
Abstract
Objectives: The identification of individuals at high risk of becoming psychotic within the near future creates opportunities for early intervention before the onset of psychosis. This study sets out to identify a group of symptomatic young people in a Chinese population with the high likelihood of transition to psychosis within a follow-up period of 6 months, and to determine the rate of transition to psychosis in this group.
Method: Symptomatic individuals with a family history of psychotic disorder, subthreshold psychotic symptoms or brief transient psychotic symptoms were identified using the operationalized criteria of an ‘At Risk Mental State’. The individuals were prospectively assessed monthly on a measure of psychopathology for 6 months.
Results: Eighteen out of 62 individuals (29%) made the transition to frank psychosis within a 6 month follow-up period, with the majority occurring within 3 months. In addition, significant differences were found in the intake Positive and Negative Syndrome Scale, Comprehensive Assessment of ‘At Risk Mental State’ and Global Assessment of Functioning scores between the group that ultimately became psychotic and the group that did not.
Conclusion: The period of the highest risk of transition to psychosis was within the 3 months after the study began. Thus, distressed youths in our outpatient clinic, who meet the high-risk criteria should be monitored most closely in the initial 3 months, particularly those individuals with high levels of psychopathology and functional decline.
Introduction
Psychosis in general, and schizophrenia in particular, is serious and often affects young people. Up to now, the aetiology of schizophrenia remains unknown. Despite progress in the development of medication with fewer side-effects, the treatment often cannot alleviate the disability associated with this chronic form of illness. Deficit symptoms and cognitive impairment, which appear to be the greatest determinants of disability, remain largely beyond the reach of current forms of treatment [1]. The treatment outcome is often poor and associated with extensive cost, burden, morbidity and mortality [2–5]. The rationale for early intervention in psychosis has been extensively discussed in a considerable number of papers in recent years [6–11].
Various studies have demonstrated that the prepsychotic or prodromal period is characterized by nonspecific symptoms such as depressed mood and anxiety, as well as sub-threshold psychotic symptoms [12–14]. Subtle subjectively experienced cognitive, vegetative and perceptual disturbances called ‘basic symptoms’ have also been described [15–17]. This prodromal period is often prolonged, lasting from 2 to 5 years [18–21], and is associated with substantial levels of psychosocial impairment and disability [10,22–24]. Researchers and clinicians view the prodromal period as potentially important for early intervention and the possible prevention of the development of psychotic disorders.
Klosterkotter et al. assessed a cohort of patients with personality and neurotic disorders for presence of ‘basic symptoms’, using the Bonn Scale for the Assessment of Basic Symptoms [25]. After an average follow-up period of 9.6 years, 79 out of 160 subjects had developed schizophrenia. The presence of certain ‘basic symptoms’, such as thought interference, thought blockages, pressure of thought, visual distortions or the disturbed reception of languages, was found to be highly predictive of psychosis [26, 27].
McGorry et al. introduced the term ‘At Risk Mental State’ (ARMS), implying that a sub-threshold syndrome can be regarded as a risk factor for the subsequent development of psychosis, but that the onset of psychosis is not inevitable [22, 23]. Criteria for the identification of the ultra high-risk cohort have previously been outlined and their rationale described [28, 29]. Comprehensive Assessment of ‘At Risk Mental State’ (CAARMS) [27], was specifically designed to prospectively measure subthreshold psychotic symptoms in the group at high risk of developing psychosis. It incorporates seven dimensions of psychopathology, including positive symptoms, cognitive symptoms, emotional disturbances, negative symptoms, behavioural change, motor or physical change and general psychopathology. It also incorporates some items from the Huber Basic Symptoms. It operationally defines ARMS criteria as well as the threshold for established psychosis, and has demonstrated good reliability and predictive validity (Yung et al., in preparation, personal communication, 1994).
Several studies were conducted at the Personal Assistance and Crisis Evaluation clinic over recent years, and yielded a conversion rate of 30–50% [9,29–33].
Several other preventive studies have been initiated in the last few years, using ARMS criteria that are similar to those used at the Personal Assistance and Crisis Evaluation clinic. The conversion rates to psychosis that have been reported from the early phases of these studies are between 33% and 58% [6].
