
Abstract
Design
Retrospective study.
Objectives
(1) To investigate the quality-of-life (QOL) outcomes in the population undergoing lumbar spine surgery with versus without recombinant human bone morphogenetic protein-2 (rhBMP-2); (2) to determine QOL outcomes for those patients who experience postoperative complications; and (3) to identify the effect of patient characteristics on postoperative QOL outcomes.
Methods
A retrospective review of QOL questionnaires, including the Patient Health Questionnaire-9, Patient Disability Questionnaire (PDQ), EuroQol-5D (EQ-5D), and quality of life-year (QALY), was performed for all patients who underwent thoracolumbar and lumbar fusion surgery with versus without rhBMP-2 between March 2008 and September 2010. Individual preoperative and postoperative QOL data were compared for each patient. Demographic factors and complications were reviewed.
Results
We identified 266 patients, including 60 with and 206 without rhBMP-2. Questionnaires were completed an average of 10.3 ± 5 months after surgery. For all measures, average scores improved postoperatively compared with preoperatively. No differences in postoperative QOL outcomes were identified between the rhBMP-2 and the control cohorts. Median annual household income was positively associated with EQ-5D and QALY. Compared with those without, patients with postoperative complications had fewer QOL improvements.
Conclusions
There was no difference in QOL outcomes in the rhBMP-2 compared with the control group. Socioeconomic status and postoperative complications affected QOL outcomes following surgery. The QOL questionnaires provide the clinician with information regarding the patients’ self-perceived well-being and can be helpful in the selection of surgical candidates and for understanding the effectiveness of a given surgical procedure.
Keywords
Introduction
In recent years, there has been a rapid rise in the use of recombinant human bone morphogenetic protein-2 (rhBMP-2; InFUSE Bone Graft, Medtronic SofamorDanek, Memphis, Tennessee, United States) for spine fusions. 1 , 2 , 3 Epidemiologic studies have shown a continued pervasive use of rhBMP-2 despite conflicting studies regarding its risks and benefits. 4 , 5 , 6 , 7 , 8 Recently, increasing numbers of complications have been reported, and there has been a decline in rhBMP-2 sales. Most of the aforementioned studies identify the complications associated with the use of rhBMP-2, with far less focus on the overall quality of life (QOL) and patient satisfaction following surgery. QOL measures and predisposing factors have been investigated for the surgical and nonsurgical treatment of patients with lower back pain, 9 , 10 , 11 lumbar diskectomy, 12 transforaminal lumbar interbody fusion, 13 as well as fusion for adjacent segment disease. 14 Despite the increasingly widespread use of rhBMP-2, however, such an analysis has not been performed in the population receiving rhBMP-2 in spine fusion.
The present study utilizes prospectively collected QOL outcomes measures (Patient Health Questionnaire-9 [PHQ-9]; Pain Disability Questionnaire [PDQ]; and EuroQol 5D [EQ-5D], and quality of adjusted life-year [QALY]) in patients who underwent thoracolumbar or lumbar fusion with rhBMP-2 to determine the preoperative to postoperative changes in QOL.
The biologic rhBMP-2 has become widely used in fusion surgery for perceived enhancement of fusion rates, but there is a relative absence of information on QOL outcomes in these patients. Most studies have focused on clinical or radiographic end points (e.g., operative time, blood loss, complications, fusion rates) and have not sufficiently utilized validated QOL data, which more accurately represent subjective patient outcomes.
The present study has three main objectives. First, pre- and postoperative QOL and QALY scores are compared between patients who received rhBMP-2 versus those who did not to ascertain the relative contribution of rhBMP-2 to postoperative QOL. Second, we investigate the impact of postoperative complications on QOL following surgery. Third, we identify demographic factors that are associated with poor postoperative QOL outcomes to help identify the optimal candidates for rhBMP-2 fusion enhancement. Our hypothesis was that the use of rhBMP-2 would not improve QOL outcome scores.
Methods
Database
A retrospective review of prospectively acquired data was performed for all patients who underwent thoracolumbar or lumbar fusion surgery with versus without rhBMP-2 at a single tertiary care center between March 2008 and September 2010. The electronic medical record system was queried to identify patients who fit the inclusion and exclusion criteria. Patients were included if they underwent thoracolumbar or lumbar spine fusion surgery with or without rhBMP-2 for degenerative conditions. Only those patients who had completed both preoperative and postoperative QOL assessments and had more than 6 months’ follow-up were included in the present study. Patients were excluded if they were younger than 18 years or had previous lumbar spine surgery, tumor, trauma, infection, or neurodegenerative disease (e.g., multiple sclerosis) as primary etiology. Relevant patient information and other study data were securely collected and managed using REDCap (Research Electronic Data Capture). 15 We intentionally excluded revision surgery to avoid potential confounding. Prospectively collected QOL outcomes were available, through the institutional Knowledge Program, via which all presenting patients (beginning in March 2008) are asked to complete the relevant self-assessments prior to being seen by their health care providers.
Patient Population
Patients had varying indications for surgery, including spondylolisthesis, degenerative disk disease stenosis, and spondylosis with pathologic motion, kyphosis, or scoliosis. All patients in the rhBMP-2 cohort received small or large doses of rhBMP-2 (4.2 mg or 12 mg, InFUSE).
