
Abstract
Study Design
Surgeon survey.
Objective
To analyze multimodal intraoperative monitoring (MIOM) for different combinations of methods based on the collected data and determine the best combination.
Methods
A questionnaire was sent to 72 training institutions to analyze and compile data about monitoring that had been conducted during the preceding 5 years to obtain data on the following: (1) types of monitoring; (2) names and number of diseases; (3) conditions of anesthesia; (4) condition of stimulation, the monitored muscle and its number; (5) complications; and (6) preoperative and postoperative manual muscle testing, presence of dysesthesia, and the duration of postoperative motor deficit. Sensitivity and specificity, false-positive rates, and false-negative rates were examined for each type of monitoring, along with the relationship between each type of monitoring and the period of postoperative motor deficit.
Results
Comparison of the various combinations showed transcranial electrical stimulation motor evoked potential (TcMEP) + cord evoked potential after stimulation to the brain (Br-SCEP) combination had the highest sensitivity (90%). The TcMEP + somatosensory evoked potential (SSEP) and TcMEP + spinal cord evoked potential after stimulation to the spinal cord (Sp-SCEP) combinations each had a sensitivity of 80%, exhibiting little difference between their sensitivity and that obtained when TcMEP alone was used. Meanwhile, the sensitivity was as low as 50% with Br-SCEP + Sp-SCEP (i.e., the cases where TcMEP was not included).
Conclusions
The best multimodality combination for intraoperative spinal cord monitoring is TcMEP + Br-SCEP, which had the highest sensitivity (90%), the lowest false-positive rate (6.1%), and the lowest false-negative rate (0.2%).
Introduction
Somatosensory evoked potential (SSEP) has been used to monitor spinal surgery since the 1980s, 1 , 2 , 3 , 4 , 5 and cord evoked potential after stimulation to the brain (Br-SCEP, D-wave) has also been used for motor pathway monitoring since the 1990s. 6 , 7 , 8 , 9 , 10 , 11 Other monitoring techniques followed, including free-running electromyography, 12 , 13 spinal cord evoked potential after stimulation to the spinal cord (Sp-SCEP), spinal cord evoked potential after stimulation to the peripheral nerve (Pn-SCEP), and transcranial electrical stimulation motor evoked potential (TcMEP). 14 , 15 , 16 , 17 , 18 In particular, TcMEP is regarded as the most sensitive monitoring. 10 Although it has been reported that TcMEP shows accurate real-time invasiveness of surgery with nearly 100% sensitivity and specificity, there are occasional reports that TcMEP, being highly sensitive, produces a relative high frequency of false-positives, thus hindering the surgery. 19 , 20 , 21 Accordingly, the importance of multimodality monitoring rather than single-modality approaches has been pointed out in numerous reports. Upon studying 1,017 cases of multimodal intraoperative monitoring (MIOM), Sutter et al reported the usefulness of MIOM, citing 89% of sensitivity and 99% of specificity, 22 and Sala et al reported the usefulness of the combination of TcMEP and D-wave for intramedullary spinal cord tumor. 9 Previous reports, however, used different modality combinations for MIOM. Furthermore, in no previous reports has any comparison been made among different combinations in terms of sensitivity or specificity. We at the Monitoring Committee of the Japanese Society for Spine Surgery and Related Research conducted a nationwide multicenter study in 2007 and collected data from 7,158 cases of monitoring performed at numerous institutions during the preceding 5 years. 23 The objective of this study is to evaluate the usefulness of various combinations of monitoring techniques to detect motor deficits after surgery.
Materials and Methods
Subjects
From 2007 to 2010, the Monitoring Committee of the Japanese Society for Spine Surgery and Related Research conducted a nationwide multicenter study to determine the manner in which intraoperative spinal cord monitoring was conducted. A questionnaire was sent to 72 training institutions to analyze and compile data about cases of monitoring that had been conducted during the preceding 5 years. The questionnaire asked about: (1) the types of monitoring; (2) the names and number of disease; (3) the conditions of anesthesia; (4) the condition of stimulation, the monitored muscle and its number; (5) any complications; (6) the preoperative and postoperative manual muscle testing (MMT), presence of dysesthesia, the duration of postoperative motor deficit. The MMT is graded as follows: grade 0, no perceptible muscle contraction; grade 1, muscle contraction palpable, but no motion; grade 2, motion of the part only with gravity reduced; grade 3, the muscle can hold the part in the test position against gravity alone; grade 4, the patient can move the part through the full active range of motion against “some” resistance; grade 5, the patient can move the part through the full active range of motion against “full” resistance. MMT was performed at final follow-up (average 7.8 months) after surgery by a third party. 20 A total of 7,158 cases of monitoring were compiled. Appropriate Institutional Review Board approval was obtained.
