
Abstract
Study Design
Randomized controlled trial.
Objective
Adolescent idiopathic scoliosis (AIS) is a common spinal deformity that affects every population. In severe deformity, surgical intervention is performed. Autogenous iliac crest bone graft (ICBG) harvesting remains a common procedure worldwide for scoliosis surgery. Postoperative pain at the ICBG donor site is a major concern in patients undergoing spine surgery that affects postoperative functional outcome and consumes health care resources. Previous studies have noted a decrease in pain and postoperative analgesic use with the application of continuous infusion of anesthetic at the ICBG site in comparison with placebo. However, there is lack of evidence addressing the efficacy of continuous anesthetic infusion at the ICBG site in young patients and in particular those with spinal deformity, such as AIS. As such, this parallel, double-blinded, randomized controlled trial addressed the pain management efficacy of continuous anesthetic infusion versus saline at the ICBG site in patients with AIS during the immediate postoperative period.
Methods
Participants were randomized into two groups. Group A (control subjects) received 3 mL per hour of saline locally at the ICBG site, and group B (treatment subjects) received a constant rate of infusion of 3 mL per hour of 0.25% levobupivacaine. Both groups received their postoperative intervention for 47 hours. All subjects and outcome assessors were blinded to the type of intervention. Utilizing the visual analog pain scale, pain was assessed at the primary spine surgical site, ICBG site, and contralateral ICBG site. Overall physical pain was assessed by the McGill Pain Questionnaire. The degree of analgesic use and complications were also evaluated. All outcomes were assessed up until the fourth day of the patients’ hospitalization following surgery.
Results
Twelve subjects were recruited (five in group A; seven in group B). No difference was noted at baseline regarding age, weight, height, arm span, sex, curve type, instrumented and fused levels, length of hospitalization, and pain scores between groups. Postoperatively, no difference was noted in surgical site pain between groups (p > 0.05). However, decreased ICBG and contralateral ICBG pain decreased twofold in group B patients in comparison with group A. Similarly, group B subjects had notably decreased postoperative overall pain scores (group A, mean 15.3; group B, mean 3.8). No significant differences were noted for the pain scores due to the small sample size.
Conclusions
This study is the first with a robust level I study design to assess the efficacy of continuous infusion of analgesia into the ICBG site in young patients with AIS. This pilot study noted a trend that continuous anesthetic infusion reduces pain at the ICBG site and may further decrease overall physical bodily pain. This study further established a sample size calculation to facilitate large-scale studies addressing these parameters. This study provides further support of postoperative pain management options for children with spinal deformities.
Introduction
Adolescent idiopathic scoliosis (AIS) is a common spinal deformity that occurs in every population worldwide. 1 For severe curves, surgical intervention is sought to decrease the deformity and improve daily function. As such, spinal fusion procedures are commonly performed and often entail the use of autogenous iliac crest bone graft (ICBG). 2
The iliac crest is a common donor site for autograft bone harvesting in spine surgery procedures due to its easy access and high structural integrity; it is an excellent source for cortical and cancellous bone. 3 However, various complications are associated with autologous ICBG harvesting and include potential injury to the neurovascular structures, donor site visceral herniation, fracture or pelvic instability, hematoma, sensory disturbances, deep wound infections, and cosmetic deformity. 4 , 5 , 6 A major concern following bone harvesting from the anterior or posterior iliac crest is postoperative donor site pain. 3 , 4 , 6 , 7 , 8 , 9 The incidence of postoperative iliac crest donor site pain varies, depending on the postoperative time interval, technique of assessment, location of the donor site, primary surgical site, and methodological study limitations. 10 Nonetheless, such pain has been reported to occur in 2.8 to ∼49% of cases. 3 , 6 , 7 , 8 However, studies have noted that up to 39% of the patients undergoing ICBG harvesting reported chronic postoperative pain (3 months or greater) stemming from the donor site. 3 , 4 , 7 As a result, functional activity could be impaired, affecting ambulation, recreational and daily living activities, work and professional duties, and sexual activity. 4 Such donor site pain could also have severe pharmacologic implications from prolonged use of analgesic medication, which is also fraught with potential complications (e.g., dependency, nausea, vomiting, dizziness, increased health care costs, etc.). 4 However, in an effort to reduce or prevent postoperative iliac crest donor site pain, several surgical techniques have been proposed regarding variation in harvesting methods and reconstruction of the donor site. 3 Nonetheless, such techniques were not found to conclusively improve postoperative iliac crest donor site pain.