The current study is a naturalistic prospective study, with an aim to identify high-risk individuals in the Chinese population who may then transit to psychosis within a brief follow-up period, and to determine the features that distinguish high-risk individuals who go on to develop psychoses and those who do not. The results will not only facilitate our understanding of the nature and development of psychosis, but may also shed light on the type and timing of intervention for young high-risk individuals in this initial critical phase of illness progression in our local population.
Method
Aims
To assess rate of transition to psychosis in a group of high-risk Chinese youths within 6 months of study entry. To compare the group of youths that became psychotic with the group that did not over 6 months of follow-up on variables such as measurement of psychopathology and functional decline.
Subjects
This was a naturalistic prospective study. The subjects were outpatient referrals from the Early Assessment Service for Young people with psychosis (EASY), which was established in Hong Kong in July 2001 [34]. It currently serves a population of seven million, and has four centres [34]. The referrals were derived from educational settings, youth services, adolescent medical centres, primary care, general health services, mental health professionals and hotlines. The recruited subjects were assessed and followed up monthly at the EASY Kwai Chung Hospital clinic.
Inclusion criteria
Age 9–25 years Subjects meet one or more of the three operationalized criteria that are defined in the CAARMS 2002 version [22, 30]
Vulnerability Group Combination of trait risk factors: that is, a family history of psychosis in a first degree relative and a significant deterioration in functioning as measured by a 30% drop in Global Assessment of Functioning (GAF) score. Attenuated Psychotic Symptom Group Symptoms that deviate from normal phenomena but are not yet frankly psychotic: that is, sub-threshold intensity. Brief Limited Intermittent Psychotic Symptom (BLIPS) Group Symptoms that are of psychotic intensity but very infrequent, or which have a total duration of less than 7 days before resolving spontaneously.
The three operationalized criteria are described in the CAARMS [30].
Exclusion criteria
Known history of psychotic episode for longer than a week Previous or current treatment with antipsychotic or mood stabilizer drugs Intellectual disability Organic brain disorder
Transition to psychosis
The main outcome measure in this study was the development of psychosis. The point of onset was defined as a specific score on severity and frequency in the subscales for disorders of thought content, perceptual abnormalities or disorganized speech in the CAARMS [30].
Intake and follow-up assessments
At the study intake, the subjects were assessed with the CAARMS, the Positive and Negative Syndrome Scale (PANSS) [35, 36], the GAF [37, 38] and the Structured Clinical Interview for DSM-IV (SCIDDSM-IV) [36]. At monthly intervals thereafter, the CAARMS with sessions on positive symptoms was used to determine the thresholds for psychosis. After the subjects met the CAARMS operationalized psychotic threshold, the SCID was conducted within 3 months to determine the current DSM-IV diagnosis. The PANSS and GAF were also completed. Subjects who did not become psychotic had a full SCID completed at the 6-month follow-up to detect any other psychiatric diagnosis. The PANSS and GAF were also conducted at that time.
Data analysis
SPSS for Windows (SPSS Inc., 2002, Version 10.1, Chicago, IL, US) was used to perform the analysis. For categorical variables, chi-squared tests were used to assess whether different categories of variables differed in terms of the proportion of subjects becoming psychotic within 6 months. For the numerical variables, the t-tests were used to compare the mean scores of those who became psychotic within 6 months and those who did not.
Results
Referrals
Between June 2002 and April 2003, there were 256 referrals to the EASY Kwai Chung Hospital clinic, among which 153 were psychotic and they were treated accordingly. With the remaining 103 subjects, 67 met the operationalized intake criteria, and 62 of them consented to participate in the project.
The 62 recruited subjects were not on antipsychotic or moodstabalizing medication at intake. They all received supportive counselling; they could receive symptomatic treatments with antidepressant and anxiolytic medication when needed.
Most subjects (n = 51) met the ‘attenuated’ intake criteria (Group 2). Twelve cases met the ‘BLIPS’ criteria (Group 3) and 12 cases met the vulnerability criteria (Group 1). There was a considerable degree of overlap between the groups (Fig. 1).
