
Abstract
Study Design
Systematic review and meta-analysis.
Objective
To compare the recurrence and perioperative complication rate of en bloc vertebrectomy (EV) and intralesional resection (IR) in the giant cell tumor of the mobile spine (SGCT).
Methods
We systematically searched publications in the PubMed and Embase databases for reports of SGCTs, excluding the sacrum. Two reviewers independently assessed all publications. A meta-analysis was performed using local recurrence and postoperative complications as the primary outcomes of interest.
Results
There were four articles reporting recurrence and two articles reporting postoperative complications. All included articles were case series. In all, 91 patients were included; 49 were treated with IR and 42 were treated with EV. Local recurrence rates were 36.7 and 9.5% in the IR and EV groups, respectively. Rates of postoperative complications were 36.4% with IR and 11.1% with EV. Overall, patients treated with EV not only had a lower recurrence rate (relative risk [RR] 0.22; 95% confidence interval [CI] 0.09 to 0.52) but also had a lower postoperative complication rate (RR 0.34; 95% CI 0.07 to 1.52) compared with IR.
Conclusions
Based on the limited data obtained from systematic review, SGCT patients treated with EV had a lower recurrence rate and fewer postoperative complications than those treated with IR.
Keywords
Introduction
Spinal giant cell tumors (SGCTs) are locally aggressive benign bone tumors that can occur anywhere along the spine. SGCTs account for approximately 2 to 3% of all giant cell tumors (GCTs). Its incidence is higher in females, the sacral region, and patients aged 20 to 40 years. 1 , 2 SGCTs are usually discovered at Enneking stage 2 (fully osteolytic lesion with well-defined borders) and stage 3 (ill-defined border lesion eroding and extending beyond cortex into the surrounding soft tissue). 3 Donthineni et al reported that 13.7% of SGCTs eventually metastasize to the lung, a higher rate compared with extremity GCT. 4
The goals of SGCT treatment are tumor removal, spinal stability, and neural tissue decompression. The choices of operative treatment are en bloc vertebrectomy (EV) or intralesional resection (IR). 5 , 6 Because of the proximity of vital structures to the vertebrae, EV may be too damaging to undertake in some cases. Therefore, IR might be the alternative choice in selected cases. 7 Numerous adjuvant therapies can be employed with either of these two surgical strategies.
Because previous studies have provided inconclusive results, we compared the overall recurrence rates and complications between IR with or without adjuvant therapy against EV in patients with SGCT from published case series.
Materials and Methods
Data Source and Search Strategy
Two independent reviewers (P.L., W.S.) performed a search in October 2015 of all peer-reviewed relevant literature in human patients using EMBASE and PubMed for studies comparing IR versus EV treatment in patients with SGCT. No language or date limitations were applied. The following search terms were used: ((giant cell tumo*) AND ((((((spine) OR spinal) OR vertebral) OR vertebra) NOT sacrum) NOT craniocervical)) AND ((recurrence) OR complicatio*). Additional searches were performed by using the reference lists from the retrieved studies that were relevant to SGCT.
Inclusion and Exclusion Criteria
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses protocol was followed for data selection and analysis. The inclusion criteria were randomized controlled trials, observational studies, or case series in patients with primary SGCT (excluding the sacrum), intervention (IR), comparator (EV), and outcomes that reported local recurrence or incidence of postoperative complications. Studies were excluded if they had fewer than three patients, multiple GCT lesions, less than 6 months’ follow-up, recurrent tumors, previous surgical resections, mixed reports with other tumor types, or lack of specificity for time points of recurrence or complications. Case reports, review articles, and technical reports were also excluded. Both reviewers independently screened abstracts and titles after removing duplicated publications. Then, thorough full-paper readings were performed of the studies that might meet the inclusion criteria to determine final inclusion. Disagreements were solved by discussion for consensus.
