
Abstract
Study Design
Retrospective cohort study.
Objectives
Atypical hangman’s fractures are associated with increased risk for neurologic injury due to involvement of the posterior cortex of the axis body. We present the largest single-center cohort of atypical hangman’s fractures with the goal of guiding treatment decisions and outcomes based on fracture classification.
Methods
We performed a retrospective analysis of all patients with atypical hangman’s fractures treated at a single Level I trauma center between January 2010 and September 2023. 51 patients met inclusion criteria and demographic, treatment, and radiographic data were recorded and compared across the Type I and II fracture groups.
Results
Final treatment modalities varied significantly between the groups (P < 0.01), with hard cervical collar and invasive halo immobilization being the most prevalent treatments for fracture Types I and II respectively. One Type I fracture patient and four Type II fracture patients failed non-operative treatment, requiring surgery. Across both groups, posterior cervical fusion (73%) was the most common surgical approach. Median length of stay varied significantly between the two fracture groups (2.0 (1.0-7.0) vs 5.0 (3.0-8.0) days; P = 0.01). Irrespective of fracture type, longer hospital length of stay was associated with increased patient age (IRR = 1.02; P < 0.01), non-white race (IRR = 2.47; P = 0.01), injury caused by MVC (IRR = 1.93; P < 0.01), and the presence of non-spine orthopedic injuries (IRR = 1.72; P = 0.03).
Conclusions
While atypical Type I hangman’s fractures may be managed effectively non-operatively with a hard cervical collar, atypical Type II fractures managed with a hard cervical collar are at greater risk of requiring subsequent surgical intervention.
Introduction
Fractures of the axis account for 15%–20% of all cervical spine fractures. 1 Among axis fractures, hangman’s fractures, or traumatic spondylolisthesis of C2, are the second most common fracture type, following odontoid process fractures.2,3 This fracture subtype has been estimated to account for up to 22% of all axis fractures and are often a component of more complex atlantoaxial injuries. 4 The classic description of hangman’s fractures, termed “typical,” involve bilateral C2 pars interarticularis fractures, which generally result in central canal enlargement with C2 anterolisthesis. “Atypical” hangman’s fractures, however, involve a coronal fracture that extends into either the unilateral or bilateral aspect of the posterior wall of the C2 vertebral body.1,5 Benzel et al described 12 such cases of coronally oriented vertical C2 body fractures in 1994, referring to them as Type I C2 body fractures as opposed to atypical hangman’s fractures. 6 Due to the involvement of the posterior vertebral body wall, there is an increased risk of spinal cord compression with anterior translation. Prior literature has shown that atypical hangman’s fractures may account for 18%–74% of all hangman’s fractures.4,5,7-9 Despite the increased risk of neurologic injury and compromise with atypical hangman’s fractures, there is no standard treatment paradigm for these fractures.
Historically, nonoperative management, with an orthosis or halo vest, has been the predominant treatment modality for most hangman’s fractures.10-13 Both typical and atypical hangman’s fractures may be classified using the Levine and Edwards classification system. Type I and some Type II fractures are thought to be well-suited for nonoperative treatment via immobilization due to their stable nature. However, in the case of more unstable fractures, such as Type IIa and Type III fractures, poor outcomes with non-operative treatment and advancements in surgical instrumentation and techniques have led to a shift toward operative intervention.2,11,14
A comprehensive meta-analysis by Li et al found that most patients with Type I and Type II fractures were treated nonoperatively via immobilization, whereas the majority of patients with Type IIA fractures and Type III fractures were treated operatively. 11 Furthermore, the authors reported that healing rates for Type I and Type II fractures managed nonoperatively were 100% and 60% respectively and healing rates for Type IIa and Type III fractures were below 50%. 11 However, there is a paucity of literature examining the outcomes of non-operative vs operative intervention among atypical hangman’s fracture patterns. It is also unclear whether outcomes for non-operative vs operative management of these patients are comparable to those of typical hangman’s fracture patients by the Levine and Edwards classification. In the current study, we present the largest single-center cohort of atypical hangman’s fractures with the goal of guiding treatment decisions and outcomes based on fracture classification.