Criteria for Selecting Cases
The prerequisites for inclusion in the baseline data were as follows: (1) cases in which monitoring was conducted under the stimulation condition shown in Table 1; (2) cases in which monitoring was conducted under the recording condition shown in Table 1; (3) cases recorded at institutions where loss of amplitude for TcMEP and amplitude loss of 50% or more or latency delay of 10% or more for Br-SCEP, Sp-SCEP, and SSEP were used as the alarm points. When any of the waveforms changed during the surgery, we ordered the anesthetist to raise the systolic blood pressure blood pressure or reverse hypotensive anesthesia and warm the core temperature. If the waveform still did not recover, such cases were considered positive as regards to the waveform change, and the surgeon was alerted to suspend the surgery. It was regarded as true-positive if postoperative paralysis was recognized, and it was regarded as false-positive if postoperative paralysis was not recognized. The anesthesia management that allows intraoperative monitoring particularly of TcMEP consists of a constant infusion of propofol (usually in a dose of ∼100 to 150 μg/kg/min) and fentanyl (usually around 1 μg/kg/h). Short-acting muscle relaxants are given during intubation but not thereafter to allow continuous TcMEP monitoring. 10 Halogenated anesthetics should not be used.
Monitoring condition of stimulation and recording
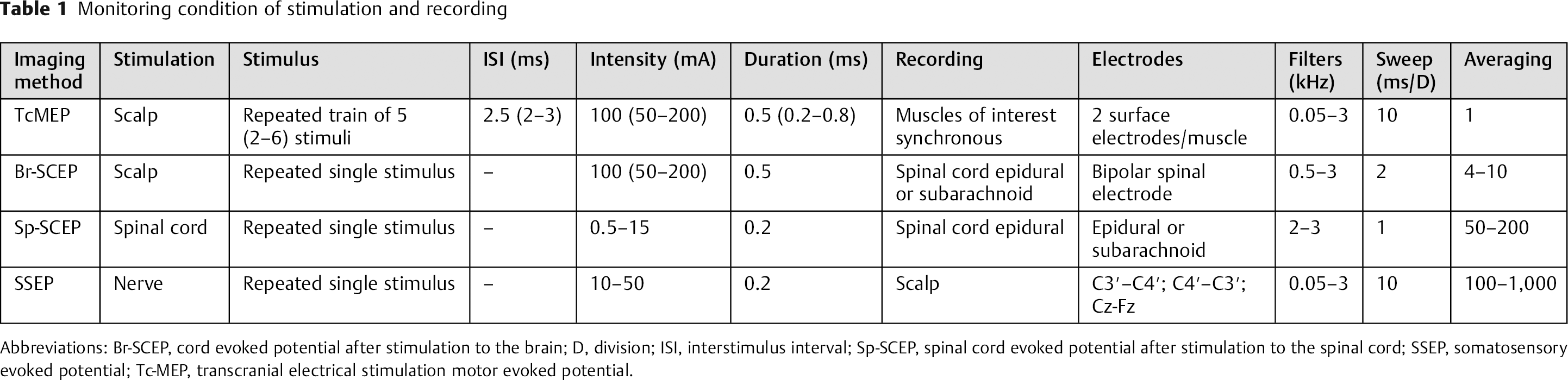
Abbreviations: Br-SCEP, cord evoked potential after stimulation to the brain; D, division; ISI, interstimulus interval; Sp-SCEP, spinal cord evoked potential after stimulation to the spinal cord; SSEP, somatosensory evoked potential; Tc-MEP, transcranial electrical stimulation motor evoked potential.
Of the 7,158 cases, 3,028 met these criteria. In particular, 1,396 cases of single-modality monitoring (SIOM; 17 institutions) and 1,632 cases of MIOM (13 institutions) were selected as the subjects of this study (Fig. 1).
