
Abstract
Study Design
Case series.
Objective
We report the unusual occurrence of vertebral artery injury (VAI) during routine posterior exposure of the cervical spine. The importance of preoperative planning to identify the course of the bilateral vertebral arteries during routine posterior cervical spine surgery is emphasized.
Methods
VAI is a rare but potentially devastating complication of cervical spinal surgery. Most reports of VAI are related to anterior surgical exposure or screw placement in the posterior cervical spine. VAI incurred during posterior cervical spinal exposure surgery is not adequately addressed in the existing literature. Two cases of VAI that occurred during routine posterior exposure of the cervical spine in the region of C2 are described.
Results
VAI was incurred unexpectedly in the region of the midportion of the posterior C1–C2 interval during the initial surgical exposure phase of the operation. An aberrant vertebral artery course in the V2 anatomical section in the region between C1 and C2 intervals was identified postoperatively in both patients. A literature review demonstrates a relatively high incidence of vertebral artery anomalies in the upper cervical spine; however, the literature is deficient in reporting vertebral artery injury in this region. Recommendations for preoperative vertebral artery imaging also remain unclear at this time.
Conclusions
Successful management of this unexpected complication was achieved in both cases. This case report and review of the literature highlights the importance of preoperative vertebral artery imaging and knowledge of the course of the vertebral arteries prior to planned routine posterior exposure of the upper cervical spine. In both cases, aberrancy of the vertebral artery was present and not investigated or detected preoperatively.
Introduction
Vertebral artery injury (VAI) is a rare but potentially devastating complication of cervical spinal surgery. Most reports of VAI are related to anterior surgical exposure or screw placement in the posterior cervical spine. VAI incurred during posterior cervical spinal exposure surgery is not adequately addressed in the existing literature. Two cases of VAI that occurred during routine posterior exposure of the cervical spine in the region of C2 are described.
Case Reports
Case 1
A 69-year-old man presented with a 3-month history of progressive cervical myelopathy. He was noted to have multilevel subaxial cervical spinal stenosis and C1–C2 stenosis (Fig. 1). The patient's preoperative magnetic resonance imaging (MRI) and computed tomography (CT) sagittal images demonstrated an abnormal posterior course of the V2 segment of the right vertebral artery (Fig. 2A, B). An injury of this anomalous vertebral artery segment occurred during routine posterior surgical exposure. Profuse and uncontrollable arterial bleeding was unexpectedly encountered in the region of the midportion of the posterior C1–C2 interval. The patient lost 1,900 mL of blood during the surgical exploration and repair of the injured vertebral artery. Intraoperative direct repair of the injury was successfully performed by the on-call vascular surgeon using 6–0 Prolene sutures (Ethicon, Inc., Ontario, Canada) (Fig. 3). Due to the significant loss of blood, the surgical plan was altered, and an uninstrumented subaxial cervical laminectomy only was performed after vessel repair. The patient had an uneventful postoperative course without clinical evidence of VAI or postlaminectomy kyphosis (Fig. 4). The stenosis in the C1–C2 region was not addressed. Despite the persistence of the C1–C2 stenosis, he demonstrated fair recovery from his clinical myelopathy at 6 months postoperatively.

Preoperative sagittal computed tomography image of a 69-year-old man with multilevel cervical spinal stenosis and C1–C2 stenosis.
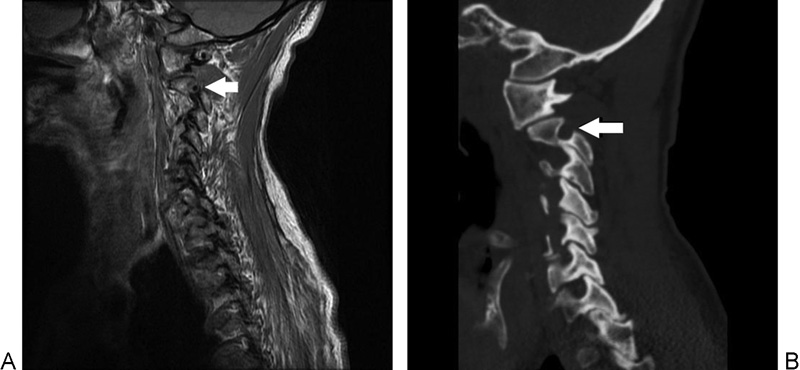
(A, B) Sagittal magnetic resonance imaging and computed tomography showing abnormal course of posterior right V2 segment of the vertebral artery (arrow).