Methods
Patient Population
This is a retrospective analysis of all atypical hangman’s fracture patients treated at a single tertiary Level 1 trauma center between January 2010 and September 2023. This study received IRB approval under Study Protocol 00007981. Informed consent was not required as all patient data was accessed retrospectively in a deidentified manner. Using the radiology Picture Archiving and Communication System (PACS), 85 patients diagnosed with hangman’s fractures treated at our institution between the specified dates were identified. Each patient’s radiographs were reviewed by two independent attending orthopedic spine surgeons at our institution to assess for an atypical pattern. Typical hangman’s fractures were defined as bilateral pars interarticularis fractures without vertebral body involvement. Atypical hangman’s fractures were defined as fractures involving the posterior aspect of the C2 vertebral body with at least unilateral continuity of the posterior cortex or pedicle (Figure 1).
5
55 patients treated for atypical hangman’s fractures were identified. Patients with less than 2 months of follow-up were excluded as this was not sufficient time to assess for fracture healing. 51 patients were ultimately included in the present study. Computed tomography (CT) images demonstrating morphological fracture differences between atypical (A-D) and typical (E-H) hangman's fractures in a 73-year-old woman and an 18-year-old woman, respectively. Midline sagittal (A, E), right parasagittal (B, F), left parasagittal (C, G), and axial images (D, H). The fracture component extending into the posterior cortex of the C2 body (A, D [white arrows]) characteristic of atypical fractures may increase risk of neurologic injury.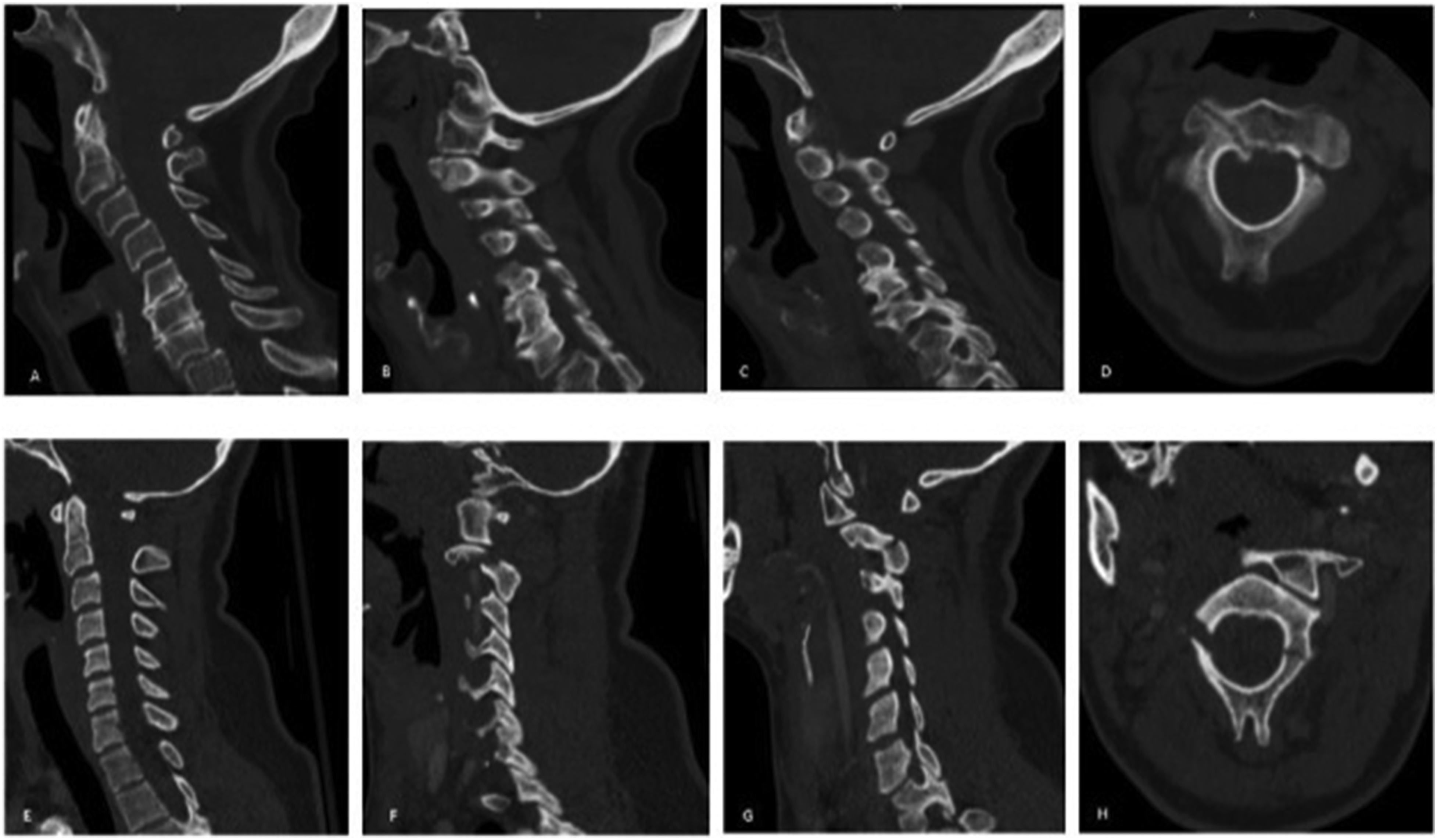
On presentation to our trauma center, all patients were evaluated by either an orthopaedic surgery or neurosurgery resident, either in the emergency department or in an inpatient setting, prior to being staffed with an attending surgeon overseeing the treatment of their atypical hangman’s fracture. All final treatment decisions were made by an attending orthopaedic surgeon or neurosurgeon at our institution.