The rates of local recurrence and postoperative complications were extracted directly from the original studies to calculate risk ratios. Both reviewers extracted data independently. The methodological quality of the included studies was independently assessed by the two reviewers using the Methodological Index for Nonrandomized Studies (MINORS) scale that allocates a maximum of 24 points for comparability, exposure, quality of selection, and outcome of study participants. 8
We performed a meta-analysis using Review Manager software (RevMan Version 5.1; Nordic Cochrane Center, Copenhagen, Denmark). Risk ratios (RRs) and 95% confidence intervals (CIs) were used to evaluate the dichotomous outcomes of incidence of local recurrence and complications. Statistical heterogeneity was assessed using the Cochrane Q test, with a p value set at 0.1 for significance. Heterogeneity between trials was evaluated based on an assigned I2 value and substantial heterogeneity was represented by an I2 value greater than 50%. The fixed-effects model was used when the effects were assumed to be homogenous. In the presence of heterogeneity, we used a random-effect model. A funnel plot with the test of Begg and Mazumdar was used to evaluate publication bias. 9 , 10 , 11 Sensitivity analysis was performed by rejecting the studies with higher statistical heterogeneity. A p value < 0.05 was considered statistically significant.
Results
There were 507 abstracts (172 from PubMed and 335 from EMBASE) identified through the database search. Of these, 122 publications were duplicates and thus a total of 385 unique abstracts were screened. Eighty-six abstracts were selected for full review after 299 nonrelevant abstracts were removed. Eighty-two reports were excluded for following reasons: 3 had unclear data, 17 had multiple tumor types reported, 7 had no surgery, 10 did not compare IR/EV, 4 had recurrent tumors, 2 had multiple lesions, and 39 were nonqualifying publications (review article, case report, technical note, correspondence). The reviewers selected a total of four studies for systematic review and meta-analysis of SGCT recurrence (Fig. 1). The details of the included studies are summarized in Table 1.
