cannabis use was further divided into ‘no use’ in previous year, ‘less than weekly use’ and ‘at least weekly use’. (This categorization was decided upon after a preliminary scanning of the frequency of use data). When dividing cannabis use this way, 19% of the total sample had used cannabis at least once but less than weekly in the year prior to recruitment and 37% of these subjects subsequently developed psychosis. Sixteen per cent of the sample had used cannabis at least weekly and 38% of these developed psychosis. There were no significant differences in the rates of transition to psychosis between the groups when divided according to frequency of use (χ 2 (2) = 0.66, p = 0.72).
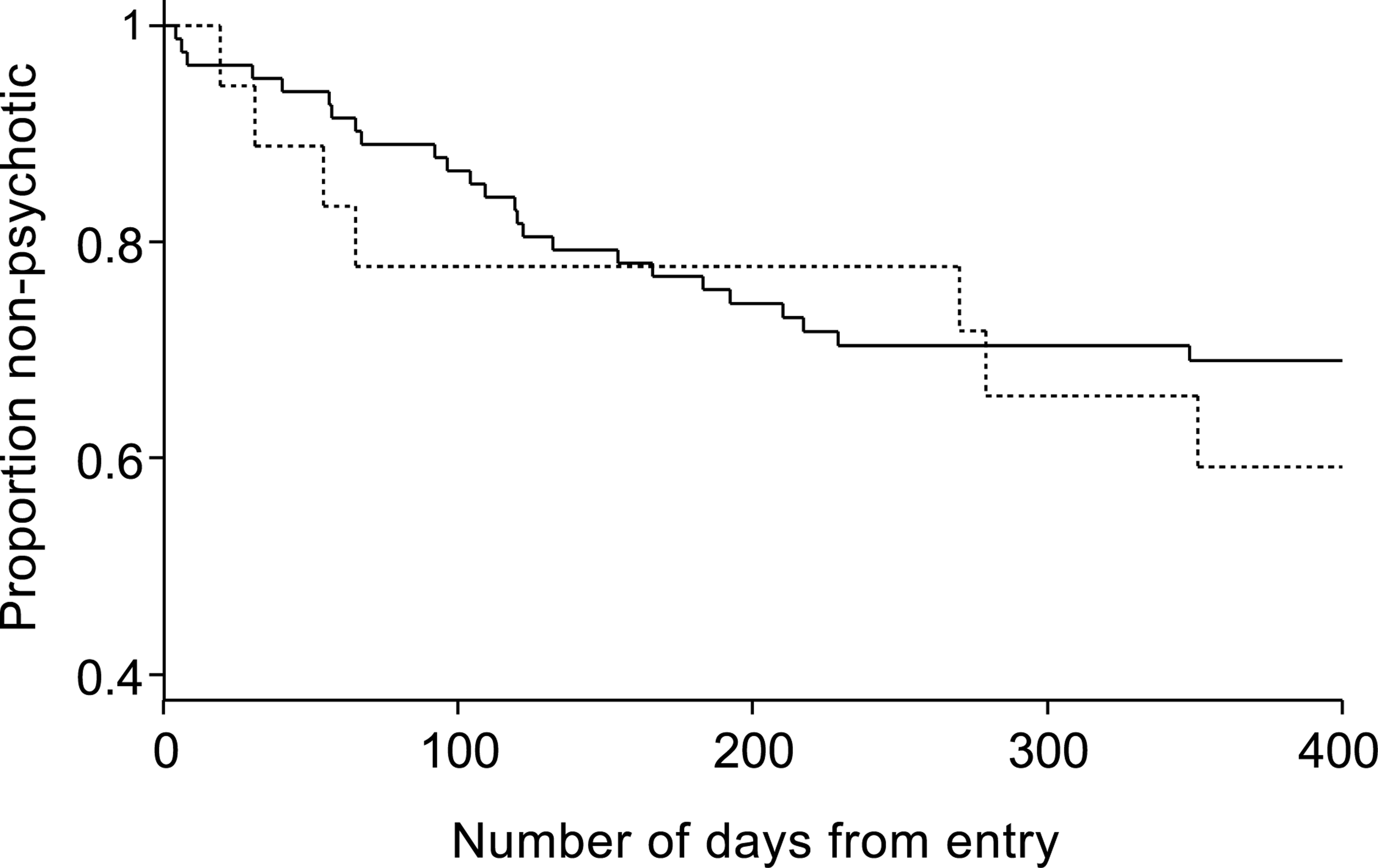
The previous analyses regarding transition to psychosis do not fully utilize the available information – in particular the time to onset of acute psychosis. To address this, survival analysis was applied: Kaplan–Meier survival curves were produced and the log-rank test was carried out. However, even when using this test, there was no indication of higher risk of onset of psychosis in those individuals who had used cannabis in the previous year than those who had not (p = 0.51). Additionally, those who were cannabis dependent in the previous year were not at significantly greater risk of becoming psychotic than those who were not (p = 0.52). The relevant survival curves are shown in Figures 2 and 3.