Patient demographics were recorded, including age, gender, marital status, body mass index, smoking status (past and present), medications (antidepressants, anxiolytics, narcotic analgesics), and chronic conditions (psychological disorders, hypertension, hyperlipidemia, coronary heart disease, diabetes). Current smokers were defined as patients who were smoking at the time of surgery. Median annual household incomes were calculated based on patients’ zip codes. 16 , 17 , 18 Operative information included surgical approach, duration of hospital stay, and blood loss. Information on postoperative complications, including radiculitis, wound infection, pseudarthrosis, and urologic and bowel problems, was also collected.
Surgical approaches and the reasons for surgeon use of rhBMP-2 were heterogeneous, with no definable protocol or limitations for its use. Levels operated upon included T11 to S1. Seven fellowship-trained spine surgeons (three neurosurgeons, four orthopedic surgeons) performed all operations (with equal distributions of the surgical approaches and levels).
QOL data were collected in conjunction with the institutional Knowledge Project. All patients were given a portable tablet personal computer prior to being seen by the health care provider (both pre- and postoperatively) and asked to complete the PHQ-9, PDQ, and EQ-5D questionnaires. The responses to these questions were then automatically transferred to their medical record. As with most practices, some patients were unable, or refused, to complete the questionnaires. These patients were excluded from this study.
These clinical outcomes and QOL measures have been previously used in spine surgery research and have advantages over some other outcome measures such as the Short Form-36, 19 , 20 , 21 , 22 , 23 Oswestry Disability Index, 23 , 24 , 25 , 26 visual analog scale, Million Visual Analog Scale, 27 , 28 , 29 , 30 and Roland-Morris Disability Questionnaire. 23 , 31 , 32
Although the previously mentioned QOL measures determine level of disability and functionality, they are not very effective at ascertaining pre- and postoperative psychological dispositions (e.g., depression and anxiety). Moreover, as lack of postoperative improvement in pain and function has been shown to be predicted by preoperative depression and anxiety (regardless of the surgical outcome), 12 , 33 , 34 , 35 psychological predisposition should be an important consideration in determining candidates for surgery. The PHQ-9 36 is a validated questionnaire that can be used to assess for presence and severity of depression in the spine surgery population. 12 , 33 , 37 , 38 , 39 Finally, the EQ-5D provides analysis of multiple aspects of the patients’ QOL. It has been validated in different populations for various disease processes (allowing for comparisons) and is increasingly used in spine surgery research. 40 , 41 , 42 , 43 , 44 EQ-5D is broken down into five components including EQ-Mobility, EQ-Self-Care, EQ-Usual Activities, EQ-Pain/Disability, and EQ-Anxiety/Depression.
QALY was derived from the EQ-5D and is defined as the number of years of life that would be added by the intervention. This value is calculated as QALY = (Years of Life) · (Utility Value), where 1 year in perfect health is assigned the utility value of 1.0 and death is assigned a utility value of 0.0; anything between perfect health and death is assigned a utility value between 0.0 and 1.0. This utility value is calculated based on the EQ-5D scores and converted to QALY values using U.S. valuation. 40 , 45 , 46 , 47
The QOL data that were obtained were compared with the minimal clinically important differences (MCIDs) for these particular surgeries. The MCID values are patient-derived health outcome scores for different QOL measures that reflect the minimum change in QOL necessary to elicit meaningful improvement for the patient. Several different methods exist in calculating MCIDs because multiple factors influence the MCID. The MCIDs used for each questionnaire was as follows: visual analog scale (2.1), PDQ (26.0), PHQ-9 (5.0), and EQ-5D QALY (0.1 to 0.2). 13 ,48,49
Statistical Analysis
All data were analyzed using JMP 9.0 (2007; SAS Institute Inc., Cary, North Carolina, United States). An a priori power analysis, with an α level of 0.05 and power of 0.8, was performed to ensure sufficient sample size in each group. Due to the observed ranges of the QOL measures, PDQ and PHQ were analyzed as continuous variables and the individual EQ-5D questions were analyzed as categorical variables. Descriptive statistics summarizing patient demographics were presented as means and standard deviations or counts with percentages as appropriate. Paired t tests and Wilcoxon signed rank tests were used for parametric and nonparametric data, respectively, to ascertain significance in the pre- to postoperative QOL score change for each patient for the respective questionnaire. Association of demographic/operative factors with changes in pre- to postoperative QOL measures was calculated using independent sample t tests, analysis of variance, or chi-square tests, as appropriate, and p values ≤ 0.05 were considered statistically significant.