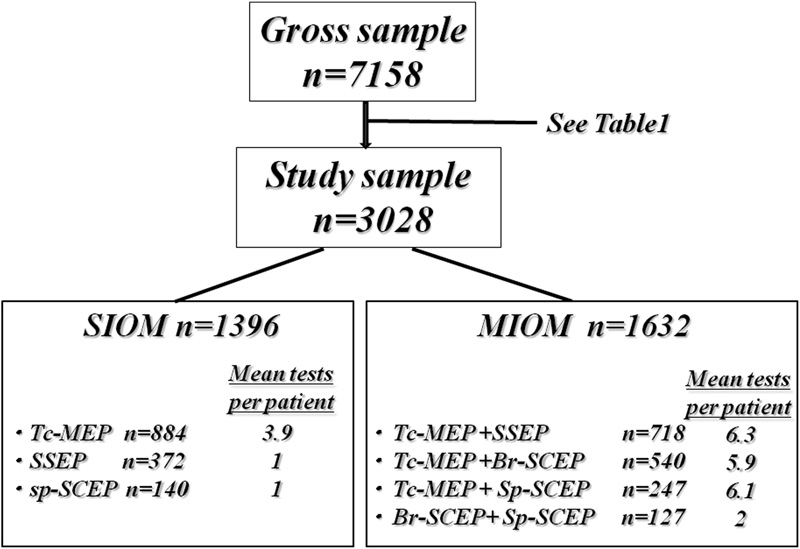
Flowchart of the subjects of this study showing mean tests per patient and mean recording numbers. Abbreviations: Br-SCEP, cord evoked potential after stimulation to the brain; MIOM, multimodal intraoperative monitoring; SIOM, single-modality monitoring; Sp-SCEP, spinal cord evoked potential after stimulation to the spinal cord; SSEP, somatosensory evoked potential; Tc-MEP, transcranial electrical stimulation motor evoked potential.
Tables 2 and 3 show the breakdown of the diseases between SIOM and MIOM groups.
Breakdown in single-modality intraoperative monitoring group
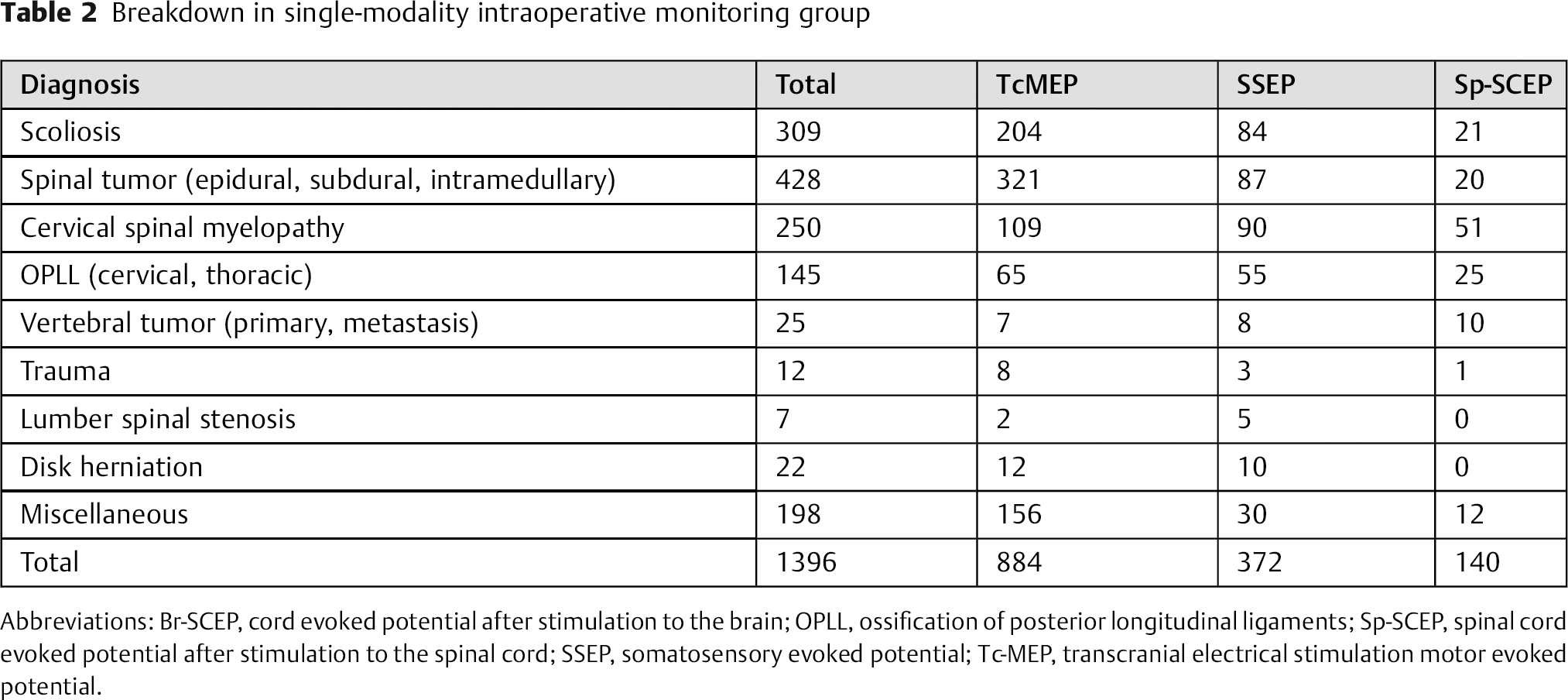
Abbreviations: Br-SCEP, cord evoked potential after stimulation to the brain; OPLL, ossification of posterior longitudinal ligaments; Sp-SCEP, spinal cord evoked potential after stimulation to the spinal cord; SSEP, somatosensory evoked potential; Tc-MEP, transcranial electrical stimulation motor evoked potential.