Survival curves: proportions remaining nonpsychotic for cannabis users and non-users in previous year. (—) no; (– – –) yes. Log-rank test: p-value = 0.51. Survival curves: proportions remaining nonpsychotic for cannabis dependent and non-dependent subjects in previous year. (—) no; (– – –) yes. Log-rank test: p-value = 0.52.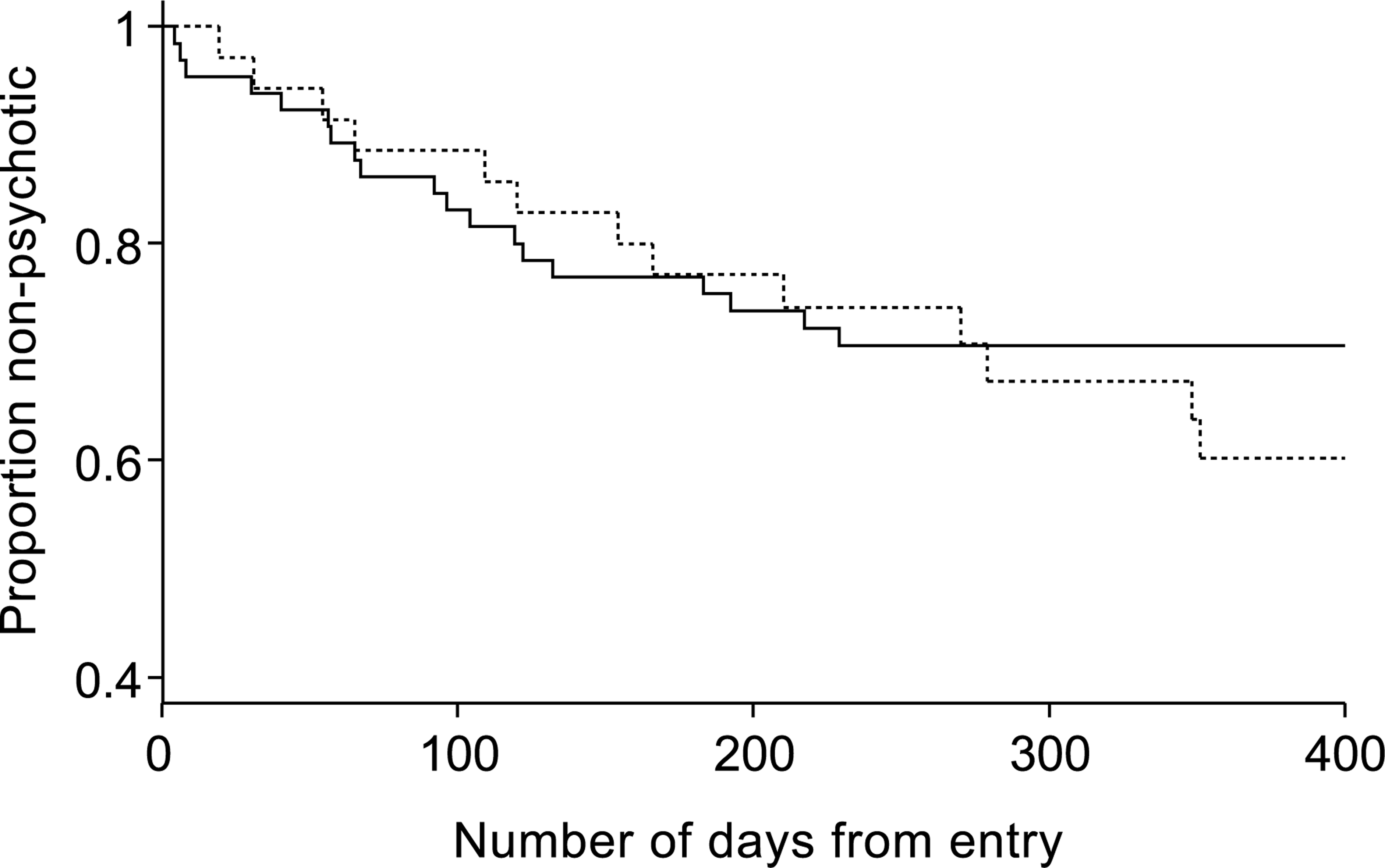
Discussion
The most important finding of this prospective study of individuals at high risk of developing a psychotic disorder is that neither cannabis use nor dependence in the year prior to recruitment to this study contributed to the risk of developing psychosis. This finding was not confounded by the effects of other substance abuse or dependence, or by the effects of antipsychotic medication (not used at all in this cohort of patients).