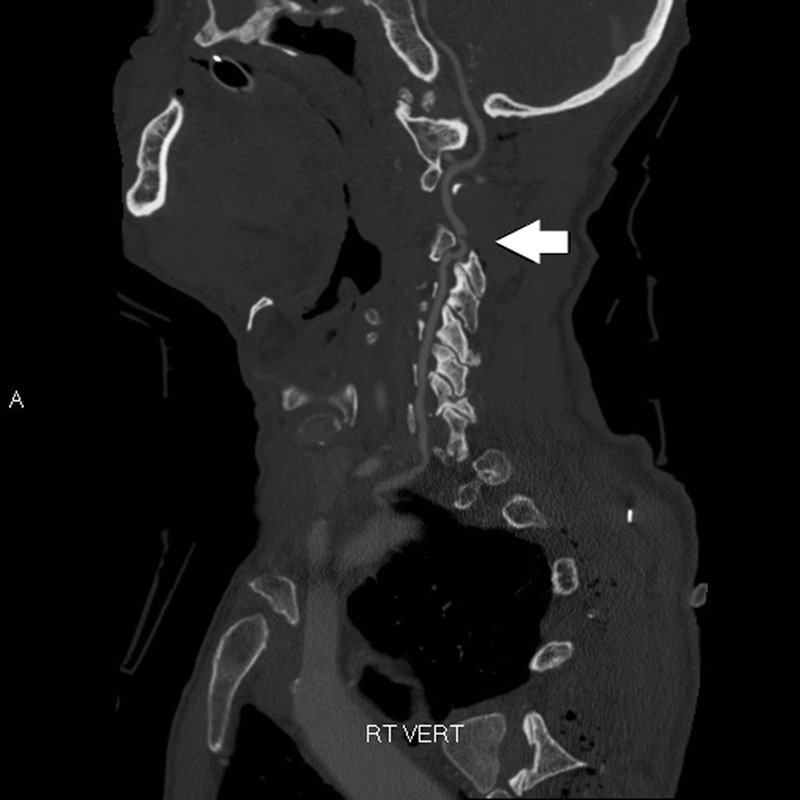
Postoperative sagittal computed tomography angiogram demonstrating patency across the vertebral artery injury repair site.
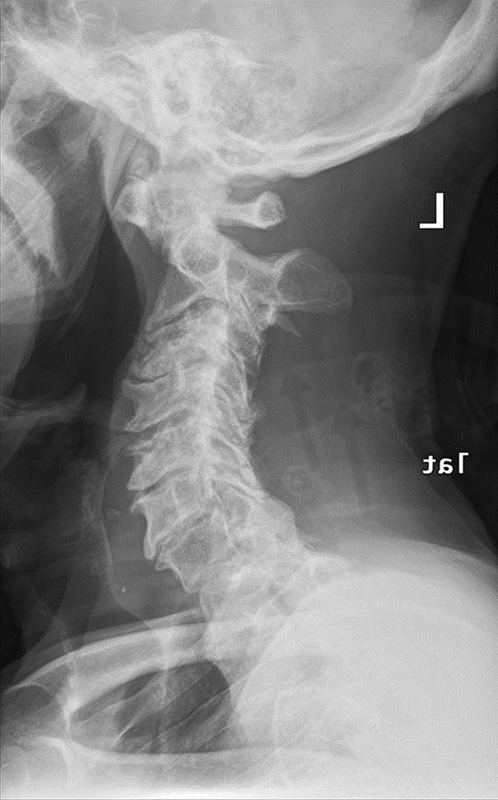
Six-month postoperative lateral radiograph showing persistent C1–C2 stenosis and maintained sagittal alignment.