Demographic data, mechanism of injury, radiographic data at presentation (fracture displacement and angulation), treatment modality (hard cervical collar vs invasive halo immobilization vs surgical intervention), post-treatment radiographic data (fracture displacement and angulation), and time to fracture union were recorded for each patient. Radiographs from the time of presentation were used to determine the Levine and Edwards classification of each patient.
Levine and Edwards Classification Criteria
Upon inclusion in this study, radiographs of all patients with atypical hangman’s fractures were reviewed to determine the appropriate Levine and Edwards Classification for each fracture. Type I fractures were defined as being nondisplaced or having minimal translation (<3 mm of displacement of the C2 vertebral body relative to C3). 14 Type II fractures were defined as having some angulation (<11 degrees) and significant translation (>3.5 mm) of C2 relative to C3. Type IIA fractures were defined as having more severe angulation (>11 degrees) with little to no translation of C2 relative to C3. Our cohort only had Type I, Type II, and Type IIA fractures. Type IIA fractures were classified as Type II fractures for analysis. Type III fractures were defined as having severe angulation and translation of C2 relative to C3 with facet dislocation. No Type III atypical hangman’s fractures were managed at our institution during the duration of this study.
Statistical Analysis
Statistical analyses were performed using Stata16.0 (StataCorp, College Station, Texas). Treatment decisions and outcomes were compared between Type I and Type II atypical hangman’s fractures. Categorical variables were compared using chi-squared tests, and continuous variables were compared using non-parametric Kruskal-Wallis tests. Logistic regression models were used for binary outcomes (mortality, surgery as final treatment, and failure of non-operative treatment requiring surgery). Negative binomial regression models were used for discrete outcomes (length of stay), with incidence rate ratios (IRRs) reported. Linear regression models were used for continuous outcomes (fracture displacement). Statistical significance was set at P < 0.05.
Results
Patient Demographics.
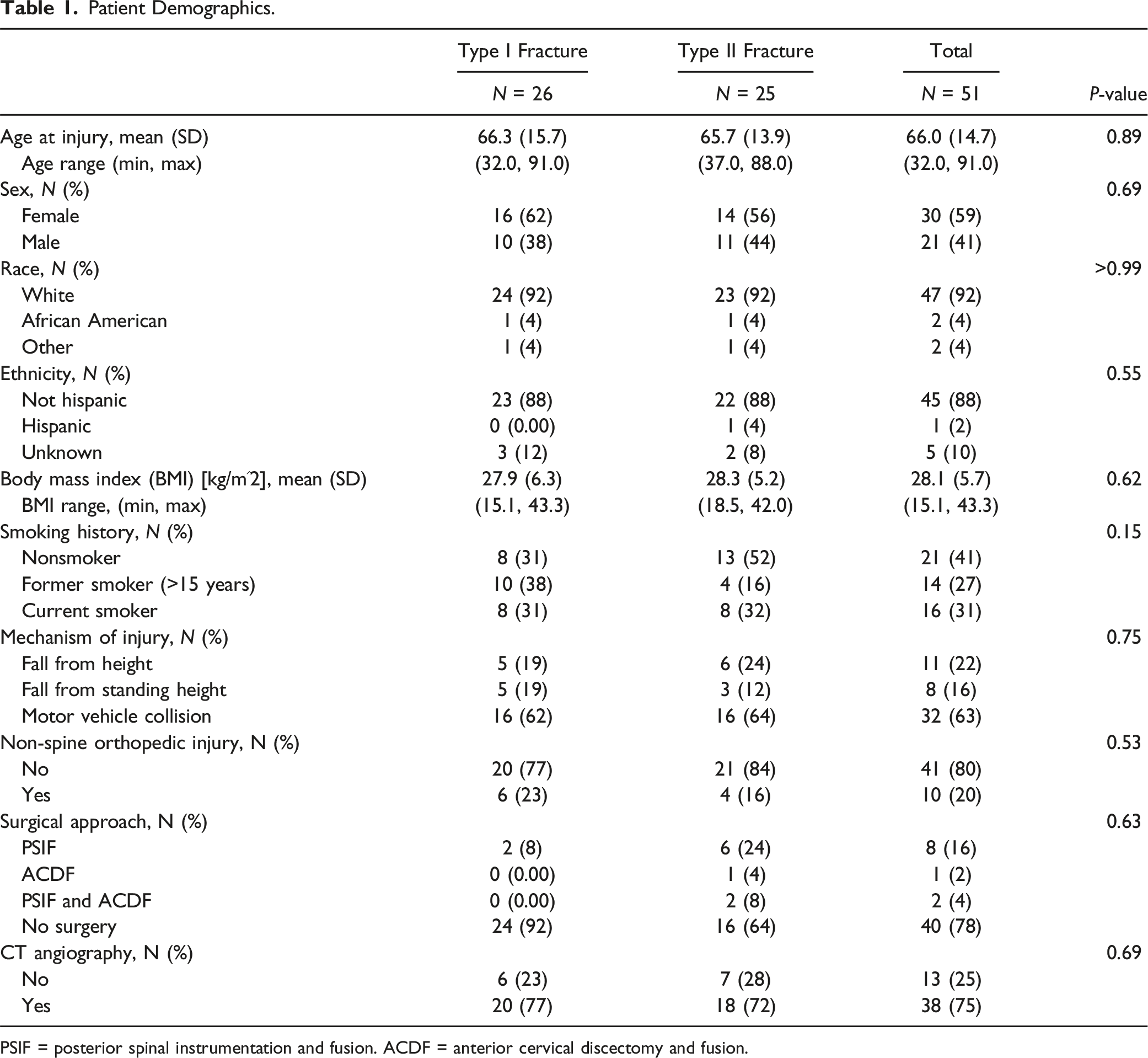
PSIF = posterior spinal instrumentation and fusion. ACDF = anterior cervical discectomy and fusion.
Among patients that underwent surgical intervention in each group, there were no significant differences in the number of levels fused or the surgical approach (i.e. anterior cervical discectomy and fusion (ACDF), posterior spinal instrumentation and fusion (PSIF), or a combined anterior/posterior approach). Across both Type I and II fractures, PSIF (73%) was the most common surgical approach, followed by a combined anterior/posterior approach (18%), and ACDF (9%). Two of three patients who underwent ACDF as initial surgical treatment ultimately required unplanned posterior fixation at a mean of 26 days post-operatively due to concerns regarding residual instability. No patients treated with posterior cervical fusion as initial surgical management were revised. There were no significant differences in rates of computed tomography (CT) angiography between the Type I and Type II fracture groups. All patients across both groups had an American Spinal Injury Association (ASIA) score of E.
Clinical Outcomes.