The application of an anesthetic agent (e.g., bupivacaine) on non–iliac crest-specific wound sites in orthopedic and other surgical procedures was found to decrease postoperative pain and narcotic usage, 11 but a consistent, significant difference between the anesthetic and saline or control in some studies has not been clearly demonstrated, which suggests that anesthetic analgesic control may depend on the operative site. 12 Nonetheless, various studies have noted that the analgesic effects associated with local anesthetic application seem to outlast the expected duration of the anesthetic agent. 13 Several authors contend that such effects in deep tissue injuries are possibly attributed to the decrease of spinal cord receptor field changes and hyperexcitability due to the immediate reduction of noxious afferent input afforded by local anesthetic application. 14
Several randomized and nonrandomized prospective studies have noted that the application of an anesthetic agent on the donor site following bone graft harvesting from the iliac crest to address non-spine-specific procedures resulted in decreased postoperative donor site pain, analgesic use, and hospitalization. 15 Studies have also noted that application of donor site anesthetic immediately following surgery not only improves pain in the postoperative short term, but significantly improves long-term pain in comparison with individuals without such intervention. 16 Furthermore, based on randomized controlled trials, the use of continuous anesthetic infusion on the donor site, including the ICBG site, has demonstrated a reduction in postoperative pain and analgesic use in adults. 9 , 15 , 17 , 18 , 19 Thus, such effects may conceivably translate into reduced health care costs and a quicker return to daily activities. 4
Based on the literature, the postoperative pain management of the ICBG donor site in children who receive surgical treatment for AIS remains in contention, which is of particular importance because recent studies have noted that the rate of postoperative acute pain in children undergoing orthopedic procedures is ∼84% (13% chronic pain) and that over 30% of subjects reported that such pain interferes with their sleep, social functioning, and extracurricular activities. 20 According to Skaggs et al, 2 the authors noted that in children undergoing spinal fusion who underwent posterior ICBG, 24% reported donor site pain and 15% noted that the pain was severe enough to interfere with daily activities even up to a mean of 55 months after surgery. Furthermore, although not fully understood, childhood pain experiences may “increase” the risk of psychological issues in adulthood. 21
In many centers around the world, ICBG is still harvested for various spine surgeries, including procedures to treat AIS. 22 , 23 , 24 , 25 As such, we conducted a double-blinded, randomized controlled clinical trial to address the immediate efficacy of postoperative pain management comparing continuous infusion of saline to anesthetic at the posterior ICBG donor site in patients with AIS.
Methods
Study Design and Participants
This study was a parallel, double-blinded, randomized controlled trial of participants of Southern Chinese origin with AIS undergoing posterior spinal fusion with autogenous posterior ICBG at the Duchess of Kent Children's Hospital in Pokfulam, Hong Kong. Each subject was screened to determine eligibility for the study. Participants who weighed less than 35 kg were excluded due to the fear of medical overdose. Individuals who had undergone previous spine surgery and/or ICBG harvesting, had known allergies to levobupivacaine and morphine, were pregnant or lactating, had infection at the site of bone graft harvesting, had a history of blood coagulation disorders or pulmonary embolism, had known psychological disorders, and had any additional comorbidities or criteria that led the investigators to believe that the subject may not comply with the study protocol were excluded. All participants were between 10 to 18 years of age at the time of surgery.
The study was approved by the Institutional Review Board of The University of Hong Kong and the Hong Kong West Clusters Hospital of the Hospital Authority and was registered with Hong Kong Clinical Trials (HKCTR-1247). Participation was voluntary, and informed consent was obtained from all subjects as well as their guardians. The protocol of the study was described to all subjects at the time of recruitment, and documentation was provided to them in a language they understood, noting that at any time during the study they had the right to withdraw without justification.
Sample Size
Due to the absence of similar trial designs addressing the stated parameters in children with AIS, there was a lack of evidence to facilitate the sample size calculation with confidence. As such, our initial recruitment of participants served as a pilot study.
