
Abstract
Study Design
Prospective observational study.
Objective
To determine whether preference-based health utility scores for common spinal radiculopathies vary by specific spinal level.
Methods
We employed a standard gamble study using the general public to calculate individual preference-based quality of life for four common radiculopathies: C6, C7, L5, and S1. We compared utility scores obtained for each level of radiculopathy with analysis of variance and t test. Multivariable regression was used to test the effects of the covariates age, sex, and years of education. We also reviewed the literature for publications reporting EuroQol-5 Dimensions (EQ-5D) scores for patients with radiculopathy.
Results
Two hundred participants were included in the study. Average utility for the four spinal levels fell within a narrow range (0.748 to 0.796). There were no statistically significant differences between lumbar and cervical radiculopathies, nor were there significant differences among the different spinal levels (F = 0.0850, p = 0.086). Age and sex had no significant effect on utility scores. There was a significant correlation between years of education and utility values for S1 radiculopathy (p = 0.037). On review of the literature, no study separated utility values by specific spinal level. EQ-5D utilities for both cervical and lumbar radiculopathy were considerably lower than the results of our study.
Conclusions
Utility values associated with the most common levels of cervical and lumbar radiculopathy do not significantly differ from each other, validating the current practice of grouping utility by spinal segment rather than by specific root levels. The discrepancy in average utility values between our study and the EQ-5D highlights the need to be mindful of the underlying instruments used when assessing outcomes studies from different sources.
Introduction
Spine-related ailments are a major cause of morbidity and lost productivity in the United States, affecting nearly 33 million people per year. 1 Although multiple spine-related symptoms often coexist, the individual symptomatic components can be broadly divided into those that cause axial pain, central neural dysfunction (myelopathy, neurogenic claudication), and nerve root dysfunction (radiculopathy). The term radiculopathy refers to the varying degrees of pain, sensory changes, and motor weakness associated with irritation of spinal nerves.
Etiologies of radiculopathy are numerous and include compression from herniated intervertebral disks, degenerative overgrowth, spinal instability, and certain autoimmune and metabolic disorders. 2 , 3 , 4 , 5 It is a common condition, affecting up to 5% of the population, with equal distribution among men and women. 6 The most common nerve roots affected in the cervical spine are C6 and C7, and extrapolating from the literature on herniated lumbar disks, the majority of lumbosacral radiculopathies are L5 and S1. 7 , 8 The treatment includes both nonoperative modalities (e.g., physical therapy, epidural steroid injections) and surgical intervention, depending on the causal pathophysiology, degree of debilitation, and duration of symptoms.
The most common surgical treatment for radiculopathy involves decompression of the affected nerve root by removing variable amounts of bone, ligament, and herniated disk material. This treatment constitutes the fifth most commonly performed surgery in U.S. hospitals with over 500,000 performed annually,9 a figure that does not include the scores of patients with recalcitrant radiculopathy treated with spinal fusion surgery. Spinal fusion is the single most expensive surgical procedure in terms of aggregate costs, accounting for $12.8 billion spent on index hospitalization costs in the United States annually.9 Therefore, it is no surprise that these procedures have been subject to numerous comparative and cost-effectiveness studies.
The primary outcome instruments used in effectiveness studies quantify three major categories of patient-reported outcomes: global health-related quality of life (HRQoL), pain, and disease-specific disability. Although multiple disease-specific disability instruments exist for spinal conditions, such as the Oswestry Disability Index for low back pain and the Neck Disability Index for neck pain, there is no widely used radiculopathy-specific disability instrument. Pain is highly subjective and varies tremendously from patient to patient, thus the most reliable tools with which to compare patients with radiculopathy are global HRQoL instruments.
Global HRQoL Instruments and Valuation Techniques
“Preference-based” instruments are a specific subtype of HRQoL measures used to derive utility scores, which generally range from 0 (death) to 1 (perfect health), although negative numbers may be reported and reflect health states deemed to be worse than death. 10 The utility scores obtained from these instruments are generated from studies of the general public employing valuation techniques such as the visual analog scale (VAS), time trade-off (TTO), and standard gamble (SG) methods. 11 Because the general public is surveyed, rather than only individuals afflicted with the specific disease state, such studies provide a “societal perspective” of utility.
The VAS is a line with two anchors usually being death (e.g., 0) and perfect health (e.g., 100) and asks responders to rate various health states as a single mark on the line. The TTO method presents the participant with a written description of a health state under evaluation and then presents the hypothetical choice of living for X years in the described state, or a shorter amount of time, Y years, in perfect health. The utility of the described health state is Y/X. For example, if the participant would rather live 5 years in perfect health than 10 years with severe low back pain, the utility for severe low back pain would be 5/10 = 0.5.