Numbers in ARMS groups (numbers who transited to psychosis in 6 months shown in brackets). ARMS, At Risk Mental State; BLIPS, Brief Limited Intermittent Psychotic Symptoms.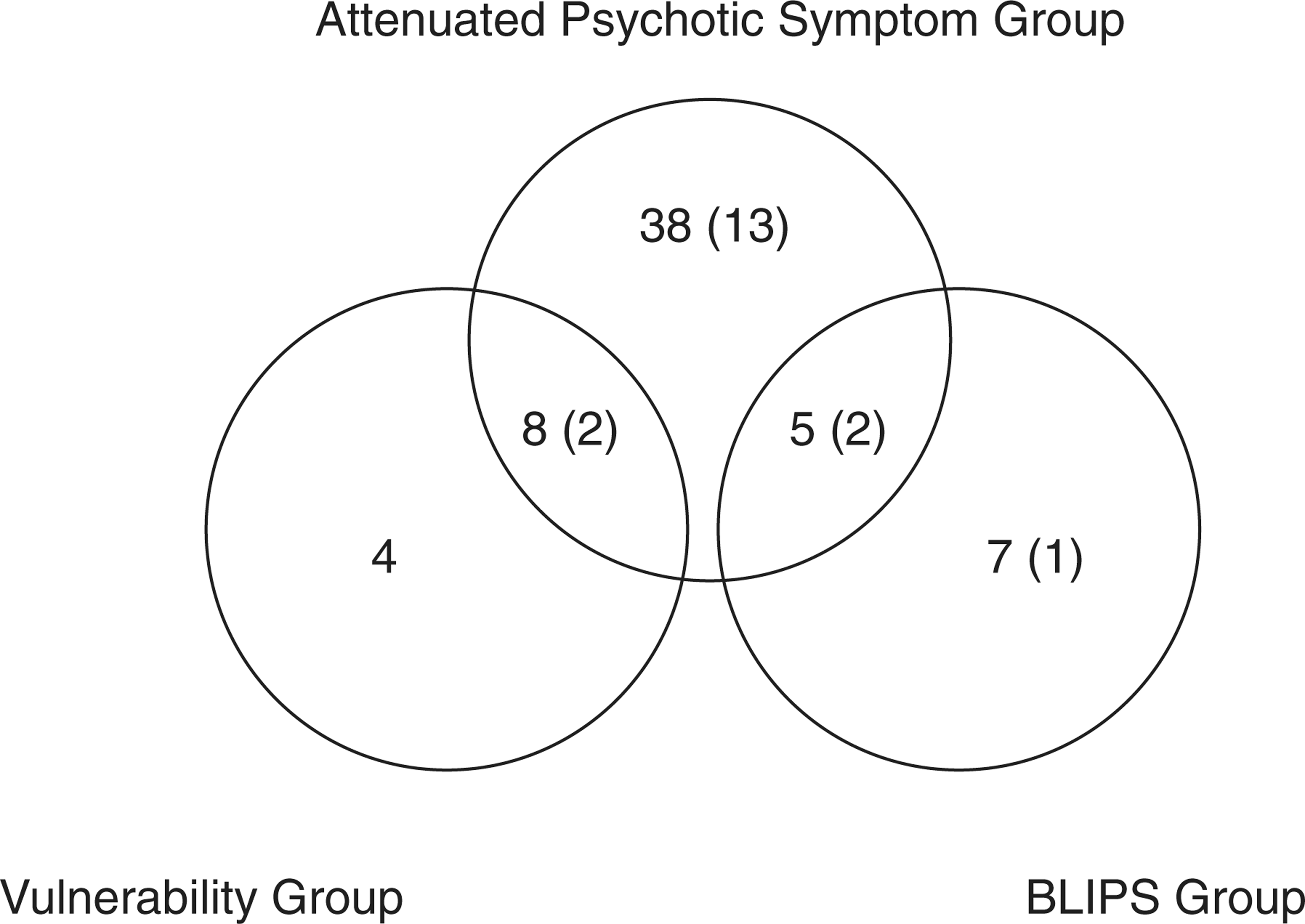
Intake characteristics
The mean age at first assessment was 16.2 years (median = 16.6, SD = 3.7, range = 6.9–23.5). Thirty-six of the subjects were male and 26 were female. Fifty-one of the subjects were born in Hong Kong, while 11 were born in mainland China with a mean length of stay in Hong Kong of 7.1 years (median = 6, SD = 3.1, range = 3–12). Most of the subjects were students.
Nine subjects reported histories of substances misuse. Among these substance misusers, ketamine was the most commonly reported substance used (6 out of 9), followed by ecstasy (n = 4), cannabis (n = 3), amphetamine-like substances (n = 2), solvents (n = 1) and opiates (n = 1).