Case 2
An 83-year-old man presented with a displaced type II odontoid fracture after a fall down three steps. The patient was noted to be neurologically normal on initial examination. X-ray and CT imaging studies demonstrated a type II odontoid fracture with 7 mm of posterior displacement. The patient was taken to the operating room for a planned C1–C2 posterior spinal instrumented fusion. Preoperative cervical MRI imaging was not performed. Preoperative neuromonitoring was utilized, and the patient was placed in the prone position for surgery. During the routine posterior surgical exposure of the midportion of the left posterior C1–C2 joint, profuse and uncontrollable arterial bleeding was encountered. An injury to an unrecognized anomalous posterior vertebral artery segment located between the C1–C2 interval was incurred with bovie electrocautery. After multiple attempts, direct repair of the injured vertebral artery segment was unable to be achieved. The patient lost 2,300 mL of blood prior to successful suture ligation of the injured vertebral artery segment. Fig. 5 illustrates the anatomic anomaly.
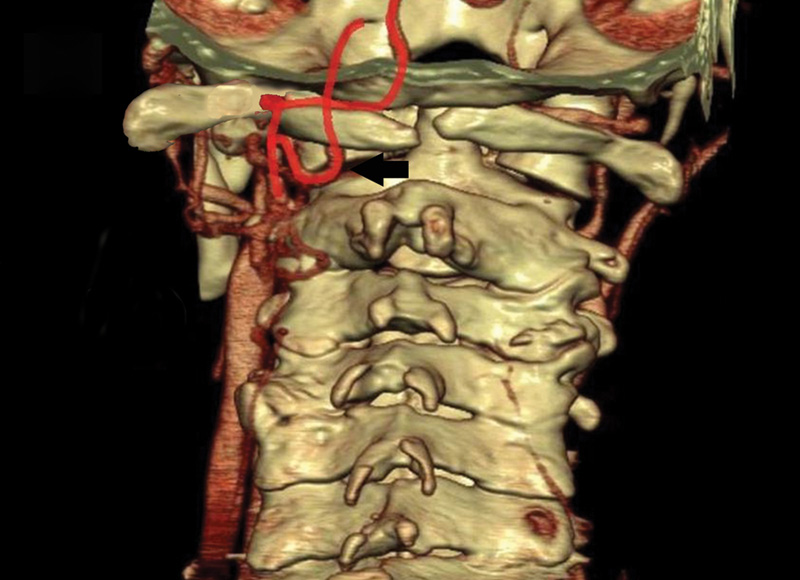
Illustration depicting well-described persistent first intersegmental artery V2 segment vertebral artery anomaly in the midregion of the posterior C1–C2 joint. 18
Postoperatively, the patient awakened neurologically normal without clinical evidence of VAI. CT angiogram after surgery revealed the complete injury to an anomalous V2 segment of the vertebral artery. A vascular surgery consultation was obtained postoperatively, and the patient was evaluated. The patient was discharged home on aspirin for 3 months. At 6 months postoperatively, his injury was stable and he remained neurologically normal.
Discussion
VAI is a rare but potentially devastating complication of cervical spinal surgery. Unexpected VAI may result from poor surgeon preoperative planning along with the failure to recognize an abnormal vertebral artery course preoperatively. The profuse degree of vertebral artery bleeding encountered with injury may result in excessive blood loss and hypotension. Fortunately, in many cases the bleeding may be controlled with topical hemostatic agents, direct vessel repair, or ligation. Mortality may occur in instances where bleeding cannot be adequately addressed in a timely fashion.
Aberrant vertebral artery anatomy is often cited in published cases of VAI during cervical spine surgery 1 , 2 , 3 , 4 ; however, it remains frequently unrecognized prior to surgery. The existing literature includes several reports identifying and describing anomalous courses of the vertebral artery in the cervical spine. 5 , 6 , 7 , 8 , 9 , 10 A tortuous anterior course of the vertebral artery V5–V3 segments has been described by Curylo et al and occurs in ∼5.5% of subjects. 5 Several reports of injury to the vertebral artery during anterior cervical decompression surgery exist in the literature. 1 , 2 , 11 The present study describes two patients who sustained VAI during routine upper cervical spine posterior exposure in the midline region of C2. To our knowledge, the unusual occurrence of VAI during routine posterior surgical spine exposure surgery in the upper cervical spine has not been previously reported.