Finally, the SG method presents participants with a choice of two alternatives: (1) a definite health state A (e.g., severe low back pain) and (2) a hypothetical gamble, resulting in two possible health states (usually perfect health, B, or death, C). Participants are asked what probability of death they would accept for a chance at perfect health. For example, if the responder was indifferent between having severe low back pain (A) and a 30% probability of death, the utility of the severe low back pain state would be 1 − C = 0.7.
“Direct measures” of utility involve surveying participants directly using the above valuation techniques, and “indirect measures” of utility take the form of standardized surveys not specific to any particular disease. The two most commonly used indirect utility instruments in the spine literature are the EuroQol-5 Dimensions (EQ-5D) and Short-Form (SF) surveys. The SF surveys have multiple iterations, the most common of which is the non-preference-based SF-36. The shorter, preference-based SF-6D was developed to directly generate utility scores, and because they involve the same questions, the SF-36 can be mapped to the SF-6D to derive utility scores. Utility values for these instruments depend on population-specific value sets used to derive the score. For the EQ-5D U.S. (n = 4,048) and United Kingdom (n = 3,395) value sets, scoring was performed using a TTO method.12,13 The original SF-6D value set was developed using a SG study of 611 United Kingdom participants. 14 Studies on nonspinal diseases, such as coronary artery disease and osteoarthritis, have identified that utility values can vary widely between the two instruments and therefore they may not be interchangeable. 15 , 16
Because of the disparate utility values generated from different instruments, researchers must specify which instrument was used to generate the data. In a similar vein, it may be useful for outcomes studies on radiculopathy to delineate the specific radiculopathies being treated and their associated utility values because different levels of radiculopathy present with different symptoms and disability. Although many studies present a breakdown of the affected spinal levels, they do not distinguish whether there are differences in utility by level, but rather group all patients as either having or not having radicular symptoms in a certain spinal segment (cervical, thoracic, lumbar). It is possible that different levels of radiculopathy (e.g., C6 versus C7) may be associated with different utility values, which would have implications for comparative outcomes research.
To clarify this void in knowledge, we conducted an SG study on the general public (a direct measure of utility) to assess the preference-based health utility between specific levels of spinal radiculopathy and compared our results to indirectly measured utility values identified in the literature.
Materials and Methods
We employed the SG approach to calculate the individual preference-based HRQoL (utility values) for various radiculopathies.17 Randomly chosen individuals on and around the campus of the University of Pennsylvania (community members) were interviewed and presented scenarios for each of four radiculopathies: C6, C7, L5, and S1. These scenarios (
We calculated the means and standard deviations for the utility scores obtained for each of the four radiculopathy levels. The utility values of the different spinal levels were compared using analysis of variance with the Bonferroni correction for multiple comparisons. The adjacent levels within each spinal segment (cervical, lumbar) were compared using the Student t test. Multivariable linear regression was used to test the effects of the covariates age, sex, and years of education for each radiculopathy. All statistical analyses employed Stata v.12 (StataCorp, College Station, Texas, United States). Differences for which the probability was <0.05 were considered significant.
We also reviewed the literature for publications reporting EQ-5D utility scores for patients with cervical and lumbar radiculopathy. We limited our search to PubMed-indexed English-language articles published between 2000 and December 2014 that contained preoperative utility scores. We supplemented the search by using the “Related Articles” feature of PubMed and by manually searching the bibliographies of selected articles. If multiple studies were published from the same institution or utilizing the same database, only the largest study was included to avoid redundancy.
Results
Two hundred community members were interviewed and included in the study; the demographics are summarized in Table 1. The average participant was 36.7 years with 16.2 years of education. The results of the SG for the four levels of radiculopathy are summarized in Table 2. The average utility values for the four spinal levels fell within a narrow range (0.748 to 0.796), with L5 radiculopathy resulting in the lowest utility and C7 radiculopathy resulting in the highest utility. There were no statistically significant differences in utility between lumbar and cervical radiculopathies, nor were there significant differences among the different spinal levels (F = 0.0850, p = 0.086). Correlations between the demographic factors and utility for each radiculopathy are summarized in Table 3. Sex and age had no significant effect on utility scores. There was a significant correlation between years of educations and the utility values for S1 radiculopathy (p = 0.037), as illustrated in Fig. 1.