Breakdown in multimodality intraoperative monitoring group
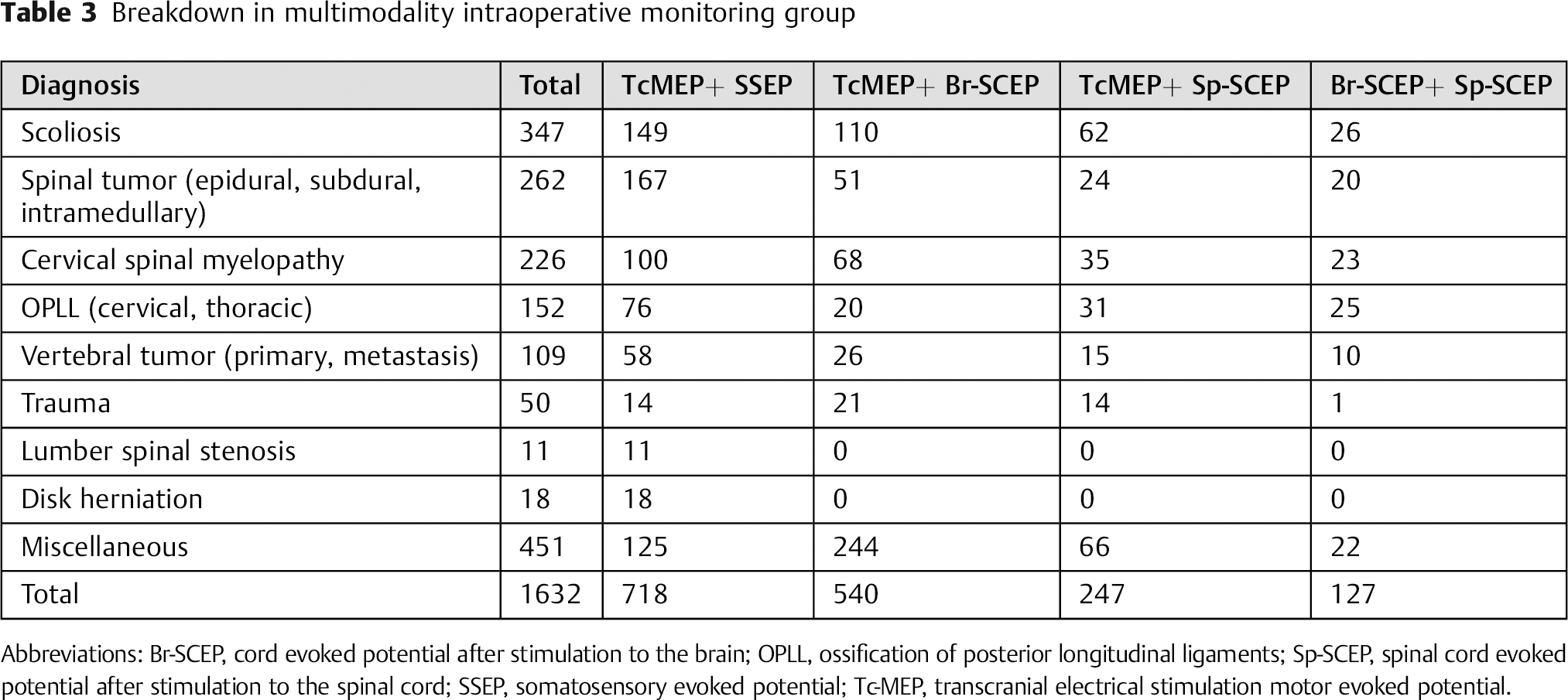
Abbreviations: Br-SCEP, cord evoked potential after stimulation to the brain; OPLL, ossification of posterior longitudinal ligaments; Sp-SCEP, spinal cord evoked potential after stimulation to the spinal cord; SSEP, somatosensory evoked potential; Tc-MEP, transcranial electrical stimulation motor evoked potential.