Most reports of VAI are related to anterior surgical exposure or screw placement in the posterior cervical spine. The reported incidence of VAI during cervical spine surgery ranges from 0.20 to 1.96%. 1 , 2 , 4 , 11 , 12 , 13 , 14 Molinari et al recently published a systematic review of the topic of VAI in spinal surgery, which revealed a paucity of published literature addressing the topic. 15 Burke et al reported six cases of VAI in anterior corpectomy surgery. 1 Three patients were treated with primary repair or ligation, and no postoperative complications were noted with these patients. Bleeding from the injured vertebral artery was controlled with hemostatic agents in the other three patients, and two of these patients experienced postoperative complications. 1 Surgeons should always consider primary vertebral artery repair or ligation, even when control of the vertebral arterial bleeding is achieved with hemostatic agents, due to the risk of pseudoaneurysm or rebleeding. Other studies have reported VAI rates of 0.10 to 1.96%, depending on the type of anterior cervical spine procedure. 1 , 15 , 16
Reports of VAI with posterior surgery have been described; however, these typically involve injury incurred during the instrumentation phase of the posterior surgery. Magerl and Harms screw techniques are associated with injury rates of 0 to 8% and 0 to 5%, respectively. 14 Only a single case report describing VAI during wide subaxial posterior cervical spine surgical exposure was identified. The patient had an uneventful outcome after resection of the lateral mass and tamponade of the VAI. 17 None of the studies reporting VAI identified the importance of obtaining preoperative imaging to identify anomalous or tortuous vertebral arteries.
The Cervical Spine Research Society recently published the results of a VAI questionnaire provided to its members. 16 A 0.07% overall incidence of surgical VAI (111/163,324) was reported among members. One-fifth (22/111) of all injuries involved an anomalous course of the vertebral artery. The most common management was by direct tamponade. The outcomes of VAIs included no permanent sequelae in 90% of patients, permanent neurologic sequelae in 5.5%, and death in 4.5%. The surgeon's level of experience was noted to be inversely related to the frequency of VAI. Surgeons who had performed 300 or fewer cervical spine surgeries in their career had a VAI incidence of 0.33% compared with a 0.06% rate in surgeons with more than 300 lifetime cases. The questionnaire did not address the routine use of preoperative imaging studies to evaluate the course of the vertebral artery prior to planned surgery.
Both VAIs in our study were incurred in the posterior region of the C2 midlateral mass interval. An aberrant course of one of the vertebral arteries in this region was present in both patients. Variations in the course of the vertebral artery at the craniovertebral junction have been described and tend to follow predictable patterns. 7 , 18 The most common variant is a persistent first intersegmental artery that arises from the embryonic first intersegmental artery. This aberrant vertebral artery takes an anomalous course and enters the spinal canal between C1 and C2. A recent magnetic resonance arteriogram study has shown this aberrant artery to be present in 3.2% of patients. 8 It is likely that the persistent first intersegmental artery anomaly was the source of injury at the C1–C2 interval in the second case presented in this report. Posterior vertebral artery anomaly in the form of a right persistent first intersegmental artery in the region of the right posterior C1–C2 lateral mass interval has been well described in the literature. 7 , 8 , 9 , 19 Uchino et al have reported a persistent first intersegmental artery in up to 3.2% of normal subjects and an overall prevalence of craniovertebral junction vertebral artery anomalies of 5%. 9 In both cases described in this report, dedicated preoperative vertebral artery imaging was not performed. This particular vertebral artery anomaly poses great risk to the conventional placement of C1 lateral mass screws through previously described techniques involving the exposure of the C1 lateral mass or placement of the screw through the C1 posterior ring.