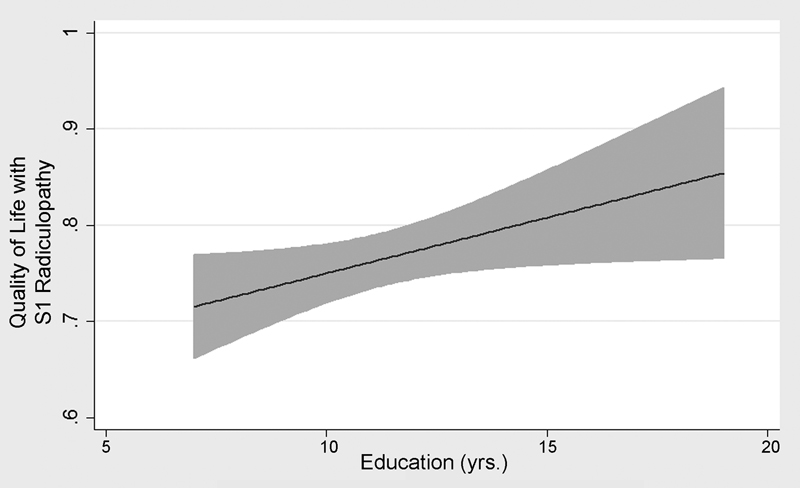
Linear regression of quality of life with S1 radiculopathy, plotted against years of education of interviewee. The line represents the fitted mean values, the gray area the 95% confidence intervals.
Demographics of subjects
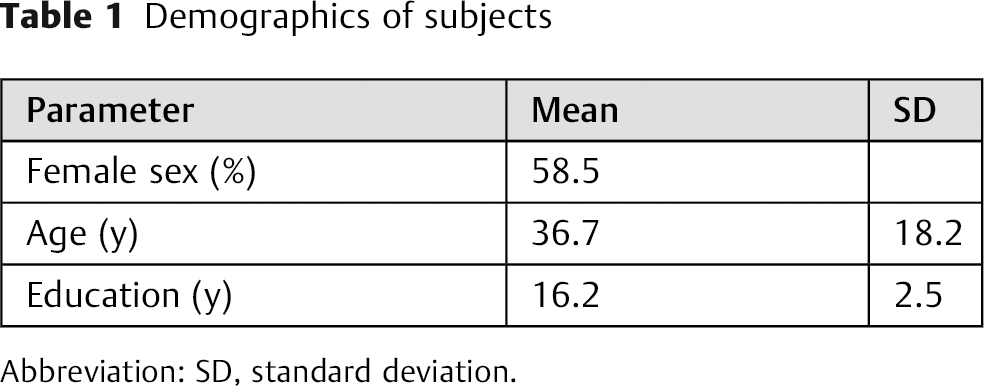
Abbreviation: SD, standard deviation.
Utility of radiculopathy
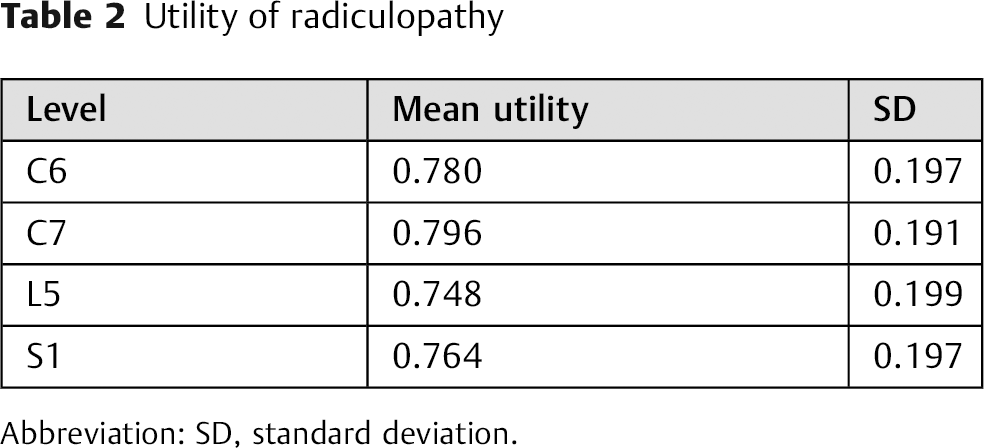
Abbreviation: SD, standard deviation.
Correlations with utility (p value)

Multiple studies were identified with preoperative EQ-5D utility data for patients with radiculopathy and are detailed in Table 4. No study separated the utility values by specific spinal levels. For the EQ-5D, the median ages of subjects with lumbar and cervical radiculopathy were 44 and 49.3, respectively. The average preoperative utility ranged from 0.21 to 0.51 for lumbar radiculopathy and 0.55 to 0.59 for cervical radiculopathy. The postoperative utility values ranged from 0.58 to 0.87 for lumbar radiculopathy and 0.69 to 0.72 for cervical radiculopathy.