Examined Items
The sensitivity and specificity (separately for SIOM and MIOM), the false-positive rate, the false-negative rate of each type of monitoring, and the relationship between each type of monitoring and the period of postoperative motor deficit were examined. Statistical analysis was performed using the paired t test.
Results
Fifty-nine cases (1.9%) of postoperative motor deficit were identified with 46 true-positive cases and 13 false-negative cases (Fig. 2). There were 191 false-positive cases with an overall sensitivity of 78% and an overall specificity of 94%.
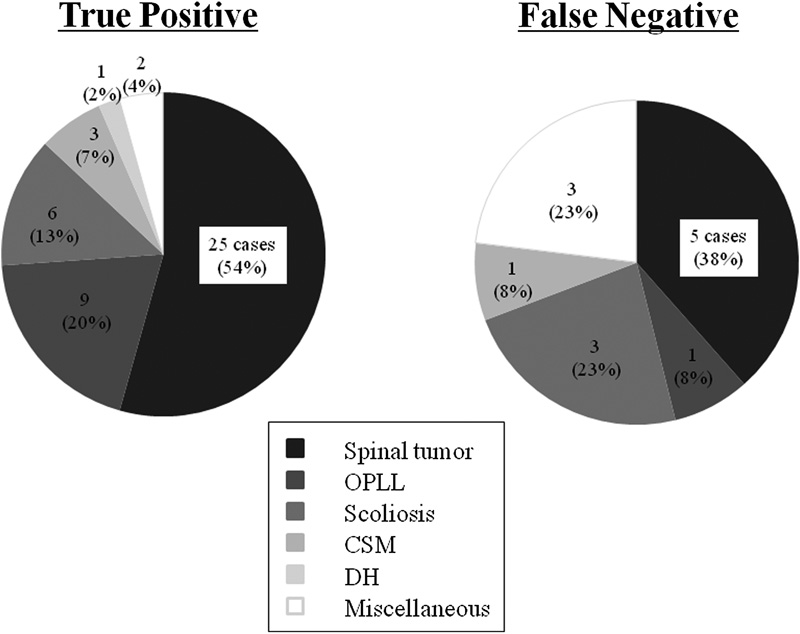
Breakdown and number for motor deficit cases. Abbreviations: CSM, cervical spondylotic myelopathy; DH, disk herniation; OPLL, ossification of posterior longitudinal ligaments.
Sensitivity and Specificity in the Single-Modality Monitoring Group
The SIOM group included 22 cases of postoperative motor deficit, in which 17/884 cases (1.9%) occurred with TcMEP, 3/140 cases (2.1%) with Sp-SCEP, and 2/372 cases (0.5%) with SSEP. The overall sensitivity and specificity in the SIOM group were 72 and 95%, respectively, with a false-positive rate of 5%. Review of each type of monitoring revealed that TcMEP had a significantly higher sensitivity (82%) than Sp-SCEP. The sensitivity was significantly lower in the cases where only Sp-SCEP or SSEP was conducted (SSEP: 50%, Sp-SCEP: 33%; see Fig. 3 and Table 4).
Sensitivity and specificity in the SIOM and MIOM groups

Abbreviations: Br-SCEP, cord evoked potential after stimulation to the brain; MIOM, multimodal intraoperative monitoring; NPV, negative predictive value; PPV, positive predictive value; Sp-SCEP, spinal cord evoked potential after stimulation to the spinal cord; SIOM, single-modal intraoperative monitoring; SSEP, somatosensory evoked potential; Tc-MEP, transcranial electrical stimulation motor evoked potential.