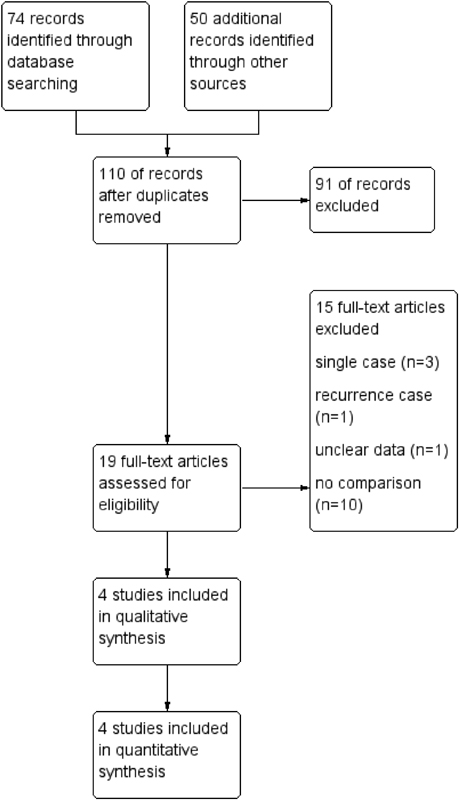
Flow diagram demonstrating study search results.
Characteristics of included studies
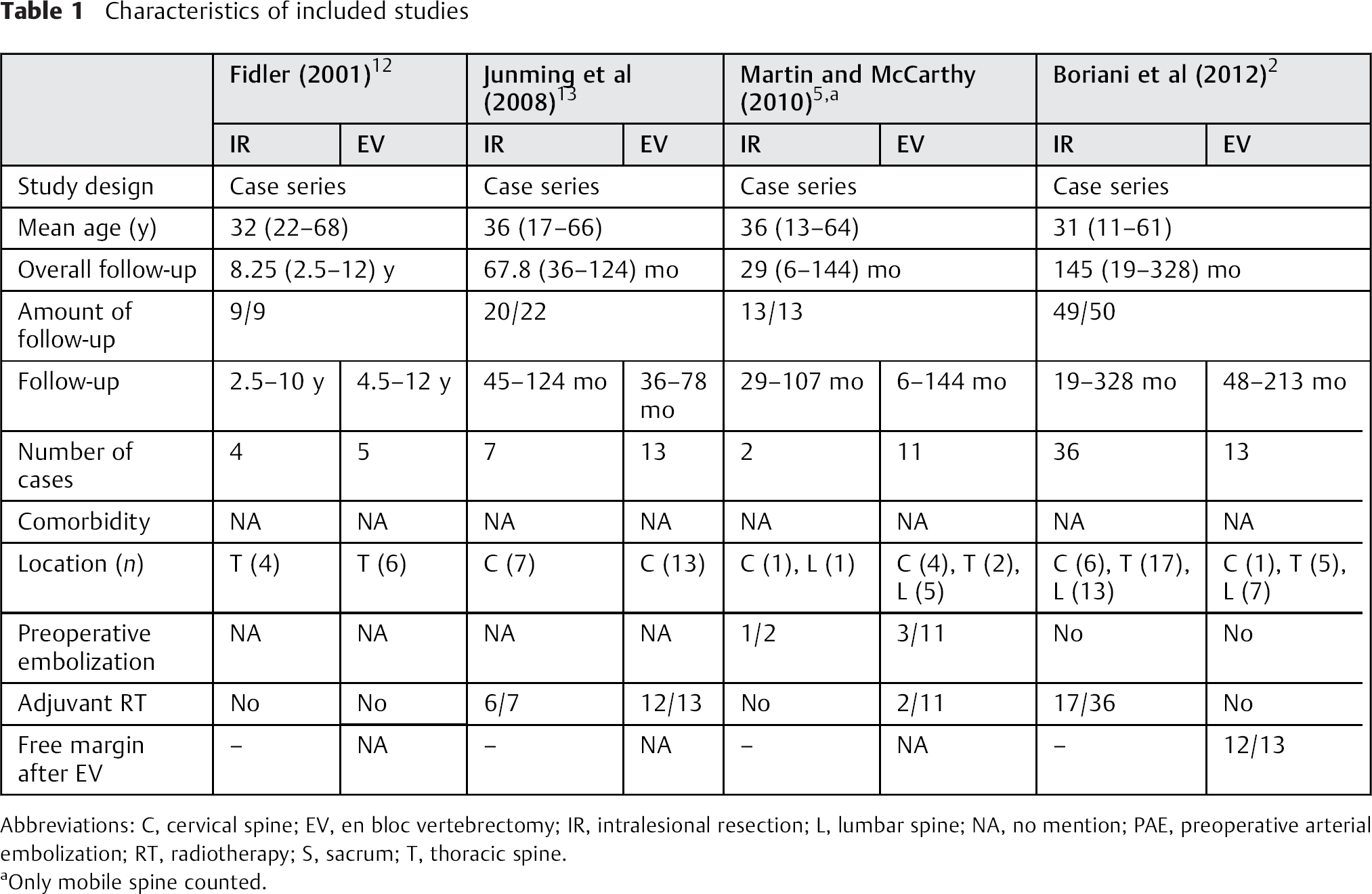
Abbreviations: C, cervical spine; EV, en bloc vertebrectomy; IR, intralesional resection; L, lumbar spine; NA, no mention; PAE, preoperative arterial embolization; RT, radiotherapy; S, sacrum; T, thoracic spine.
Only mobile spine counted.
All four studies selected for meta-analysis of recurrence were retrospective case series that showed lower rates of recurrence and postoperative complications with EV as compared with IR. 2 , 5 , 12 , 13 However, EV was not performed prior to 1991 in the series by Boriani et al. 2 The follow-up period ranged from 19 to 328 months. Most of the patients having IR received postoperative radiation therapy ranging from 30 to 50 Gy in 10 to 20 fractions. 2 Both the series by Boriani et al and the series by Junming et al had one patient death in the early postoperative period; these patients were not included in their analyses because local recurrence could not be assessed. 2 , 13 We excluded one case in the series of Junming et al of an SGCT lesion located solely in the posterior elements of C7.
In total, the included series contained 91 patients with primary SGCT. Of these patients, 42 underwent EV and 49 underwent IR. Overall recurrence rates for SGCT treated with IR versus EV were 36.7% (18 of 49 patients) versus 9.5% (4 of 442 patients), respectively. The pooled RR for tumor recurrence was 0.22 (95% CI 0.09 to 0.52; p = 0.0006; homogeneity I2 0%), suggesting that IR was associated with a higher rate of recurrence (Fig. 2).