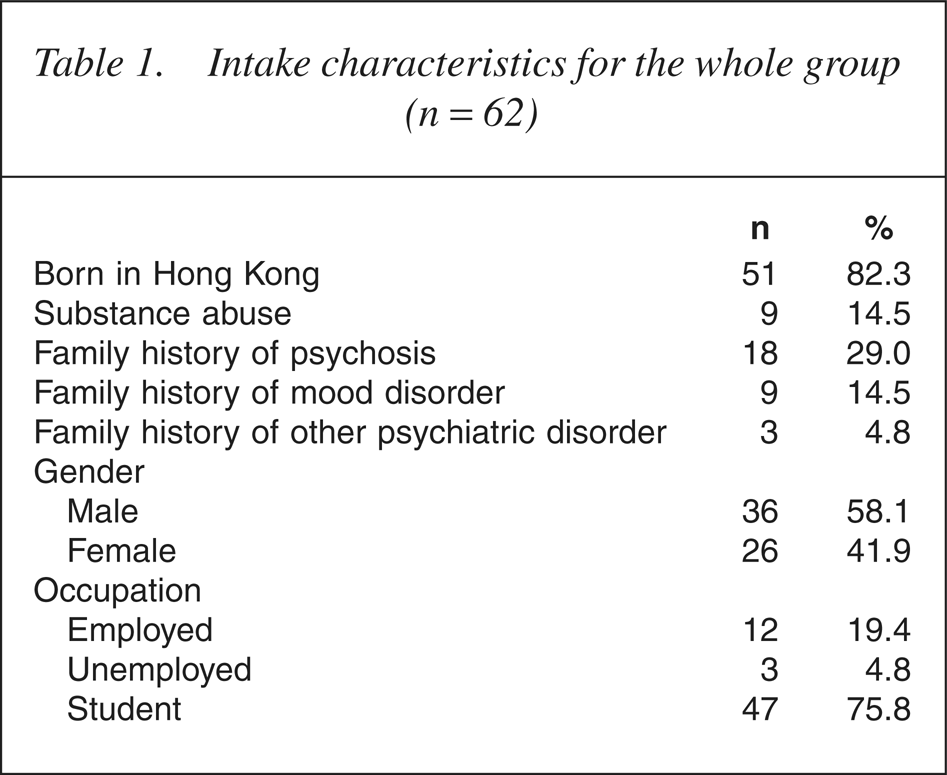
Eighteen subjects reported family histories of psychotic illness (in either first or second degree relatives). Nine reported family histories of mood disorders as shown in Table 1.
Intake characteristics for the whole group (n=62)
The mean GAF and PANSS scores at first assessment were 72.0 (median = 70.0, SD = 10.8) and 53.0 (median = 50.0, SD = 12.1), respectively. The time between symptom onset and time to study intake varied widely among the subjects, with a range of 11–2405 days (6.6 years), a median of 463 days.
From the CAARMS psychopathology subscales, the most commonly reported ‘first noticed disturbances’ were irritability (n = 18), followed by avolition (n = 13), subjective cognitive experience (n = 11) and disorganized stigmatizing behaviour (n = 11). Among the subjects who developed psychosis in 6 months, the most commonly reported ‘first noticed disturbance’ were irritability (n = 7) and subjective cognitive impairment (n = 5).
The most frequent concerns, as counted by ≥ 2 score in the CAARMS psychopathology subscales, were subjective cognitive experience (n = 58), disorder of thought content (n = 56) and depression (n = 52).
Nine subjects were followed up for less than 6 months. However, they were all contacted via telephone 6 months after their initial assessment. Both the subject and one other informant were spoken to over the telephone. They were asked about the severity, frequency and persistency of the disorder of thought content, perceptual abnormality or disorganized speech to ascertain whether the operationalized psychosis threshold criteria had been met. None of these nine subjects met the psychosis threshold criteria.
Transition to psychosis
Over the 6-month follow-up period, 18 subjects met the criteria for a psychotic disorder according to the above definition. Therefore, the 6-month transition rate was 29% (18 of 62). Of the 18 subjects who became psychotic within 6 months, 16 made the transition within 3 months of study entry.
Comparison between psychotic and non-psychotic subjects
A comparison was made between those who became psychotic within 6 months and those who did not. Age, gender, family history of psychiatric illness, history of substance misuse and place of birth were not significantly related to the onset of psychosis.