Results
Demographics and Hospital Experience
In all, 743 patients underwent thoracolumbar or lumbar fusion between 2008 and 2010 and at least partially completed the QOL questionnaires. Of these patients, 266 (36%) fit the inclusion criteria with both pre- and postoperative QOL data and a minimum 6-month follow-up. This included 60 (31 men, 52%) who underwent thoracolumbar or lumbar fusion with rhBMP-2 and 206 (99 men, 48%) who underwent fusion without rhBMP-2 (Table 1). The mean age in the rhBMP-2 group was 57 and in the control group was 60. Average body mass index was 29 for both the rhBMP-2 and control groups. Marital status was similar in both cohorts, with the majority of patients were married (73% in the rhBMP-2 group and 71% in the control group). Antidepressant use was 35% in the rhBMP-2 group and 28% in the control group (p = 0.3), anxiolytic use was 32% in the rhBMP-2 and 25% in the control group (p = 0.3), and narcotic use was 48% and 70% for the rhBMP-2 and control groups, respectively (p = 0.002), at the time of surgery. Past smoking history was similar in both groups (50% and 45% for the rhBMP-2 and control groups, respectively), but there were more current smokers in the rhBMP-2 group (52%, 31 of 60) as compared with the control group (1%, 2 of 206; p = 0.02). Presumably, surgeons were more likely to use the biologic for patients who were active smokers.
Patient characteristics
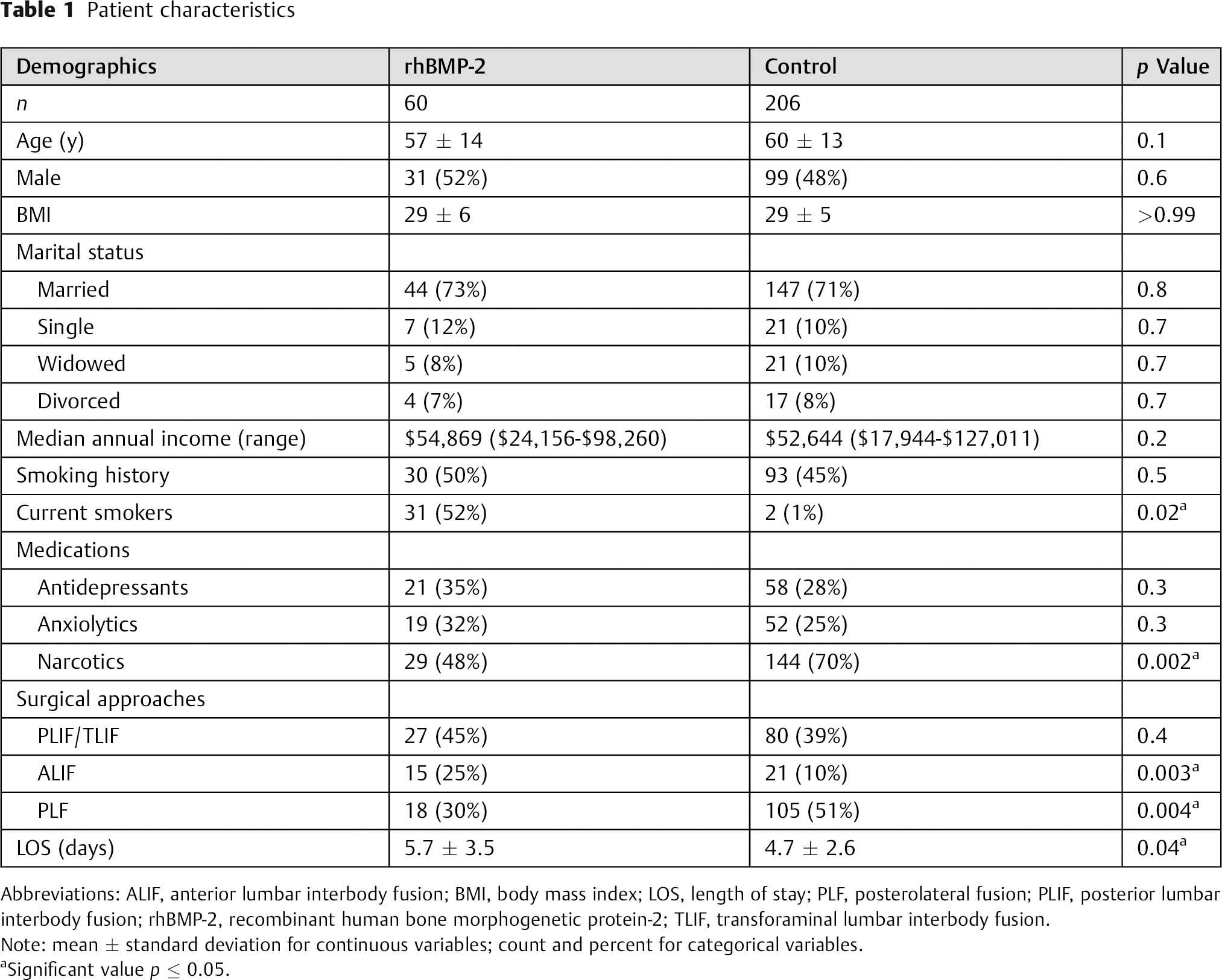
Abbreviations: ALIF, anterior lumbar interbody fusion; BMI, body mass index; LOS, length of stay; PLF, posterolateral fusion; PLIF, posterior lumbar interbody fusion; rhBMP-2, recombinant human bone morphogenetic protein-2; TLIF, transforaminal lumbar interbody fusion.
Note: mean ± standard deviation for continuous variables; count and percent for categorical variables.
Significant value p ≤ 0.05.