Forest plot to illustrate risk ratio in recurrence between vertebrectomy and intralesional resection. Abbreviations: CI, confidence interval; M-H, Mantels-Haenszel methods.
Two of these studies also qualified for meta-analysis of postoperative complications, for a total of 29 patients. 12 , 13 In the IR group, 4 of 11 patients experienced complications (including screw loosening, graft fracture, intrathoracic hematoma, and respiratory failure) versus 2 of 18 patients in the EV group (including intraoperative bleeding/abdominal wall weakness and postoperative cerebrospinal fluid leakage). Junming et al reported an intraoperative unilateral vertebral artery injury in two patients in the EV group that required unilateral ligation; however, these patients experienced no postoperative deficits and were not counted as postoperative complications in the analysis. 13
The rates of postoperative complications for SGCT treated with IR versus EV were 36.4% (4 of 11) versus 11.1% (2 of 18), respectively. The pooled RR for postoperative complications was 0.34 (95% CI, 0.07 to 1.52; p = 0.16; homogeneity I2 = 0%; Fig. 3). Therefore, there was a lower rate of postoperative complications associated with EV compared with IR, but without statistical significance.

Forest plot to illustrate risk ratio in postoperative complications between en bloc vertebrectomy and intralesional resection. Abbreviations: CI, confidence interval; M-H, Mantels-Haenszel methods.
The mean MINORS scores of the included studies were 14.75 ± 1.50 (Table 2). Funnel plotting for bias demonstrated that all four studies fell within the funnel, all near the midline (Fig. 4).
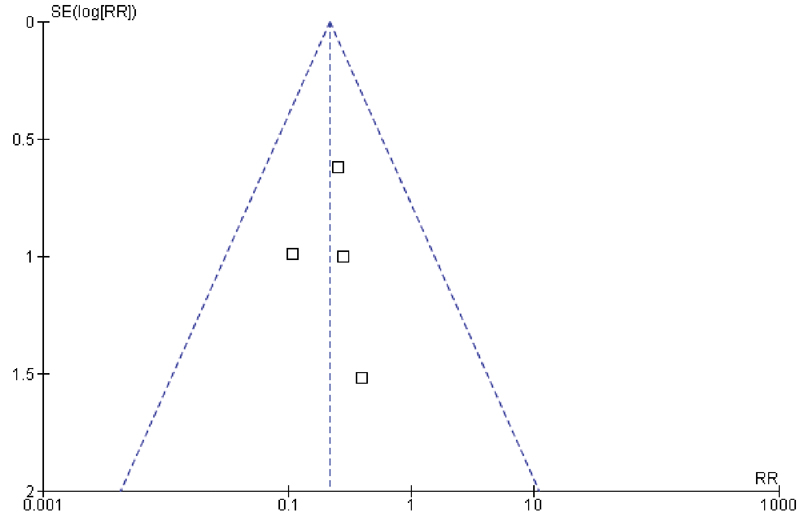
Funnel plot for the publication bias test of the four eligible studies.