The intake scores from the PANSS, CAARMS and GAF of the two groups are shown in Table 2.
Comparison of intake scores between those who became psychotic in the 6-month followup and those who did not
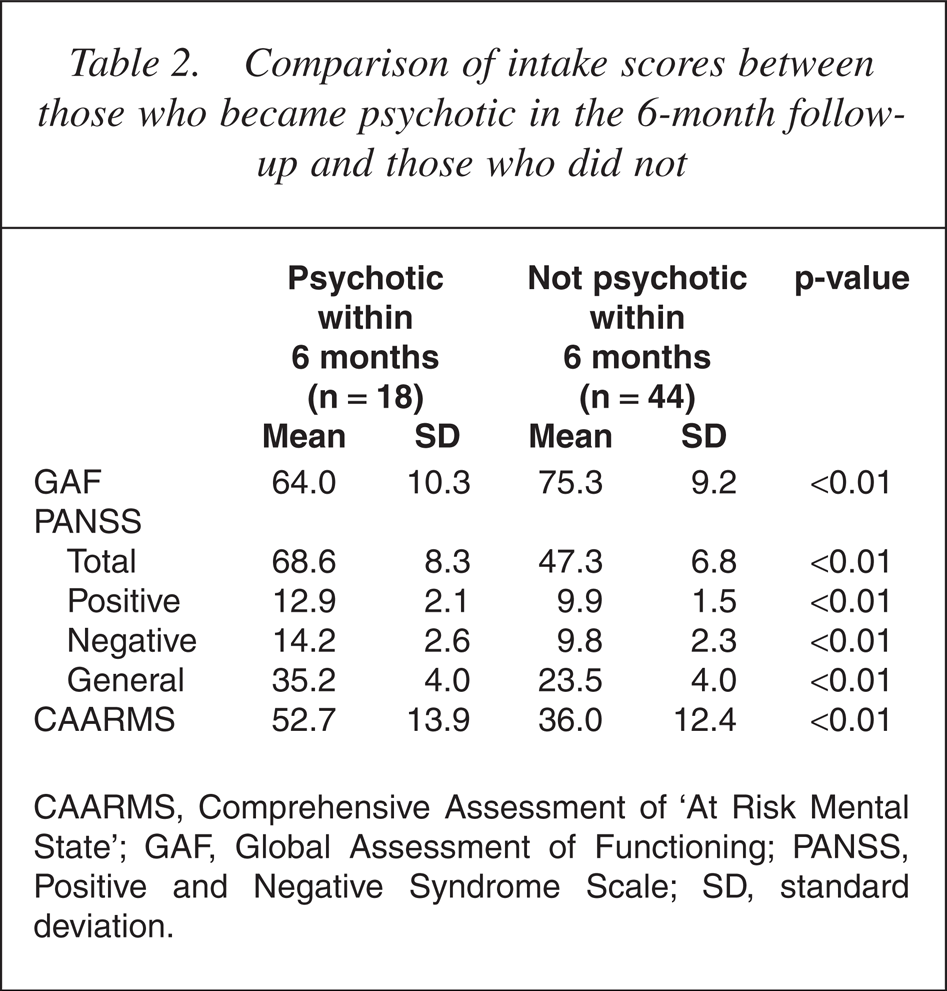
CAARMS, Comprehensive Assessment of ‘At Risk Mental State’; GAF, Global Assessment of Functioning; PANSS, Positive and Negative Syndrome Scale; SD, standard deviation.
Significant differences between the groups were found in the baseline scores of the PANSS (total, positive, negative and general subscales), CARRMS and GAF.
SCID-DSM-IV diagnosis
Table 3 shows the SCID data (current diagnosis only) on psychotic disorder at intake and after 6 months for the non-psychotic group, and within 3 months of psychosis onset for those who became psychotic.