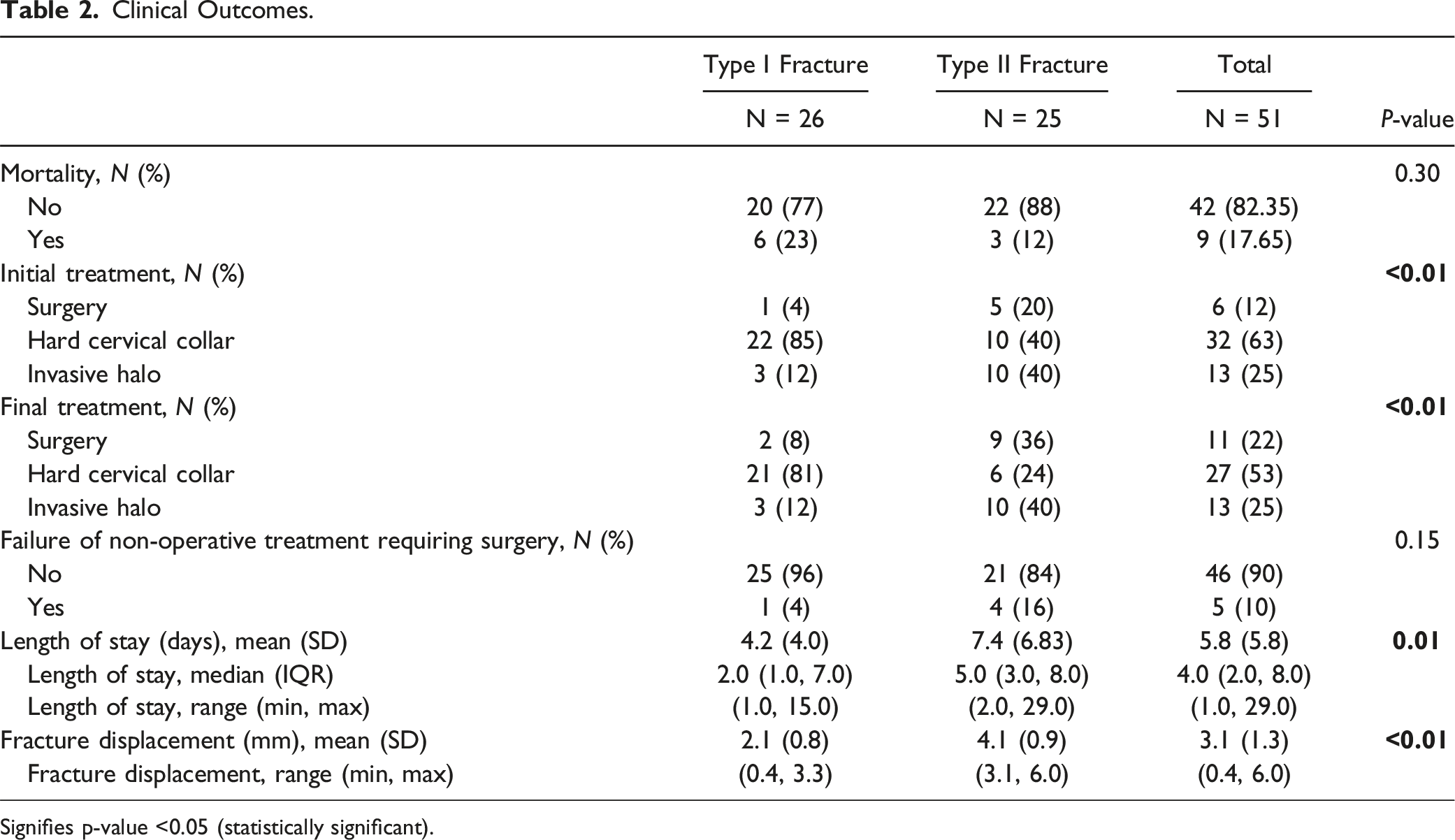
Signifies p-value <0.05 (statistically significant).
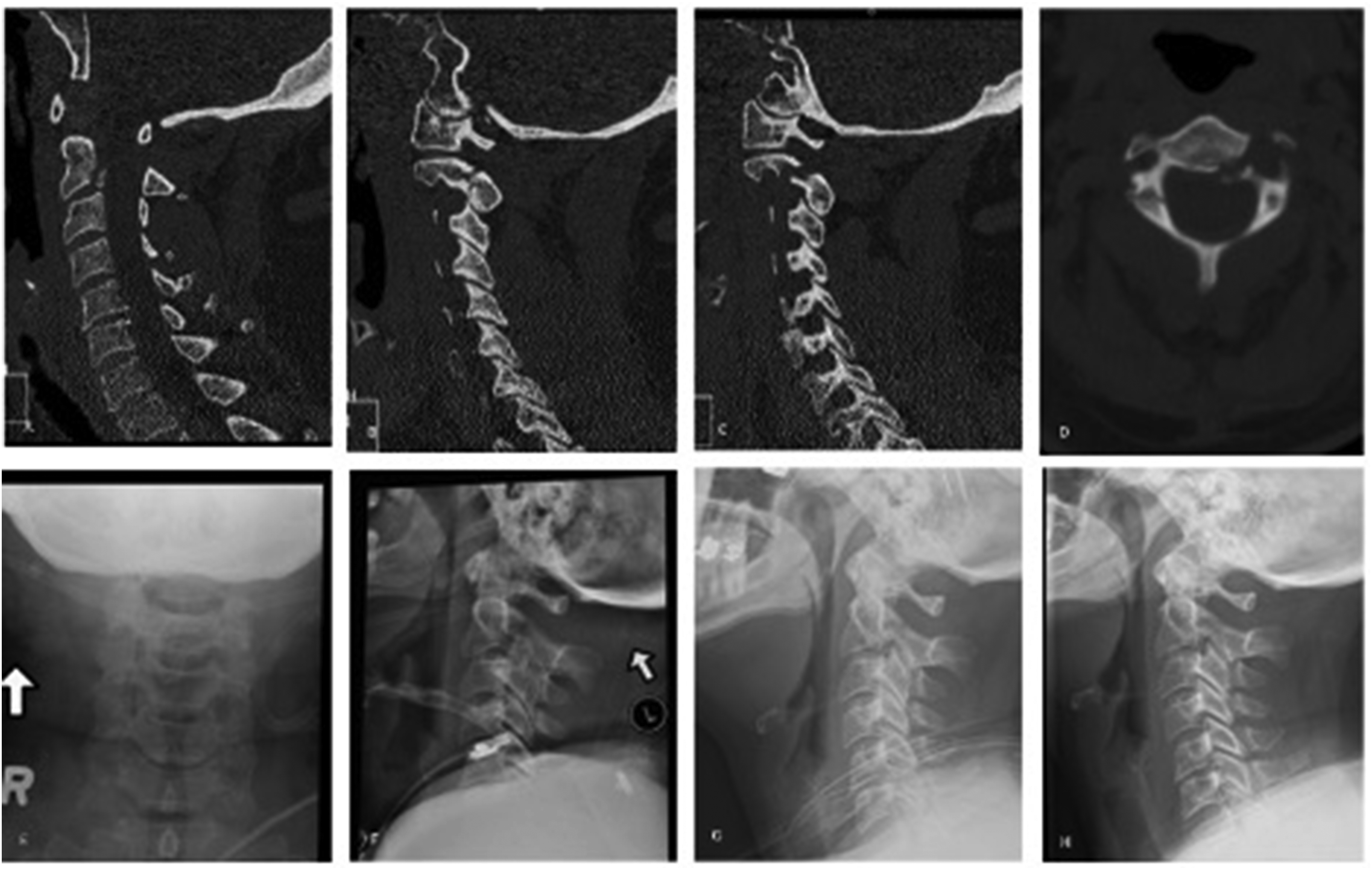
Computed tomography (CT) images and plain radiographs of a 51-year-old female who presented with a Type II atypical hangman’s fracture. Midline sagittal (A), right parasagittal (B), left parasagittal (C), and axial images (D) demonstrate the initial injury. The patient was treated with invasive halo immobilization with appropriate fracture alignment on post-immobilization radiographs (E, F). After 2.5 months of halo immobilization, pre-halo removal (G) and post-halo removal (H) radiographs demonstrate maintained alignment.
Multivariate Regression Analysis for Factors Impacting Outcomes.
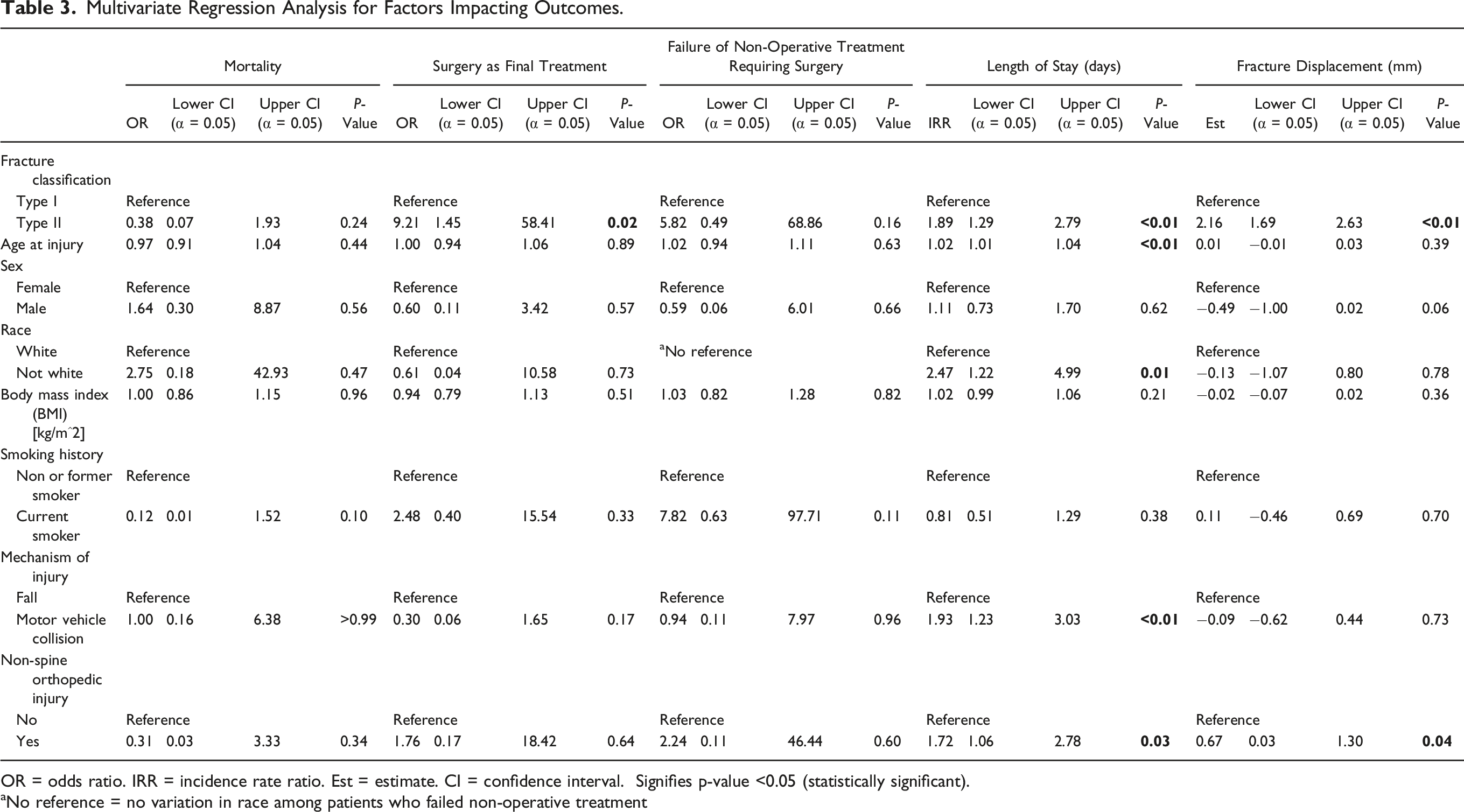
OR = odds ratio. IRR = incidence rate ratio. Est = estimate. CI = confidence interval. Signifies p-value <0.05 (statistically significant).
aNo reference = no variation in race among patients who failed non-operative treatment
Discussion
To date, there have been limited studies discussing the management of atypical hangman’s fractures, with few large single-center cohorts despite atypical fractures comprise a substantial portion of all hangman’s fractures. Atypical hangman’s fractures were first formally described by Starr and Eismont in 1993, with a series of nineteen hangman’s fractures, six of which involved the posterior cortex of the axis body (32%), termed atypical. 