Risk of bias and technical quality assessment of included studies using Methodological Index for Nonrandomized Studies score
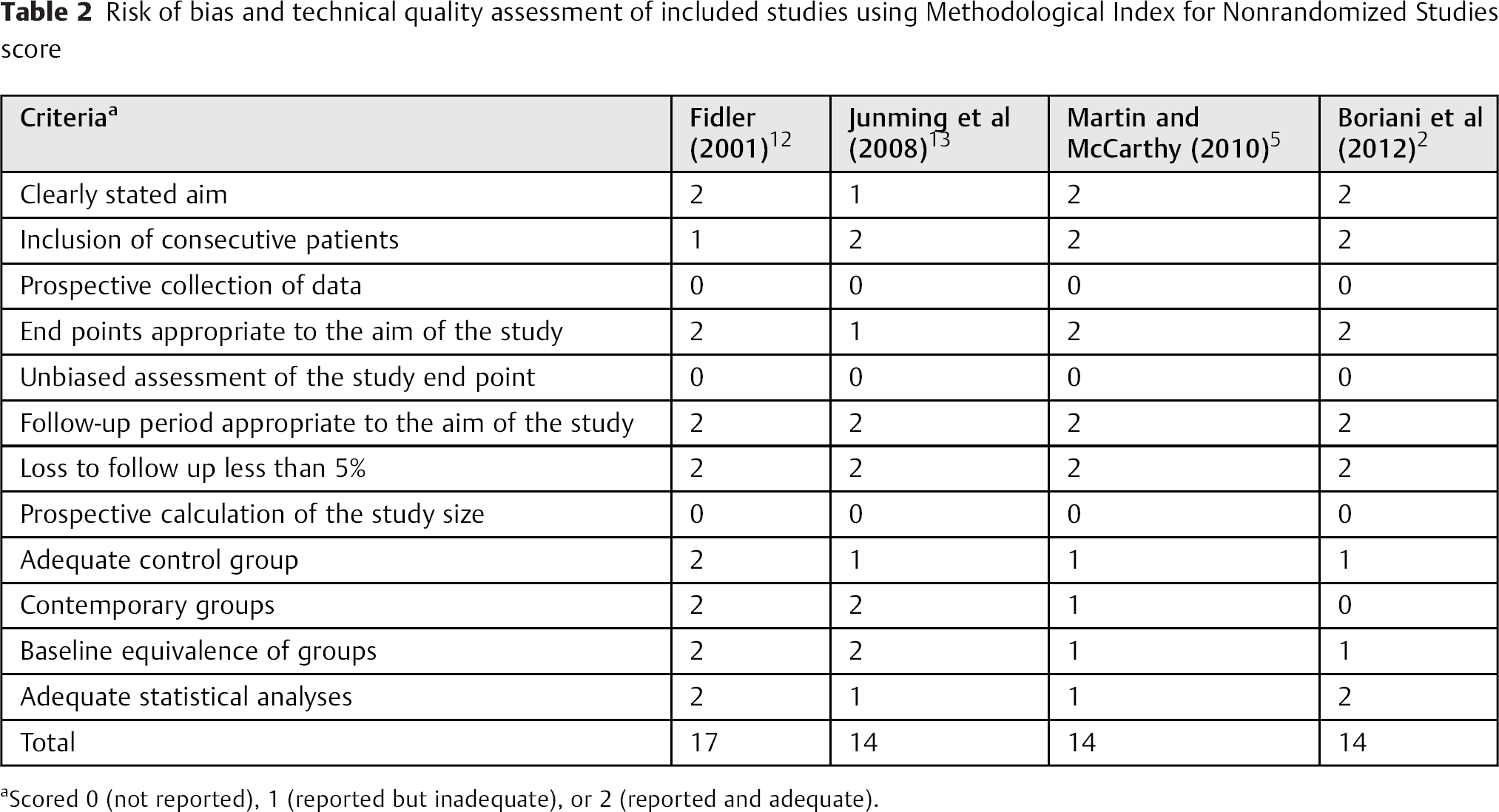
Scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate).
Discussion
GCTs of the mobile spine are classified as locally aggressive benign tumors, but they have a high overall reported rate of recurrence (11 to 45%). 14 , 15 , 16 Case series have been reported, suggesting that total tumor removal must be performed to prevent local recurrence and pulmonary metastases. Many single case reports showed no local recurrence after vertebrectomy in the cervical, thoracic, and lumbar regions. 17 , 18 , 19 , 20 , 21 However, because of the complexity of spinal anatomy and the proximity to neural elements, vertebrectomy may require sacrifice of vital structures causing significant and permanent postoperative morbidity. Other series have reported the efficacy of IR with adjuvant therapy for preventing local recurrence, a technique that arguably would produce lower complication rates and less morbidity. 22 , 23 , 24 Most of these studies had limited numbers of patients. Therefore, our objective was to systematically review studies comparing the efficacy of SGCT operative treatment and to increase statistical power by performing a meta-analysis.
EV has reported local recurrence rates of 0 to 14%, and IR has recurrence rates of 0 to 71%. 2 , 5 , 12 , 13 , 17 , 18 , 19 , 20 , 21 , 25 , 26 , 27 Our meta-analysis produced pooled local recurrence rates of 9.5% for EV and 36.7% for IR, a statistically significant fourfold higher recurrence rate. This difference existed even with the use of adjuvant treatments in patients having IR.