For the surgical indications of the rhBMP-2 group, 63% had stenosis, 35% had spondylolisthesis, 23% had degenerative disk disease, and 20% had scoliosis. For the control group, 55% had stenosis, 33% had spondylolisthesis, 12% had degenerative disk disease, and 9% had scoliosis. Many of the diagnoses had stenosis listed as the primary diagnosis for surgery; however, fusion was performed because of either a causative or concomitant instability or deformity or in some cases for recurrent same-level stenosis. Listed diagnoses were not mutually exclusive. Decision to operate on the patient and surgical approach were at the discretion of the primary surgeon at our institution, all of whom are fellowship trained. Surgical approaches included posterior lumbar interbody fusion/transforaminal lumbar interbody fusion (45% in the rhBMP-2 group and 39% in the control group, p = 0.4), anterior lumbar interbody fusion (25% in the rhBMP-2 group and 10% in the control group, p = 0.003), and posterolateral fusion (30% in the rhBMP-2 group and 51% in the control group, p = 0.004). The rates of the different surgical approaches may vary between our institution and others, but these approaches represent the independent preferences of surgeons at our institution. Average hospital length of stay was 5.7 days in the rhBMP-2 group and 4.7 days in the control group (p = 0.04).
Quality-of-Life Outcomes Measures
All patients in the study completed both the preoperative and postoperative QOL questionnaires for the PHQ-9, PDQ, and EQ-5D. For all measures, there was a statistically significant reduction (improvement in QOL) of the average score postoperatively compared with preoperatively (Table 2). Preoperative QOL questionnaires were completed an average of 1.6 ± 1.5 months (48 ± 47 days) before the operation and were postoperatively completed an average of 10.3 ± 5 months (315 ± 151 days) after the surgery; all patients completed the questionnaire at least 6 months postoperatively. Although there was a high standard deviation of dates, plotting the pre- to postoperative differences in the QOL scores versus the length of time between surgery and postoperative evaluation indicated that the timing of QOL questionnaire completion did not affect the change in scores.
Quality of life outcomes
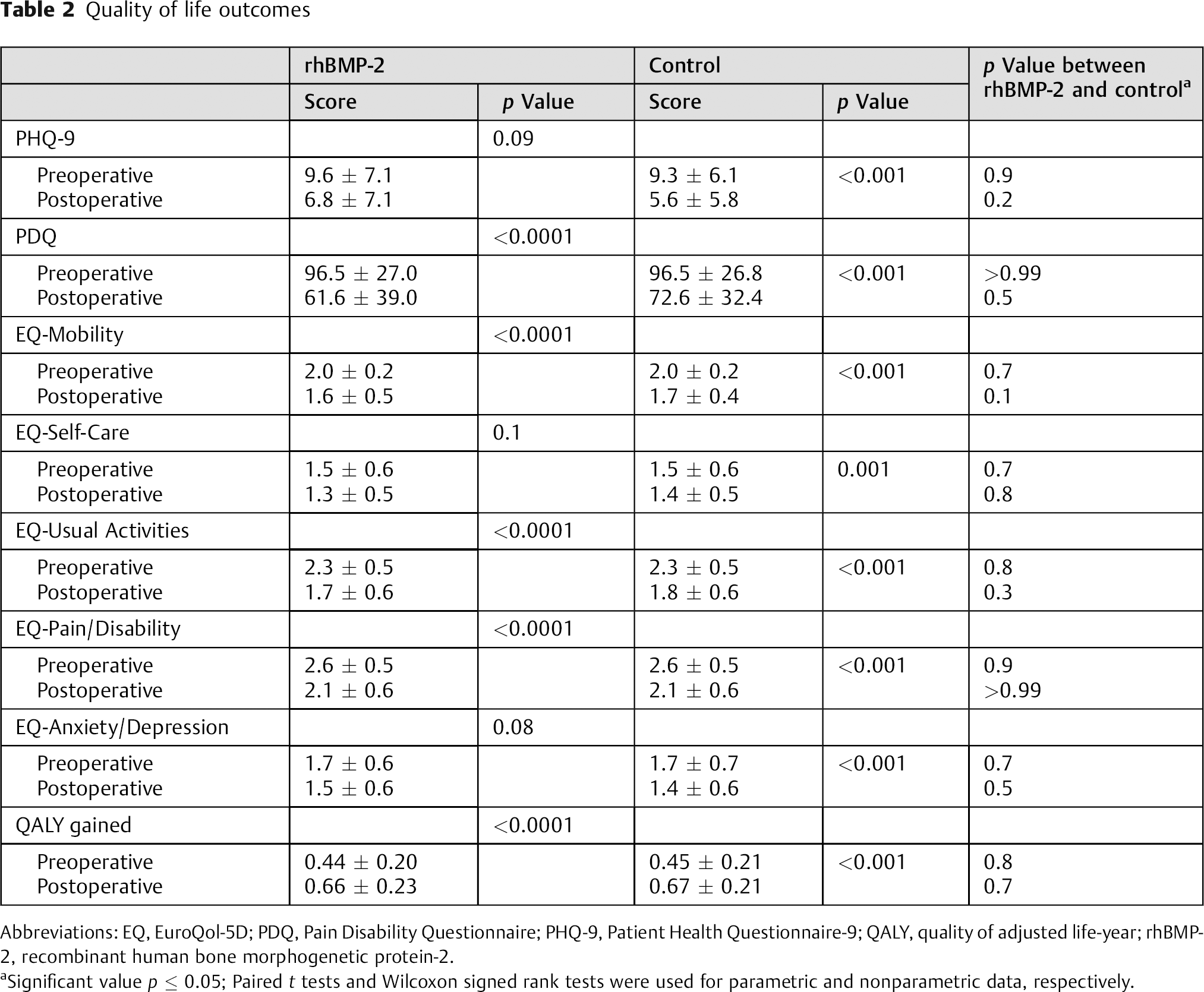
Abbreviations: EQ, EuroQol-5D; PDQ, Pain Disability Questionnaire; PHQ-9, Patient Health Questionnaire-9; QALY, quality of adjusted life-year; rhBMP-2, recombinant human bone morphogenetic protein-2.