DSM-IV psychotic disorder diagnosis at intake and all psychiatric diagnosis at 6-month follow-up
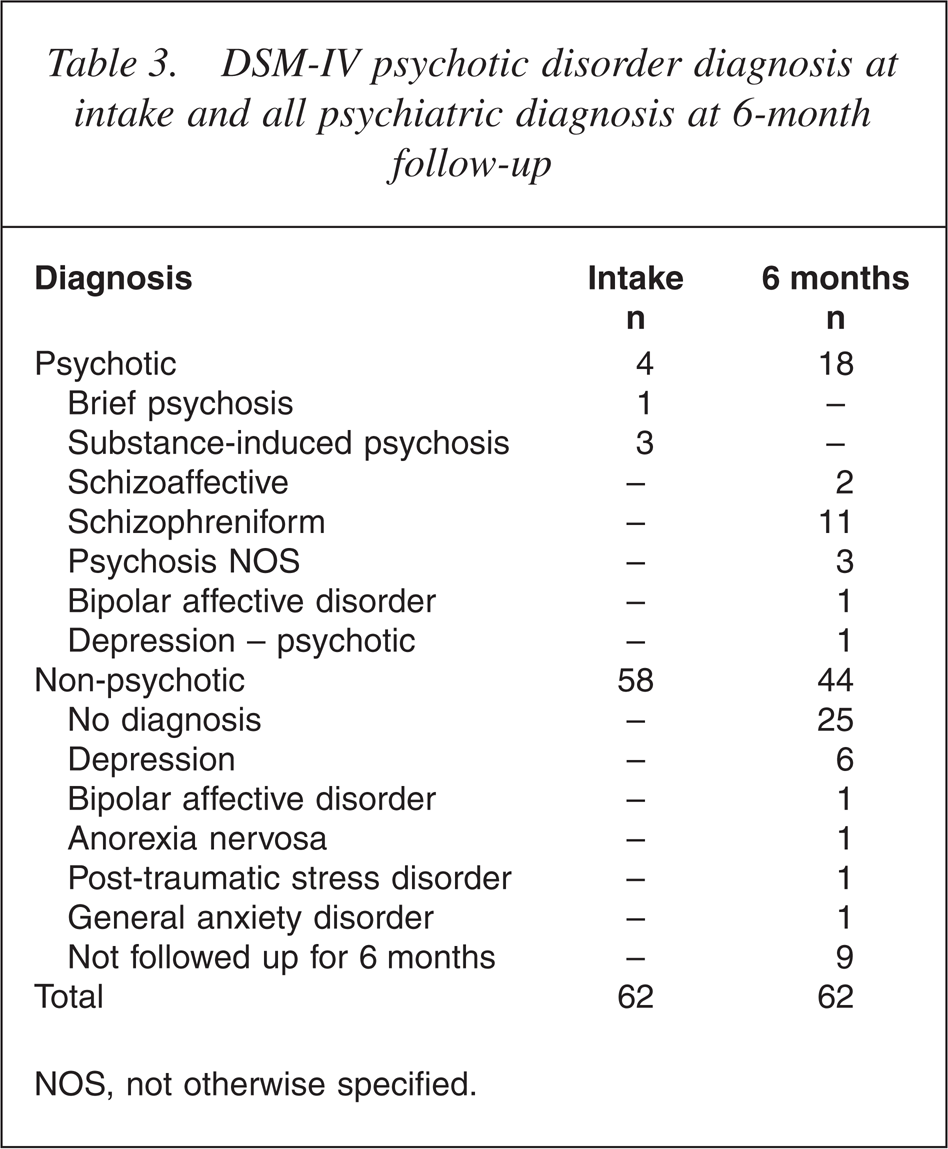
NOS, not otherwise specified.
No subjects were psychotic at intake. However, four subjects who fulfilled the BLIPS Group of the operationalized intake criteria met the SCID-DSM-IV criteria for a brief psychosis (1 subject) or substanceinduced psychosis (3 subjects). Such DSM-IV diagnoses can be made with a duration of psychotic symptoms as brief as 1 day.
At the end of the 6-month study period, 11 subjects had onset of schizophreniform psychosis (the DSM-IV diagnosis may change to schizophrenia with longer follow-up), two cases had affective psychosis (one bipolar disorder, one major depression with psychotic features), two had schizoaffective disorder (depressed type) and three subjects had psychotic disorder not otherwise specified.
Of the remaining 44 non-psychotic subjects, 22 had no current diagnosis and 13 had another non-psychotic diagnosis (mainly mood and anxiety diagnosis) at six months, as shown in Table 3. Final diagnosis was missing for nine subjects as they were not followed up for the entire study period and were only contacted via telephone at six months.
Discussion
The study results indicate that it is possible to identify a subsample of our local population with a high rate of transition to psychosis (29%) within a 6-month period.