5 Notably, atypical fractures had been described four years prior, by Burke and Harris in 1989, who reported 11 fractures involving the posterior cortex of the axis body in a series of 62 hangman’s fractures (11%). However, they were not formally defined as atypical hangman’s fractures at the time. 8 Benzel et al also described these fractures in 1994, referring to them as Type I (coronally oriented) C2 body fractures. 6 More recent studies have revealed atypical fractures may account for anywhere from 18% to 74% of hangman’s fractures, with the largest series identifying 46 atypical fractures of 62 total hangman’s fractures (74%).4,7,9 This study presents the largest cohort of atypical hangman’s fracture patients to date, with 51 of 71 total Hangman’s fracture patients treated at our institution over a thirteen-year period presenting with atypical fractures (72%). It is important to note that the term “atypical hangman’s” may be used differentially within the literature to describe this fracture pattern. Other commonly used terms include axis body fractures or miscellaneous axis fractures.15,16
The mechanism of injury of typical hangman’s fractures varies between subclassifications. Type I injuries result from extension-axial load mechanism, which leads to an axis fracture, and do not disturb the C2-C3 disk nor the anterior or posterior ligaments. 2 Type II fractures are usually caused by the combined mechanism of extension-axial loading followed by flexion-compression loading. On advanced imaging patients with Type II fracture patterns tend to have disk space widening and the high possibility of an associated ligamentous injury. 2 A flexion-compression mechanism is often associated with Type III injuries, which leads to bilateral pars interarticularis fracture, and bilateral facet dislocation. 2 The morphological difference between typical and atypical hangman’s fractures is attributed to the cervical spine alignment during injury, which leads to variation of fracture patterns associated with atypical hangman.2,3
While the management of typical hangman’s fractures has been more extensively described in the literature, it is unclear whether atypical hangman’s fractures should be managed in the same way, given the increased risk of associated neurologic injury with atypical fractures due to the involvement of the posterior portion of the vertebral body. Historically, stable typical hangman’s fractures, such as most Type I and many Type II fractures, have been managed non-operatively with hard cervical collars or invasive halo immobilization.17-21 Unstable Type II, i.e. Type IIa, and Type III fractures are typically managed operatively.2,21-23 In our cohort, we examined the management and outcomes of Type I vs Type II atypical hangman’s fracture patients to elucidate indications for non-operative vs operative management and examine differences in outcomes.