Significant value p ≤ 0.05; Paired t tests and Wilcoxon signed rank tests were used for parametric and nonparametric data, respectively.
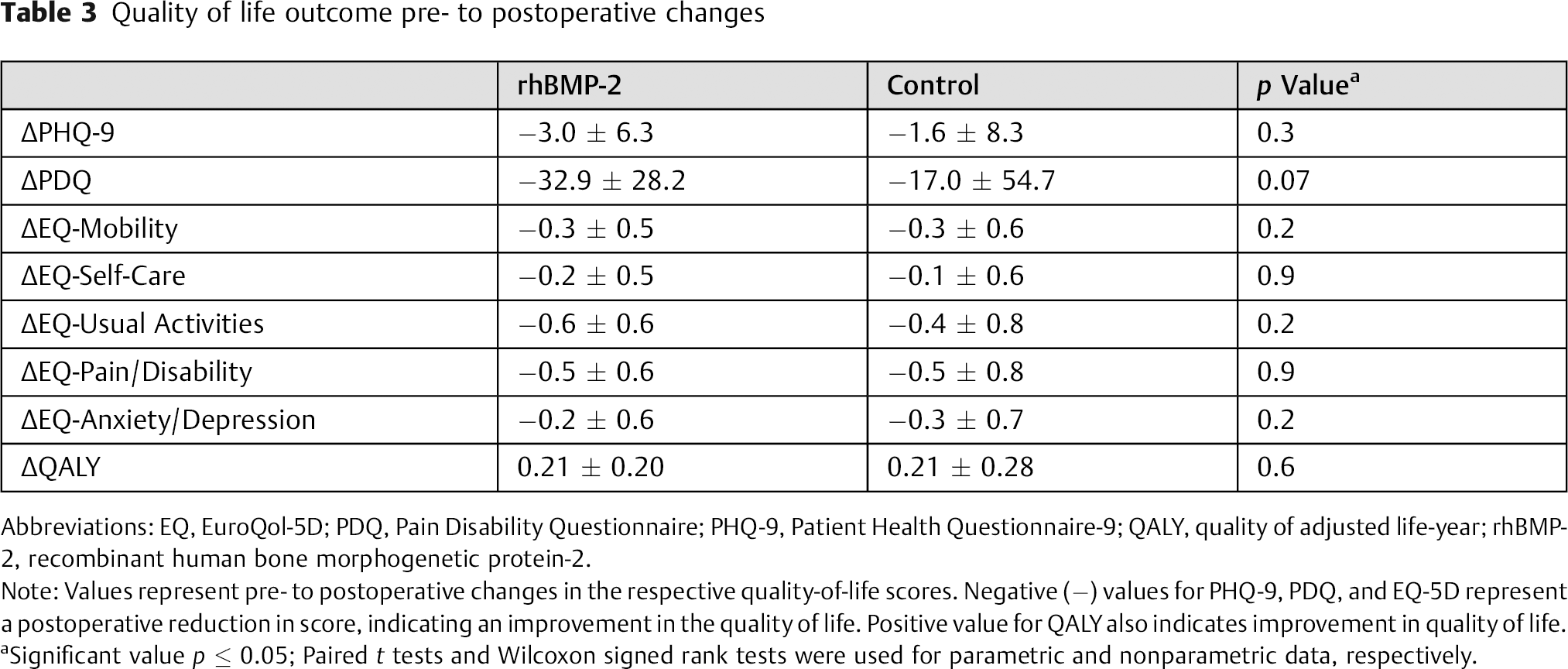
In the rhBMP-2 cohort, PHQ-9 scores were found to be reduced (improved QOL) from an average of 9.6 ± 7.1 preoperatively to 6.8 ± 7.1 postoperatively (p = 0.0006), and PDQ was reduced from an average of 96.5 ± 27.0 to 61.6 ± 39.0 (p < 0.0001). Similarly, in the control cohort, PHQ-9 scores were found to be reduced (improved QOL) from an average of 9.3 ± 6.1 preoperatively to 5.6 ± 5.8 postoperatively (p < 0.0001), and PDQ was reduced from an average of 96.5 ± 26.8 to 72.6 ± 32.4 (p < 0.0001). There was also an improvement in QALY from pre- to postoperative for both the rhBMP-2 group (0.44 ± 0.20 preoperatively to 0.66 ± 0.23 postoperatively, p < 0.0001) and the control group (0.45 ± 0.21 preoperatively to 0.67 ± 0.21 postoperatively, p < 0.0001). No significant differences were found for any of the individual measures or the pre- to postoperative changes between the rhBMP-2 and the control groups (Table 3).