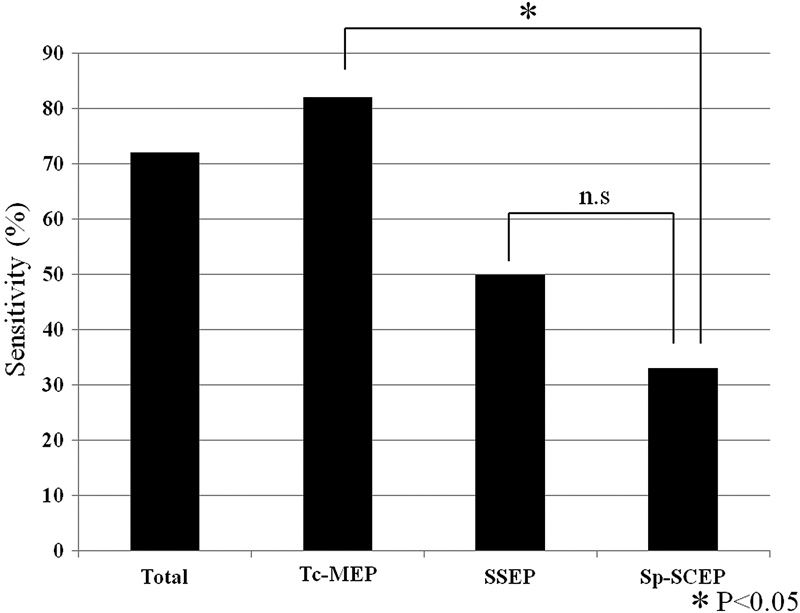
Sensitivity rate for single-modality monitoring group. Abbreviations: n.s., not significant; Sp-SCEP, spinal cord evoked potential after stimulation to the spinal cord; SSEP, somatosensory evoked potential; Tc-MEP, transcranial electrical stimulation motor evoked potential.
Sensitivity and Specificity in the Multimodality Monitoring Group
The MIOM group included 37 cases of postoperative paralysis, in which 10/540 cases (1.9%) occurred with TcMEP + Br-SCEP, 19/718 cases (2.8%) with TcMEP + SSEP, 5/247 cases (2.0%) with TcMEP + Sp-SCEP, and 2/127 cases (2.0%) with Br-SCEP + Sp-SCEP. The overall sensitivity and specificity in the MIOM group were 81 and 92%, respectively, with the sensitivity higher than in SIOM group, but the difference was not statistically significant. The comparison of the various combinations showed the TcMEP + Br-SCEP combination to have the highest sensitivity of 90%. The TcMEP + SSEP and TcMEP + Sp-SCEP combinations each had a sensitivity of 80%, exhibiting little difference between their sensitivity and that obtained when TcMEP alone was used. Meanwhile, the sensitivity was as low as 50% among Br-SCEP + Sp-SCEP cases (i.e., the cases where TcMEP was not included; see Fig. 4 and Table 4).
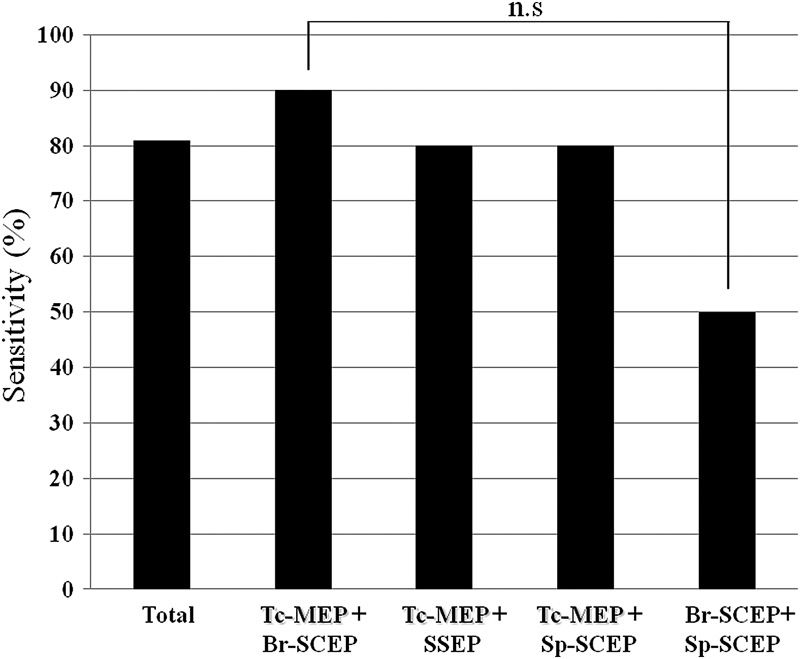
Sensitivity rate for multimodal intraoperative monitoring group. Abbreviations: Br-SCEP, cord evoked potential after stimulation to the brain; n.s., not significant; Sp-SCEP, spinal cord evoked potential after stimulation to the spinal cord; SSEP, somatosensory evoked potential; Tc-MEP, transcranial electrical stimulation motor evoked potential.