Operative Procedure
All subjects were placed prone in a knee–chest position and underwent posterior instrumentation and fusion. Through a 3-cm incision over the posterior superior iliac crest, the incision was carried down to bone, and the periosteum was subperiosteally elevated to expose the outer table of the iliac wing. A chisel and gouge were used to remove the outer cortex of the iliac wing along with the underlying cancellous bone. Hemostasis was achieved using bone wax and gel foam, and the wound was irrigated with normal saline before closure with absorbable sutures in layers. No drain was placed. The amount of bone graft harvested was approximately the same between all subjects. A deep wound epidural catheter was applied at the ICBG donor site to facilitate local anesthetic infusion. Each subject also had access to morphine patient-controlled analgesic (PCA) for up to 48 hours postoperatively per standard of care.
Intervention
The subjects were randomized into two groups. Group A consisted of control subjects and group B consisted of treatment subjects. Both groups received 5 mL of 0.5% levobupivacaine locally at the ICBG site followed by 1-hour washout of the single bolus injection. The single bolus injection was performed as such to maintain the standard of care that has been traditionally offered at our institute. After the bolus, group A received an infusion of 3 mL of saline solution per hour for 47 hours, and group B received continuous infusion of 0.25% levobupivacaine 3 mL per hour for 47 hours at the posterior iliac crest donor site. All subjects were blinded to the type of intervention they received (Fig. 1). All patients received standardized oral analgesics postoperatively. Paracetamol (1 g) was given four times daily, and 50 mg of oral tramadol was given up to four times daily as needed.
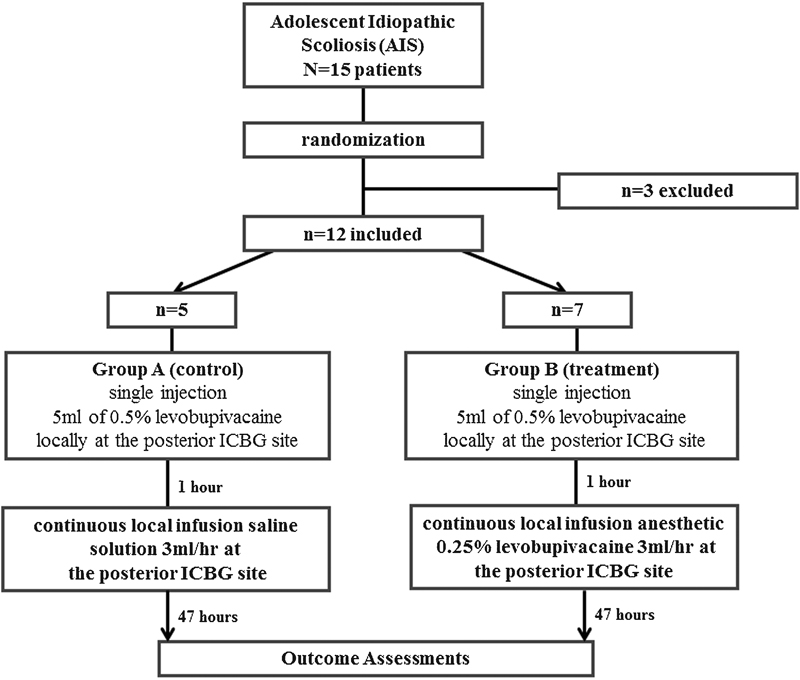
Flowchart of study recruitment. Abbreviation: ICBG, autogenous iliac crest bone graft.
Each subject was equipped with a continuous infusion syringe pump for 48 hours. An Injectomat MC Agilia dose rate syringe pump (Fresenius Kabi, Homburg, Germany) was utilized to administer the local single dose bolus and continuous anesthetic/saline infusion. The device allowed for a programmable continuous flow rate and accommodated a 50-mL syringe. To ensure the quality of the measurements and minimize the risk of measurement error, the outcome assessors underwent training to familiarize themselves with the operation and programming of the syringe pump. The syringe was refilled every 16 hours. The investigators had chosen a continuous infusion dose of 3 mL of 0.25% levobupivacaine per hour, which was believed to be a safe, nontoxic dose while maintaining a therapeutic benefit.