Quality of life outcome pre- to postoperative changes
Abbreviations: EQ, EuroQol-5D; PDQ, Pain Disability Questionnaire; PHQ-9, Patient Health Questionnaire-9; QALY, quality of adjusted life-year; rhBMP-2, recombinant human bone morphogenetic protein-2.
Note: Values represent pre- to postoperative changes in the respective quality-of-life scores. Negative (−) values for PHQ-9, PDQ, and EQ-5D represent a postoperative reduction in score, indicating an improvement in the quality of life. Positive value for QALY also indicates improvement in quality of life.
Significant value p ≤ 0.05; paired t tests and Wilcoxon signed rank tests were used for parametric and nonparametric data, respectively.
The individual questions of the EQ-5D for both the rhBMP-2 and control groups, which are scored from 1 to 3, all showed statistically significant reduction in score (improvement in symptoms), except for EQ-Self-Care and EQ-Anxiety/Depression in the rhBMP-2 cohort, which remained relatively similar pre- to postoperatively. The specific scores and changes in score can be seen in Table 2.
Patient demographic factors in both groups were associated with postoperative change in QOL. Particularly, greater annual income (median: $52,644; range: $17,944 to $127,011) was significantly associated (or trended toward significance) with superior improvements in EQ-Mobility (p = 0.02), EQ-Self-Care (p = 0.003), EQ-Usual Activities (p = 0.047), EQ-Pain/Disability (p = 0.2), EQ-Anxiety/Depression (p = 0.1), QALY gained (p = 0.01), PHQ-9 (p = 0.07), and PDQ (p = 0.07). Additionally, changes in the PDQ scores were significantly associated with patient characteristics in the rhBMP-2 group. Patients not taking narcotic analgesics at the time of surgery tended to decrease (improve) their PDQ scores after surgery more frequently than those taking narcotic analgesics (97% versus 79%, respectively, p = 0.049). Additionally, the average improvement in PDQ score among those taking narcotics at time of surgery was 23 points, whereas those not taking narcotics had an average improvement of 46 points (p = 0.003). This association between QOL changes and narcotic use was not seen with the control patients.
Trends were also seen between QOL and postoperative complications in both groups (Table 4). Eight patients with complications (13%, 8/60) were identified in the rhBMP-2 cohort, which included 2 cases of urologic complications, 5 cases of new-onset radiculitis, 1 case of wound infection, and 3 cases of pseudarthrosis. Although both patients with and patients without complications tended to show improvement in QOL following surgery, those without complications in both groups improved to a greater extent. In the rhBMP-2 group, patients without complications had a significantly greater improvement in EQ-Pain/Disability as compared with those with complications (−0.6 versus −0.1, p = 0.046), as well as a trend toward significantly greater improvement in QALY (0.23 versus 0.09, p = 0.07). Of those in the control group, 8 patients (4%, 8/206) had complications, including 1 with urologic complication, 4 with new-onset radiculitis, 1 with a myocardial infarction, 1 with deep vein thrombosis, and 1 with a pseudomeningocele. Patients in the control cohort without complications had a trend toward significantly greater improvement in EQ-Usual Activities as compared with those with a complication (−0.5 versus 0.0, p = 0.07). Moreover, although not reaching statistical significance (p = 0.2), there was a clinically significant (>MCID of 0.1 QALY gained) difference in postoperative QALY gained between those without a complication (0.23 QALY gained) and those with a complication (0.12 QALY gained).