False-Positive and False-Negative Rates in Multimodality Monitoring Group
The false-positive and false-negative rate in the overall MIOM group was 7.4 and 0.4%, respectively. These rates were significantly higher in the cases where TcMEP was included (p < 0.005). These rates were significantly lower in the cases where Br-SCEP was included (p < 0.005). Although the difference in the false-negative rates among the combinations was not statistically significant, the TcMEP + Br-SCEP combination registered the lowest rate (0.2%; see Figs. 5, 6 and Table 4).
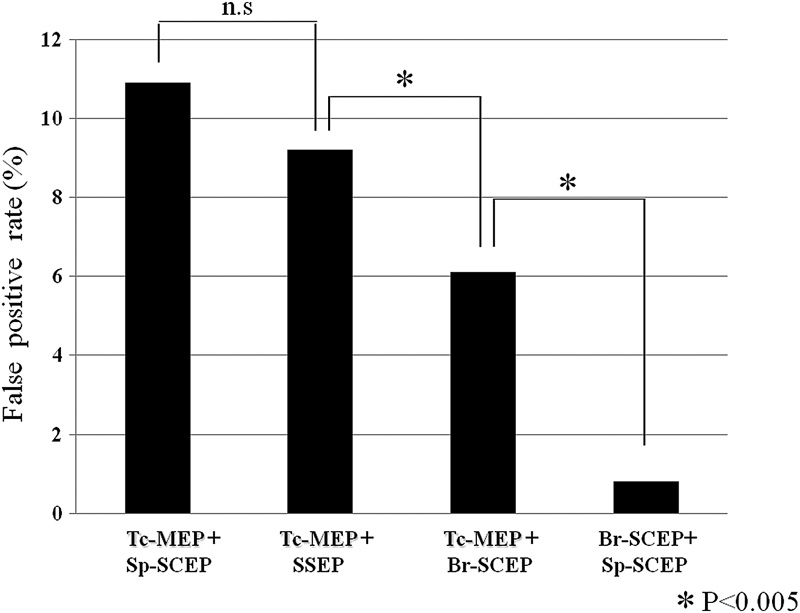
False-positive rate for multimodal intraoperative monitoring group. Abbreviations: Br-SCEP, cord evoked potential after stimulation to the brain; n.s., not significant; Sp-SCEP, spinal cord evoked potential after stimulation to the spinal cord; SSEP, somatosensory evoked potential; Tc-MEP, transcranial electrical stimulation motor evoked potential.
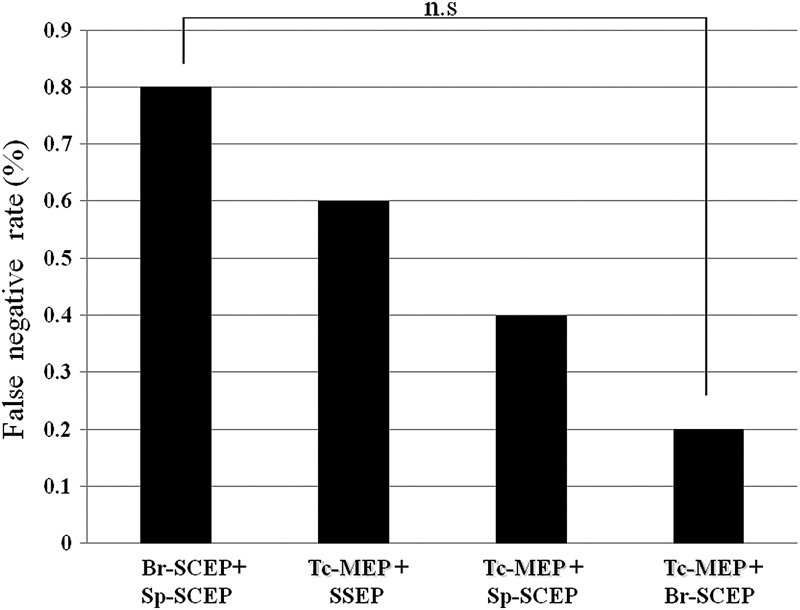
False-negative rate for multimodal intraoperative monitoring group. Abbreviations: Br-SCEP, cord evoked potential after stimulation to the brain; n.s., not significant; Sp-SCEP, spinal cord evoked potential after stimulation to the spinal cord; SSEP, somatosensory evoked potential; Tc-MEP, transcranial electrical stimulation motor evoked potential.