The level of substances misuse in this group (9 out of 62) was generally relatively low compared with the reports of substance use by the Australian high-risk cohort [39, 40] or early psychosis cohorts elsewhere [41–43]. The majority (86%) of our group reported no history of substance misuse. In addition, substance misuse was found not to be associated with a heightened risk of developing psychosis. However, this study relied solely on self-reporting and the lack of monitoring in substance misuse after study intake may have underestimated the actual rate. Additionally, this study recruited a much younger age group, including children under 12 years, and in general, our local Chinese population tends to have lower rates of substance misuse [44]. Most importantly, the individuals who present to our service setting are a biased, help-seeking sample and they certainly do not represent all young people who eventually develop psychosis [40].
Subjective cognitive impairment was found to be the most commonly reported (58 out of 62 subjects) and one of the most frequently reported first noticeable symptoms in our high-risk group at intake. This finding is comparable to several other studies [13,45–47]. Not only was it found to be the most commonly reported complaint in the whole group, it was actually found to be present in all subjects who then developed psychosis within 6 months.
Our reported 6-month transition rate (29%, 18 out of 62) is lower than the 6-month transition rate that was reported in the Australian group (8 out of 20, 40% 6-month transition rate) [48]. This may be because our subjects were younger (mean age 16 vs 19) and had not reached the peak age of psychosis onset of 15–30 years [49, 50]. In fact, none of the eight recruited subjects under 12 years of age developed psychosis within the 6-month follow-up period.
The distinction between the premorbid and prodromal stages may be hard to define. Some of these younger subjects may have been at a premorbid stage, but may later have evolved into the prodromal phase with acute changes, and then transited to psychosis [3]. Attempts were made to date the onset of prodrome by asking about changes from the normal self. However, as adolescence is a period of major psychological and social change [13, 51, 52], this distinction between premorbid personality and prodromal symptoms may not be clear-cut.
The idea that youths at high risk who will become psychotic can be clearly distinguished from those who do not become psychotic is an oversimplification of the situation. Thirteen of our total subjects had a nonpsychotic SCID-DSM-IV diagnosis at six months. Most of them had mood disturbances or disabling anxiety. The non-psychotic diagnoses in our subjects at six months may suggest that these high-risk subjects are heterogeneous, and that the ‘high-risk’ criteria may not be specific to psychosis but may also apply to other psychiatric diagnoses. Thus, these mental changes may indicate different underlying pathologies such as anxiety, depression or situational crises.
Alternatively, other non-psychotic diagnoses may reflect a prodromal phase of schizophrenia, as various studies show that there is an increased chance of schizophrenia in those subjects with other non-psychotic diagnosis [45, 53]. These non-psychotic disorders may themselves be manifestations of a psychotic prodrome. The results of a further prospective study of the conversion rates of this group with non-psychotic diagnoses may shed light on whether these syndromes represent risk factors or are simply sub-syndromal symptoms of an incipient psychosis. Ongoing research will clarify whether the conversion rates reported thus far change as a function of longer follow-up intervals.
Limitations
It must be acknowledged that our sample size was small and that the power of analysis was limited. In addition, the subjects were only followed up for 6 months, which may be too little time to allow comment on the true significance of differences as predictors of the future onset of psychosis. This may be clearer when the whole cohort has lived through the at-risk years. This study cannot be generalized beyond those who were selected by the intake criteria: that is, those who were symptomatic, help-seeking and consented to participate in the study.
Conclusions
This is the first prospective study to examine the psychopathology of a Chinese sample at high risk of developing a psychotic illness. The major findings of this study were:
Twenty-nine per cent of the identified high-risk subjects developed psychosis within 6 months. The identified high-risk subjects had moderate levels of functional decline and psychopathology at the study intake. A lengthy delay was found between the onset of symptoms and the study intake (ranging from 11 days to 6.6 years). Subjective cognitive impairment was found to be the most commonly reported symptoms in our high-risk group (58 out of 62), and it was reported in all those who developed psychosis within 6 months (18 out of 18). In addition to the 18 subjects who received psychotic diagnoses within 6 months, 13 subjects had non-psychotic diagnoses at six months which mainly consisted of anxiety or depressive disorders.
Footnotes
Acknowledgements
Thanks to P.D. McGorry and A. R. Yung for providing the CAARMS instrument.