Association of quality-of-life outcomes with complications
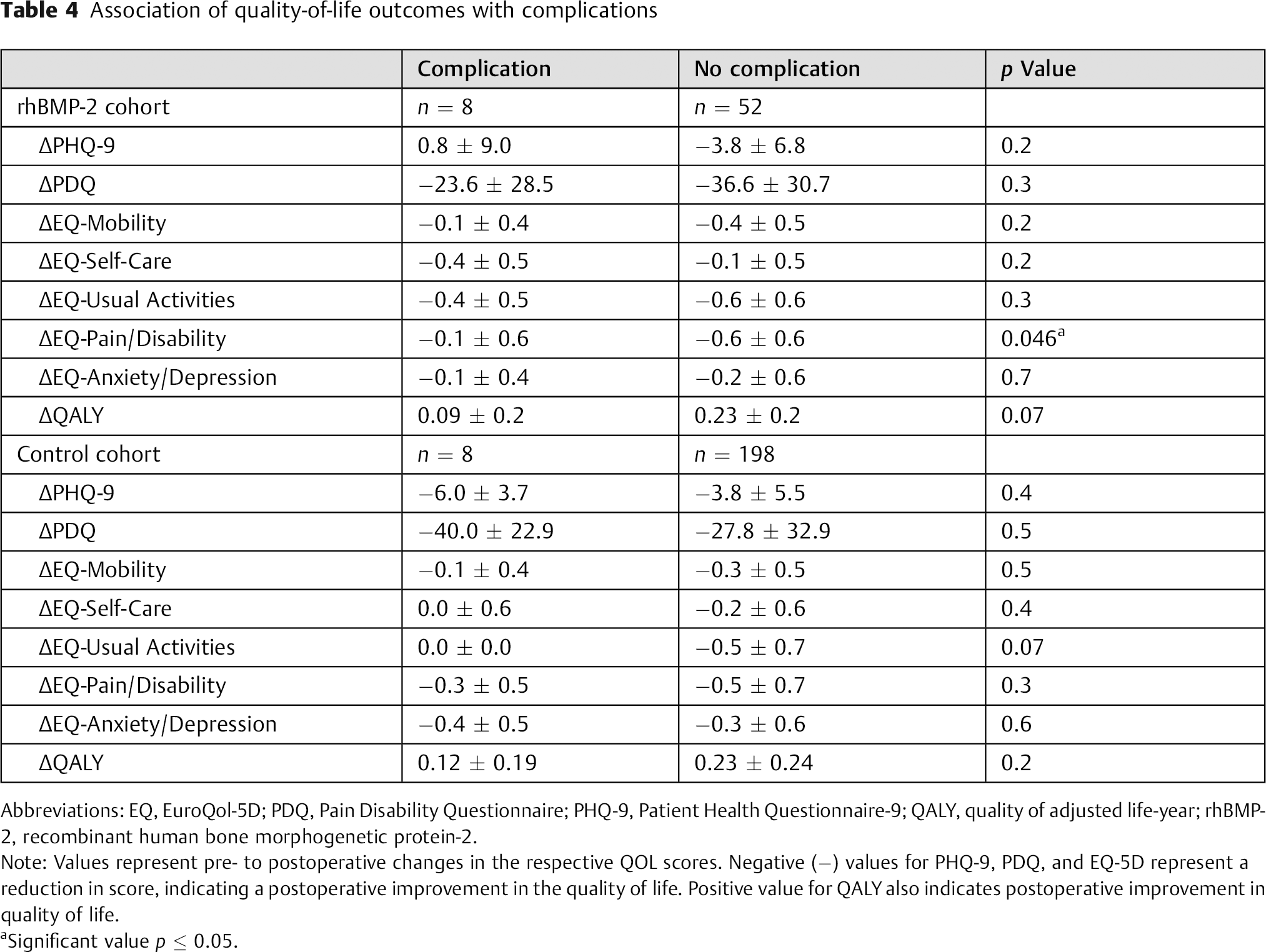
Abbreviations: EQ, EuroQol-5D; PDQ, Pain Disability Questionnaire; PHQ-9, Patient Health Questionnaire-9; QALY, quality of adjusted life-year; rhBMP-2, recombinant human bone morphogenetic protein-2.
Note: Values represent pre- to postoperative changes in the respective QOL scores. Negative (−) values for PHQ-9, PDQ, and EQ-5D represent a reduction in score, indicating a postoperative improvement in the quality of life. Positive value for QALY also indicates postoperative improvement in quality of life.
Significant value p ≤ 0.05.
To account for potentially confounding variables, additional analysis was performed controlling for smoking status and surgical approach. Despite differences between the cohorts in the rates of these factors, no significant differences were found in the QOL outcomes between current and noncurrent smokers or between the various surgical approaches.
Discussion
The majority of rhBMP-2 is used in an off-label fashion in the United States. With the rise in use of rhBMP-2, 3 the ambiguity regarding the associated complications, the complication rates, 1 , 6 , 7 , 50 the natural history of adverse events, and the uncertainty associated with the appropriate selection of patients for rhBMP-2 use has escalated. Moreover, the high cost of rhBMP-2 suggests that it be reserved for those patients who would derive maximum benefit. To this end, analysis can be performed using the traditional objective hospital outcomes such as complication rates, duration of hospital stay, and time to return to work. The medical and surgical community, however, has seen a fundamental change in how outcomes are measured and reported. The employment of validated measures of patient function and QOL are now commonplace.
In the present study, we sought to investigate three aspects of postoperative QOL outcomes in patients receiving rhBMP-2. First, we compared the pre- and postoperative QOL scores between patients who received rhBMP-2 and those who did not. Second, we identified demographic factors associated with QOL outcomes in this population. Third, we evaluated the QOL implications associated with postoperative complications.
Patients in both the rhBMP-2 and control cohorts demonstrated improvement in their QOL after surgery in terms of their pain and disability (PDQ), mental health (PHQ-9), and general function and well-being (EQ-5D). Although all of these differences were statistically significant, only the EQ-5D (QALY) met the MCID of 0.1 to 0.2 for both groups, and the PDQ for the rhBMP-2 cohort met the MCID of 26, thereby demonstrating a clinically meaningful improvement for patients. The pre- to postoperative differences in the PHQ-9 for both groups and the PDQ for the control group were below the MCID threshold for their respective questionnaires. Whereas no statistically significant differences between the two groups were found in the QOL outcomes following surgery, there was a trend toward significance (p = 0.07) for the postoperative change in PDQ, with a greater improvement in the rhBMP-2 cohort. In contrast, the changes in EQ-5D (QALY) scores met the MCID threshold but were not statistically different between groups. This supports our hypothesis that rhBMP-2 does not offer any comparative advantage, or disadvantage, in terms of postoperative QALY. Therefore, given these results, it is important to further define the utility of rhBMP-2 with longer-term studies, the associated economic cost, and its unique adverse event profile.