Postoperative complication rates have been reported for up to 24% of patients after EV, 2 , 5 , 12 , 13 and up to 80% after IR. 2 , 5 , 12 , 13 , 16 , 22 , 25 , 26 This study demonstrated that patients having IR had a higher rate of postoperative complications (36.4%) compared with patients having EV (11.1%), but this difference did not reach significance. There were many factors that affected postoperative complications including comorbidities, severity of disease, follow-up period, adjuvant therapy, and tumor location. Explanations as to why EV had a lower complication risk than IR may include selective bias (surgeons preferred EV in patients with fewer comorbidities, less-extensive tumor extension, and younger age), exclusion of studies (several studies were excluded because they only reported IR results), or underreporting of complications in the EV group.
None of the included studies reported details of comorbidities. There were no differences in overall follow-up duration or tumor location, but the use of adjuvant radiation varied in the two studies reporting its use in IR. 2 , 13 There was no difference in the local recurrence rate between patients having IR receiving radiation (35%) and those not undergoing radiation (21%). Because the use of adjuvant radiation was in part determined by the surgeons’ decision, the data may be biased.
The methodological quality of the included studies demonstrated MINORS scores between 14 and 17, slightly higher than the mean reported scores for nonrandomized surgical studies. Our assessment of bias demonstrated that all the included studies fell within the funnel plot, although the relatively small number of studies did not result in a wide distribution within the funnel.
Several limitations should be considered when interpreting these findings. First, no randomized controlled trials of SGCT have been conducted because of the relative rarity of SGCT, ethical issues, tumor proximity to surrounding neural structures, and high technical skill and experience required to perform EV. Second, only a few cases series met the inclusion criteria for the meta-analysis, and all were retrospective; only two studies reported the postoperative complication rates. Third, there likely was a physician selection bias in choosing the type of operation because less aggressive lesions in healthier patients were perhaps more likely to be treated with EV. Conversely, physicians may have preferred IR in patients who had severe comorbidities or extensive lesions. EV in the cervical spine can be a significant challenge because of surrounding vital anatomy and neurologic risk. IR may be selected in these cervical tumors in an attempt to prevent devastating complications and severe disability. Fourth, different adjuvant therapy protocols were used in the patients having IR, including radiotherapy and preoperative embolization. Additionally, in the series by Martin and McCarthy, two patients having EV had follow-up periods less than 1 year (6 and 10 months, respectively). Both of them had no recurrence at the final evaluation. Because of the short follow-up time, the incidence of local recurrence may be underestimated in this report. Thus, the meta-analysis does not provide any data regarding which adjuvant treatments are more efficacious when used with IR. Finally, included studies had variable follow-up durations and protocols.
Xu et al reported on factors influencing the recurrence risk in 102 patients with SGCT. Their multivariate analysis found that IR had a hazard ratio of 3.02 when compared with EV (p = 0.02). However, their report does not specifically state the recurrence-free intervals for the patients in each surgical treatment group, and thus we could not include their patients in our meta-analysis. However, their report provides informative findings on a relatively large series of patients, and their results mirror ours. 28
In conclusion, this meta-analysis demonstrated that EV for GCTs of the mobile spine was associated with a significantly reduced risk for future recurrence. In addition, EV had a lower postoperative complication risk, although this finding did not reach significance. Further multicenter prospective cohort studies are needed to strengthen the evidence for how best to treat these challenging tumors. Surgeons must carefully evaluate patients with SGCT on a case-by-case basis, weighing the morbidity of the surgery and the overall health of the patient with a decision to perform EV.
Disclosures
Panya Luksanapruksa: none
Jacob M. Buchowski: Consultant (Advance Medical, DePuy, CoreLink, Globus Medical, K2M, Medtronic, Stryker); Speakers’ bureau (Broadwater/Vertical Health, DePuy Synthes, Globus Medical, OrthoFix, Stryker); Royalties (Globus Medical, Wolters Kluwer Health); Travel expenses (AO Foundation)
Weerasak Singhatanadgige: none
David B. Bumpass: Consultant (Gerson Lehrman Group, Doximity); Grant (NASS)