Recent studies reporting EQ-5D values for cervical and lumbar radiculopathy patients
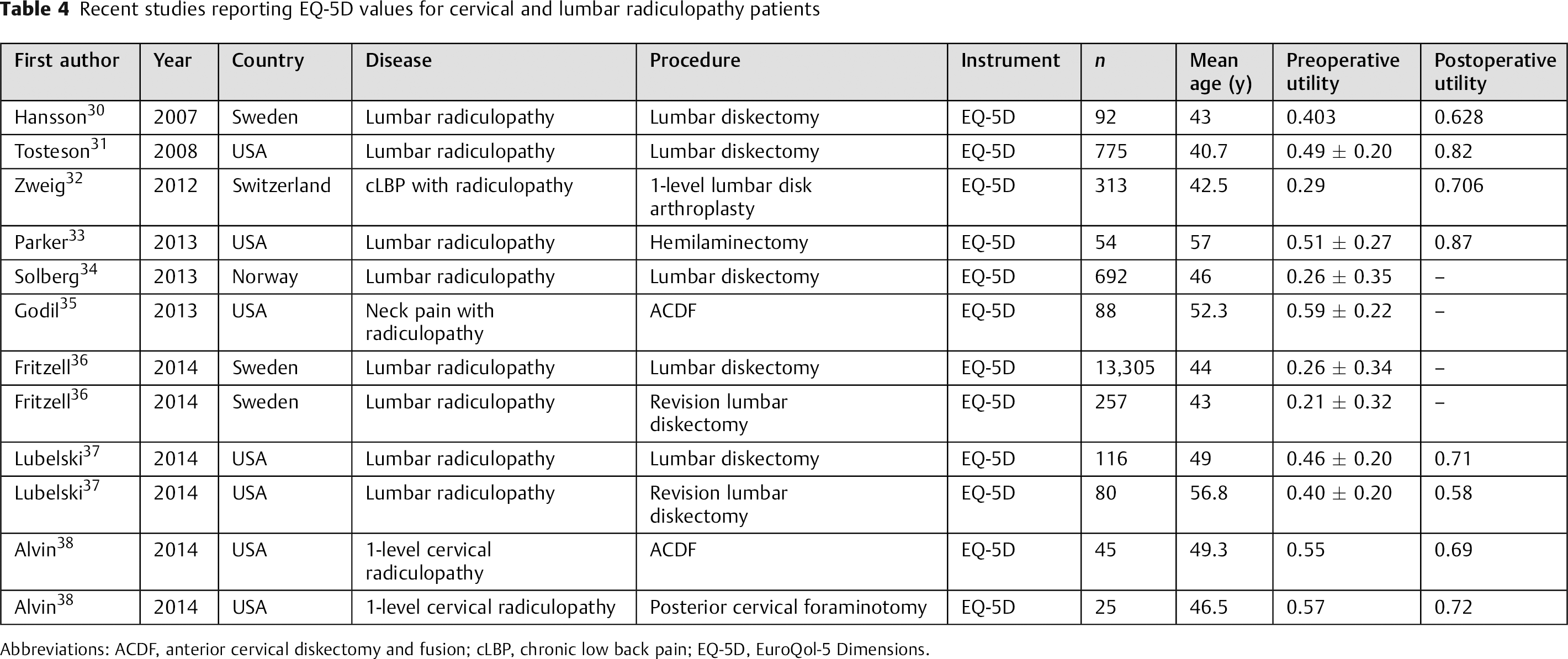
Abbreviations: ACDF, anterior cervical diskectomy and fusion; cLBP, chronic low back pain; EQ-5D, EuroQol-5 Dimensions.
For reference, the EQ-5D utility scores range from −0.594 to 1, depending on the population-specific value set used.
Discussion
The results of this study suggest that based on an SG survey of the general public, there are no significant differences in the utility values between the four most common levels of radiculopathy. Although functional disability varies by the affected nerve root, the contribution of pain may overshadow disability in terms of global HRQoL. On average, the participants were willing to undertake a 23% risk of death to be restored to perfect health from the described radiculopathy states. Additionally, age and sex did not play a role in how the participants valued each disease state. However, the utilities derived from our study were notably higher than those described in the literature based on the EQ-5D. Because of this finding, patients completing the EQ-5D have more potential for improvement than the theoretical maximum gain in utility of 0.23 among our study population. These differences would make the cost-utility ratios appear more favorable using the EQ-5D compared with our SG results.