We also found that certain patient characteristics were associated with improvement or worsening of the patients’ QOL, particularly in those patients receiving rhBMP-2. The changes in the PDQ indicate that those patients who were taking narcotic medications preoperatively were less likely to report improvement in their pain and disability. This association of narcotic use with poorer outcomes after spine surgery has been previously demonstrated by Lawrence and colleagues. 51 In a retrospective review of 91 consecutive patients who underwent cervical fusion, the authors found that those patients who had used daily narcotics prior to surgery had worse outcomes compared with the control group, which did not use narcotics. This association between narcotic use and poor postoperative (or postintervention) outcomes has also been shown to occur in various other musculoskeletal pathologies. 52 , 53
Previous studies have identified age and gender, 40 , 54 as well as psychological comorbidities such as depression, 12 , 35 , 55 , 56 to affect outcomes following spine surgery. In the present study, such effect was not observed. We did, however, identify significant associations between greater median annual household income and superior postoperative QOL outcomes including EQ-Mobility, EQ-Self-Care, EQ-Usual Activities, QALY gained, and trends toward significant associations with PHQ-9 and PDQ. This effect has been previously shown in both spine surgery outcomes 57 , 58 and in QOL outcomes among cancer survivors. 59
Significant associations were also found between postoperative complications and the EQ-5D and QALY outcomes for both the rhBMP-2 and control cohorts. There were relatively few patients with postoperative complications in each cohort, and therefore the statistical power to identify significant associations was limited. Furthermore, postoperative follow-up was an average of only 10 months, and so it is possible that certain complications, such as clinically relevant pseudarthrosis, may not have yet been detected. Accordingly, although there were some statistically significant associations between having a postoperative complication and a worse QOL outcome, more significant associations may have been seen if there was a larger cohort of patients with complications. The use of these QOL instruments complement the more traditional measures of success of surgery, such as identification of complications, and likely allow for more accurate and tailored responsiveness by the health care team to the patient's needs and concerns.
The present study had several limitations that must be taken into consideration when reviewing the data. Complications and patient demographic data were collected retrospectively and included records from multiple surgeons and multiple surgical indications. This leads to heterogeneity in the data but also improves the generalizability. These results were also relatively short term, and only about a third of the patients at our institution met our inclusion criteria. Longer follow-up and prospectively designed studies are necessary to assess the durability and reliability of our results. This cannot be overstated. There were also differences between the cohorts, in the form of a selection bias, that introduce the potential of confounding results, which we attempted to account for with our statistical analyses. To our knowledge, however, this is the first study to review QOL outcome data for patients receiving rhBMP-2 during surgery versus those without rhBMP-2. Moreover, the present study includes a large number of patients and a unique combination of validated QOL questionnaires, providing comprehensive psychosocial and QOL outcome information about this spine surgery patient population. Although there are limitations associated with the present retrospective analysis, the preliminary results will hopefully spur future larger prospective studies to validate these findings.
Conclusion
The present study demonstrated that the rhBMP-2 patient population tends to show improvement in QOL following surgery. Most of the measures demonstrate improvement without any differences based on whether rhBMP-2 was used or not, with PDQ possibly improving to a greater extent among patients receiving rhBMP-2. We identified that narcotic medication use at the time of surgery, as well as lower annual household income, is associated with poorer QOL outcomes postoperatively. Furthermore, trends toward significance were identified between those with postoperative complications and worse improvements in QOL outcomes.
Validated outcomes instruments that measure various dimensions of patients’ QOL are available to assess the success of spine surgery. In the patient population undergoing lumbar surgery with rhBMP-2, the PHQ-9, PDQ, and EQ-5D questionnaires provide the clinician with information regarding the patient's function and well-being.
The results obtained could enable the spine surgery community to better understand the postoperative QOL outcomes associated with various psychosocial and socioeconomic factors. A better understanding of these factors will lead to improved patient selection, more appropriate treatment decisions, and superior outcomes following surgery. Ultimately, well-designed prospective studies with long-term follow combined with cost-effective analysis are needed to fully elucidate these associations and understand the real QOL benefits of including rhBMP-2 in spine fusion.
Disclosures
Daniel Lubelski, none
Matthew D. Alvin, none
Andrew Torre-Healy, none
Kalil G. Abdullah, none
Amy S. Nowacki, none
Robert G. Whitmore, none
Michael P. Steinmetz, none
Edward C. Benzel, none
Thomas E. Mroz, none
Footnotes
Note
No grants, technical, or corporate support were received in conducting this study or writing this manuscript. No relevant conflicts of interest. Institutional Review Board approval (Study #10–886) was obtained prior to start of study.