The majority of Type I fracture patients were initially managed non-operatively, with only one patient managed surgically initially and one patient failing hard collar treatment and requiring surgery for delayed fracture union. Furthermore, most of these patients were managed with a hard cervical collar as opposed to invasive halo immobilization. Therefore, atypical Type I hangman’s fractures, with minimal fracture displacement, may be successfully managed non-operatively with a hard cervical collar, as is the case for typical Type I hangman’s fractures. 11 These patients should be followed carefully, however, as there is still a risk of further fracture displacement, incomplete fracture union, or delayed neurologic compromise that may result in these patients requiring subsequent surgical management.4,5
Initial and final management of atypical Type II fractures, however, were far more heterogeneous as compared to the Type I fracture group. While the majority of Type II fracture patients were also treated non-operatively, most of the non-operative patients were managed with invasive halo immobilization as opposed to a hard cervical collar. Additionally, a far greater proportion of Type II fracture patients were managed surgically initially, and nearly half of the patients initially managed with a hard cervical collar in this cohort subsequently underwent surgery due to failed fracture healing. No patients that were initially managed with invasive halo immobilization subsequently required surgery. Given that nearly half of the atypical Type II fracture patients initially managed with a hard cervical collar subsequently required surgery, it may be beneficial to pursue a more aggressive management strategy for these patients as they may be more likely to require invasive halo immobilization or surgical intervention as compared to typical Type II fracture patients. While previous reports have shown that healing in a malunion position with anterior displacement may not be harmful in typical hangman’s fractures, it should be a greater concern in atypical fractures due to the increased risk of neurologic injury.14,24,25 Therefore, we recommend strong consideration of invasive halo immobilization for atypical Type II fracture patients as an initial treatment modality, if non-operative treatment is pursued.
For surgically managed patients, there was a clear pReference for PSIF over ACDF or a combined anterior/posterior approach. This is consistent with prior literature showing increased prevalence of posterior approaches for surgical management in typical Type I and II fractures.9,14,16,22Additionally, within our study, two of the three patients treated with ACDF required early, unplanned posterior fixation due to residual instability, while no patients treated with posterior fixation as initial management required revision. Though this was not a significant difference, this finding may indicate that an ACDF has an increased risk of requiring additional surgery. Combined anterior/posterior approaches are typically reserved for cases of more severe anterior displacement of C2 relative to C3. 26 Unfortunately, beyond these observations it is difficult to establish any conclusions regarding surgical management as only a small subset of patients in this case series were treated surgically. In general, most atypical hangman’s fractures may be treated successfully with non-operative treatment.
Limitations
The major limitation of this study is it’s retrospective, single-center design. This may limit generalizability and cause challenges when attempting to infer causality. The limited population size also may cause challenges with regards to statistical power. Additionally, due to large variation in follow-up time, it is possible that some post-operative complications or incidences of failed fracture healing were missed and therefore may be underrepresented in this study. A larger sample size and extended follow-up period may help to further elucidate the differences in outcomes of the various treatment options for atypical Type I and II hangman’s fractures. Furthermore, multicenter studies are needed to control for surgeon bias in treatment selection.
Conclusions
Atypical hangman’s fractures may require different treatment considerations than typical hangman’s fractures given the increased risk of spinal cord injury due to the involvement of the posterior cortex of the axis body. While atypical Type I fractures may be managed effectively non-operatively with a hard cervical collar, atypical Type II fractures may require more aggressive management with invasive halo immobilization or surgery. Atypical Type II fractures managed non-operatively with a hard cervical collar are at greater risk of requiring subsequent surgical intervention. Therefore, treatment with a hard cervical collar may not be as effective for these patients and we recommend strong consideration of invasive halo immobilization for these patients as an initial treatment if non-operative treatment is pursued. In general, most atypical hangman’s fractures may be treated successfully with non-operative treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Statement
This study received IRB approval under Study Protocol 00007981.