This study is unique in that it is the first to utilize a ‘close-in’ strategy to demarcate a group of individuals at ‘ultra’ high risk for the development of a psychotic disorder and to observe the effects of antecedent cannabis use on the eventual psychotic status of those individuals. Although Andreasson and colleagues [8] prospectively observed the likelihood of the development of a psychotic disorder from baseline substance use, that study did not directly observe the emergence of psychotic symptoms – the mean duration of follow-up in that study was 15 years. The present study assessed evidence of an association between the two variables that is temporally more proximal: that is, the emergence of a psychotic disorder within one year of cannabis use.
While this study does not support a role for cannabis in the development of first-episode psychosis, we cannot conclude that cannabis use should be completely ignored as a candidate risk factor for onset of psychosis, one which is potentially malleable. Individuals who presented to our service setting are almost certainly not representative of all young people who eventually develop a psychosis. The UHR cohort, all of whom voluntarily presented for assessment and follow-up due to concern about changes in their functioning or perceptual experiences, are thought to be a distinctive subgroup of the high-risk population.
The levels of substance use in this group were generally relatively low compared to reports of high levels of substance use by early psychosis cohorts reported elsewhere [16, 39–41]. Thirty-seven percent of the UHR cohort reported having used cannabis at least once in their lifetime and 18% met diagnostic criteria for cannabis dependence compared to rates of dependence of 20–30% in recent onset cases reported in studies over the last 10 years [16, 39–41]. A heightened level of concern for their own mental health might be associated with lower levels of cannabis use by the UHR cohort, although this is only speculation.
It may be that other UHR individuals who do not present to this service, but who ultimately develop psychosis, use cannabis at much higher levels, and the contribution of cannabis to onset of psychosis is substantially greater than seen in this sample. Should this prove to be the case, it may be possible to reduce the risk of development of psychosis in vulnerable young people through interventions aimed at encouraging the reduction of cannabis use. A randomized trial of psychological interventions targeting cannabis use by first-episode psychosis patients that is currently underway may provide guidelines for the treatment approaches that may be utilized with UHR patients [42].
Although the rates of cannabis use in this UHR sample are lower than those of first-episode psychosis patients they appear to be higher than the general population. Recent reports state that 6% of 18–24 years olds in the Australian population are dependent on cannabis [43], while 25% of 13–17 years olds have used cannabis at least once and 11% have used it 10 times or more [44]. Other premorbid issues such as social withdrawal, negative affect or lowered mood that were not controlled in this study might impact on the level of cannabis use in the UHR cohort.
Methodological difficulties in measuring the quantity of cannabis consumed by individuals have been referred to elsewhere [13, 20]. The increase in the concentration of tetra-hydro-cannabinol (THC) in more recent strains of the Cannabis sativa plant [45], and the differing THC content in individual cannabis preparations make it difficult to estimate accurately the quantity of THC used by the high-risk sample. We have chosen to assess quantity of cannabis use by measuring frequency of use and diagnosis of dependence. It is acknowledged that this approach may not accurately discriminate between mild and moderate users, and one study found that long-term users typically used more potent preparations [46]. Using a ‘standardized’ measure of cannabis (such as that described by Brewer et al. [47]) might have provided more useful information.
The length of time of cannabis use also was not assessed. This UHR cohort may have only used cannabis for a relatively short period of time and its impact on mental health may not yet have been fully realized.
Among the strengths of the study were the rigorous use of assessment procedures, and the assessment of multiple classes of substance use. Only a very small percentage of the high-risk sample met dependence criteria for other substances, and the use of more than one substance was uncommon. It was not possible to partial out the effects of other substances by statistical means, due to the small number of individuals using more than one substance. The potential influence of other factors on the relationship between cannabis use and psychosis was not controlled in this study but should not be ignored.
An obvious weakness of this study was the lack of monitoring of cannabis and other drug use after recruitment. Escalating cannabis use among existing users or de novo use post entry are still definite possibilities that may impact on later psychotic status. Therefore, we would not rule out cannabis use as a malleable risk factor for onset without assessing this possibility. Future research in this area should seek to assess the level of cannabis use by young people at high-risk of psychosis regularly (i.e. monthly) not only at intake. In this way, potential fluctuations in use immediately prior to the onset of acute levels of symptoms can be better assessed. A study is currently underway at PACE that seeks to address this issue.
Footnotes
Acknowledgements
Thanks to the Victorian Health Promotion Foundation for providing a research programme grant, and the support of the Victorian Department of Human Services through the ‘Turning the Tide’ strategy. We thank the following colleagues for assistance in recruitment and follow-up: Alison Blair, Colleen McFarlane, Elizabeth Cosgrave, Jenny Bravin, Dominic Germano, Mats Hallgren, Anthony McDonald and Shona Francey.
Aspects of this paper were presented at the International Congress on Schizophrenia Research, Whistler Resort, British Columbia, Canada, April/May 2001 and the 3rd National Early Psychosis Conference, Melbourne, Australia, October 2001.