Relationship between Duration of Postoperative Motor Deficit and Monitoring
Of the 59 cases involving postoperative motor deficit, the duration was less than 3 months in 35 cases (59%) and 3 months or more in 24 cases (41%). The postoperative motor deficit continued for 3 months or longer in 10 (45%) of the 22 cases in SIOM group and 14 (38%) of the 37 cases in MIOM group, but the difference between the two groups was not statistically significant. Comparison of the various combinations revealed no significance, either.
Discussion
Among spinal surgeries, intramedullary tumor resection, 2 , 24 ossification of posterior longitudinal ligaments (OPLL) decompression, and scoliosis surgery in particular may have to be performed in critical situations. 25 , 26 , 27 , 28 Although numerous studies reported the advantages of MIOM, they failed to examine the combinations of MIOM methods. Furthermore, no comparisons have been made among the different combinations in terms of sensitivity or specificity.
Although recognizing no significance, this study does show MIOM has a higher sensitivity (81%) than SIOM (72%), thus confirming the greater usefulness of MIOM. Of the MIOM group, the combinations that included TcMEP had particularly higher sensitivities (80% or more) than the Br-SCEP + Sp-SCEP combination (50%), suggesting that TcMEP is essential for spinal monitoring. The group including Br-SCEP had significantly lower false-positive and false-negative rates, indicating the necessity of Br-SCEP for accurate monitoring. In view of the above, it may be concluded that the TcMEP + Br-SCEP combination is the most reliable monitoring with the highest sensitivity of 90% in motor function.
MacDonald et al reported the sensitivity and specificity of TcMEP + SSEP combination as 70% and 93%, respectively, 29 whereas Sutter et al used 11 types of monitoring and reported the overall sensitivity and specificity as 89 and 99%, respectively. 22 Eggspuehler et al used nine types of monitoring for spinal deformity and reported the sensitivity and specificity as 92.3 and 98.5%, respectively. 30 Although overall sensitivity and specificity are reported, no study has reported the rates for the different combinations. In addition, although Sutter et al reported false-positive and false-negative rates of 0.8 and 0.8%, respectively, 22 our false-negative rate was extremely high (7.2%). Presumably, this difference is because Sutter et al normally used at least four modalities and we monitored with three modalities at most. A large number of different surgical procedures were compiled, so we need to study rates in each procedure. However, this report is the first to investigate the combination of MIOM methods for intraoperative spinal cord monitoring, and accordingly it is important as a preliminary study.
One limitation of this study is that after the cases were sorted into different combinations, there were not enough cases of motor deficit in each combination to compare in sensitivity and specificity. Therefore, a study with more cases is needed. Second, this study used no more than two modalities, which was fewer than previous reports. Considering the great deal of labor required, it will be difficult to use a larger number of modalities. Still, studies with more combinations need to be conducted if motor deficits are to be prevented.
Finally, a large number of different surgical procedures were compiled, and each procedure needs to be studied.
Conclusion
The best multimodality combination for intraoperative spinal cord monitoring is TcMEP + Br-SCEP, which had the highest sensitivity (90%), the lowest false-positive rate (6.1%), and the lowest false-negative rate (0.2%).
Disclosures
Zenya Ito, none
Yukihiro Matsuyama, none
Muneharu Ando, none
Shigenori Kawabata, none
Tsukasa Kanchiku, none
Kazunobu Kida, none
Yasushi Fujiwara, none
Kei Yamada, none
Naoya Yamamoto, none
Sho Kobayashi, none
Takanori Saito, none
Kanichiro Wada, none
Kazuhiko Satomi, none
Kenichi Shinomiya, none
Toshikazu Tani, none