In addition to identifying the course of the bilateral vertebral arteries preoperatively, surgeons who perform routine posterior cervical exposure should have a thorough working knowledge of options regarding repair, mobilization, and ligation of VAIs. Surgical access to the VAI site while controlling local bleeding can be very difficult. Blood loss is often excessive when access to the injury site is delayed or impaired. Repair by suture to maintain vertebral artery patency is the preferable treatment if the injured vertebral artery can be exposed from an expanded approach. 15 If the arterial injury is in the bony canal, however, adequate access for repair may not be possible. In such cases, tamponade may be the most appropriate treatment option. Ligation of the injured vertebral artery without adverse consequence has been described in multiple patients. 15 , 17 The use of intraoperative and postoperative embolization in cases of intraoperative VAI is becoming more common in clinical practice. Bilbao et al reported successful embolization for the treatment of intraoperative VAI. 11
The two cases presented in this report highlight the need for proper preoperative planning with respect to knowledge of the anatomic course of the bilateral vertebral arteries. Eskander et al described a comprehensive preoperative vertebral artery classification system that is useful to surgeons for preoperative planning. 6 This classification system uses preoperative MRI and enables surgeons to detect and grade vertebral artery anomalies in an organized manner. The grading system classifies the anatomic position of the vertebral artery bilaterally with respect to intraforaminal midline migration, extraforaminal abnormal entrance of the cervical spine, and arterial side dominance. The authors suggest that the preoperative classification of vertebral artery positon should become an integral portion of the cervical spine surgeons’ preoperative routine. Furthermore, the identification of the intraforaminal anomaly subcategory that involves midline vertebral migration potentially places the vertebral artery at the most risk during routine corpectomy surgery. Also, VAI during a routine posterior or anterior approach may occur with extraforaminal anomalies related to a vertebral artery entering the transverse foramen at a level other than C6. In addition to aberrancy in course, vertebral artery side dominance is also addressed with the preoperative classification system proposed by Eskander et al. 6 Arterial patency anomalies include fenestrated, hypoplastic, or absent arteries. Preoperative identification of patency aberrancy is extremely important to maintain cerebral perfusion in the setting of damage to one of the vertebral arteries with the presence of contralateral arterial abnormality. The prevalence of these vertebral artery anomalies as seen on MRI was noted to be 7.6% for fenestrated, 8% for hypoplastic, and 10% for absent arteries, respectively, in 250 normal subjects. 6
The significance in this case report and review of the literature lies in the identification of the risk of complication involving VAI through a posterior cervical surgical exposure. Much of the existing literature involving VAI in cervical spinal surgery has focused on injuries incurred with anterior cervical spinal surgical procedures. A review of the literature identifies a relatively high prevalence of vertebral artery anomalies at the craniovertebral junction. 8 , 18 , 20 Published reports indicate that this particular anomaly rate may be as high as 5%. 7 , 18 The utility of routine preoperative imaging studies to demonstrate the course of the bilateral vertebral arteries prior to any planned exposure of the craniocervical junction is clearly noted in this case report. Further discussion and investigation involving the routine use of preoperative imaging studies to detect the course of bilateral vertebral arteries prior to upper posterior cervical spine surgery is warranted.
Disclosures
Robert W. Molinari, none
Peter C. Chimenti, none
William Gruhn, none
Robert Molinari, Jr., none
Perioperative VAI during cervical surgery remains a feared, albeit rare complication marked by some uncertainty in terms of diagnostic and therapeutic responses. There is no disagreement that prevention of VAI remains a universally accepted primary counterstrategy. Molinari et al present two cases, which, in retrospect, might have been avoidable with closer scrutiny to some of the telltale imaging signs of vascular anomalies. The use of CT in addition to MRI may help in detecting unusual bony apertures or recesses harboring blood vessels that could possibly have changed the surgical exposure strategy.
Both the authors of the case report and our commentator, Dr. Monteith, recommend increasing the awareness of spine practitioners and neuroradiologists by developing more focus on telltale signs of vascular anomalies, and for clinicians to then follow up where clinically relevant with a CT angiography, MRI angiography, and/or interventional angiography in select patients. Perhaps increasing the use of CT to supplement surgical management of less than straightforward cervical spine surgery could improve recognition of vascular anomalies at the cost of increased radiation exposure to patients and health care resource utilization.
The article also raises the question of the optimal management of intraoperative vertebral artery injuries. Open ligation, tamponade, repair, and delayed interventional care either with embolization or revascularization of these rare complications remain largely empirically driven treatment responses with substantial variations based on practitioner experience and available resources. In light of the relative reported rarity of VAI, a registry-based investigation of this complication and subsequent patient outcomes might offer the best chance for advancement of our knowledge base. Concerned societies such as AOSpine, Cervical Spine Research Society, and the Scoliosis Research Society could make a real difference with a well-constructed database of rare complications. For now, Evidence-Based Spine-Care Journal and Global Spine Journal thank the authors for their candor in reporting this complication and for the quality discussion provided by our commentator.