There may be several reasons for the observed differences between our study and the literature. The most obvious source is that the patients in the literature experienced radiculopathy that warranted surgical intervention. Had we studied patients successfully treated with nonoperative measures, the results may have been different. Additionally, results from the SG method depend on the risk profile of the participants surveyed. If we assume that most individuals are risk averse, the utility scores will therefore be higher. The most commonly used EQ-5D value sets are based on TTO valuations, a method that does not present the participants with risk. Furthermore, the average age for our study population was ∼37 years old, considerably younger than the median ages of 44 and 49.3 for lumbar and cervical radiculopathies, respectively, for the EQ-5D. Health values have been linked to age, sex, and current health state, 18 and although radiculopathy affects patients of all ages, the younger age of our cohort suggests they may have less overall disease burden than those profiled in the literature.
King et al performed SG and TTO utility studies in patients with diagnosed cervical myelopathy and found that a better current health state was associated with assigning higher utility values for theoretical disease states. 19 If the same holds true to our sample population, we would expect our cohort to rate the theoretical health states higher than those who actually have the disease, which is in line with our findings. On the other hand, patients with poorer health status have been found to provide higher valuations of their own disease state, 20 as evidenced by patients on renal dialysis, 18 which would be contradictory to our findings. In this scenario, we would expect that the patients profiled in the literature, who actually underwent surgical intervention for radiculopathy, to have rated their disease states higher than they actually did. Nevertheless, we do not have detailed knowledge of the health states and comorbidities of our sample population or the patients in the literature, although those variables may have had an effect in one direction or another.
Another possible reason for the discrepancy is a fundamental difference between the valuation derived via indirect, generic assessment questions in the EQ-5D and the targeted scenarios presented in the SG, which focus directly on disease-specific pain and disability. Prior studies on spinal conditions such as cervical myelopathy and chronic low back pain have found that the utilities derived from primary SG and TTO surveys are higher than those obtained from the EQ-5D. 21 , 22 Carreon et al studied the relationship between the disease-specific disability instruments and the HRQoL instruments. In two studies of over 3,700 patients with degenerative cervical spine disorders and 14,500 patients with degenerative lumbar conditions undergoing surgical treatment, the authors could not accurately predict EQ-5D scores from Neck Disability Index, Oswestry Disability Index, or VAS scores. 23 , 24 For unclear reasons, however, when the same group performed similar studies using the SF-6D, they were able to develop models with a reasonable degree of accuracy. 25 , 26
Within the published spine literature, reporting HRQoL using the SF-36 is actually more common than with the EQ-5D, although most studies utilizing the SF-36 report individual domain subscores or component summary scores, which are not directly comparable to utility scores. However, the SF-36 can be mapped to the preference-based SF-6D to derive utility scores. We could only identify a single study with radiculopathy-specific SF-6D utility values. Mummaneni et al evaluated 148 patients undergoing lumbar diskectomy for radiculopathy who presented with a mean preoperative utility of 0.517. 27 We could not identify any studies providing SF-6D utility values specific to cervical radiculopathy. Two studies on cervical myelopathy and nonspecific cervical degenerative disk disease, which presumably would include many patients with coexisting radiculopathy, reported preoperative values of 0.575 and 0.55, respectively. 28 , 29
There are multiple limitations in the current study. The participants in our survey were all recruited from a single city in the Northeastern United States. Additionally, our sample population was younger and had a high average level of education than the patients with radiculopathy identified in the literature. There is also potential selection bias because of their recruitment from the campus of a university and its surrounding neighborhoods. Finally, detailed information on survey participants’ comorbidities had not been recorded, thus there is patient heterogeneity both among our study population and populations in the literature. These factors may limit the comparability of the two populations and the generalizability of the results.
Despite the limitations, the results of this study are nevertheless important because they demonstrate that from a societal perspective, the utility values associated with the most common levels of cervical and lumbar radiculopathy do not significantly differ from each other. These findings provide validation for the current practice of grouping the utility values for radiculopathy by spinal segment rather than by specific root levels. Additionally, the discrepancy between the average utility values elicited from our study and those derived from the EQ-5D highlights the need to be mindful of the instruments used when assessing comparative and cost-effective studies from different sources. The variations due to the disparate instruments may result in vastly different comparative outcomes results. Understanding the sources of variation and developing methods to better compare the different instruments will be increasingly important as patient-reported outcomes play a growing role in clinical research and health policy.
Disclosures
Nikhil R. Nayak, none
James H. Stephen, none
Kalil G. Abdullah, none
Sherman C. Stein, none
Neil R. Malhotra, none