On the day of the surgery, all patients were confined to bed rest. On the first postoperative day, all patients were allowed to sit in the bed and begin standing exercise if tolerable. All patients began walking exercises on postoperative day 2. Patients were discharged from the hospital when they were able to ambulate independently and had a stable wound condition.
Outcomes
The primary outcomes of the study entailed the preoperative and postoperative assessment of donor site pain and the amount of postoperative analgesic use. Pain assessment was based on the visual analog scale (VAS) and the McGill Pain Questionnaire. 26 Pain at the donor site was assessed preoperatively and every 12 hours following surgery during the course of hospitalization (minimum 5 days) by an individual blinded to the intervention allocation of the patients. In addition, the pain assessment of the primary spine surgical site as well as the contralateral region of the ICBG site was also performed. The VAS score ranged from 0 to 10, with higher scores noting more severe pain. The physical quality component (potential score range: 0 to 45) of the McGill Pain Questionnaire was used to assess the overall physical/bodily pain, which translated as the higher the score, the worse physical pain experience. All subjects at the time of assessment were asked to rate their pain at its most severe. Analgesic use was based on the morphine PCA usage, recording the frequency of usage every hour for each postoperative day. The PCA machine only allowed a preset dosage of analgesic dependent on patient body weight within a 1-hour interval. The number of times patients reached the maximum allowable dose was recorded. The patient and outcome assessor were blinded to the treatment allocation throughout the trial.
Each participant was evaluated for potential donor site complications, such as, hematoma, infection, allergic response, and overdose (convulsions, cardiac problems). Each participant was assessed for the event of analgesic-related complications, such as dizziness, nausea, and vomiting. In addition, each participant was assessed during their course of medical care throughout the year for any symptoms or complications related to their primary spine surgery.
Participant demographics, surgical characteristics, and management were tabulated, accounting for sex, age, body weight and height, arm span, type of spinal deformity based on the Lenke classification, 27 duration of surgery, vertebral levels that were fused, and hospitalization duration. In addition, the study was monitored for safety and efficacy of the interventions. If at any point the investigators felt that the study presented a known harm to the participant, the study was terminated.
Randomization and Blinding
Block randomization was generated by a statistician, independent of the outcome assessment, via a statistical program to ensure equal intervention group assignment of 1:1. The intervention assignment was concealed until the surgical date. The participants and outcome assessors were blinded to the type of intervention each group received.
Statistical Methods
All data was collected and coded upon a spreadsheet. The SPSS version 21 (IBM, Chicago, Illinois, United States) statistical software program was utilized to perform the statistical analyses. Descriptive and frequency analyses were conducted of all data parameters. Significance testing was performed, whereby p values and 95% confidence intervals were obtained. If normal distribution was maintained, the independent samples t test was used to assess the mean differences between the groups. The paired samples t test was conducted to assess differences in the pre- and postoutcome parameters. The Fisher exact test was utilized to assess proportional differences between the categorical data parameters. Nonparametric tests were considered accordingly. Evaluation of the extreme outliers was assessed of all data points. If the sample size allowed, subgroup analyses was considered and based on subject demographic and spine-related deformity parameters in relation to the postoperative pain parameters. An intent-to-treat analysis was considered for participants lost to follow-up or who withdrew from the study. All statistical tests were two-sided. The threshold for statistical significance was p < 0.05.
Results
From February 2012 to July 2013, a total of 15 participants were enrolled in this study. Three female participants (control group) were excluded from the study: 2 due to infusion pump blockage and 1 due to termination of the operation as a result of intraoperative drop of motor evoked potential. As such, 12 subjects were included for this study (Fig. 1). Five subjects were allocated to group A (control group) and 7 were allocated to group B (treatment group). There were 2 male and 3 female subjects in group A, and 1 male and 6 female subjects in group B (p = 0.524). There were also no differences noted at baseline regarding age, weight, height, body mass index, arm span, and length of hospitalization (Table 1). Details about the spinal deformity and operation performed are listed in Table 2. There were no differences between the groups for the type of spinal deformity (p = 0.794), number of fused levels (p = 0.544), number of instrumented levels (p = 0.069), and duration of surgery (p = 0.285).
Study group characteristics
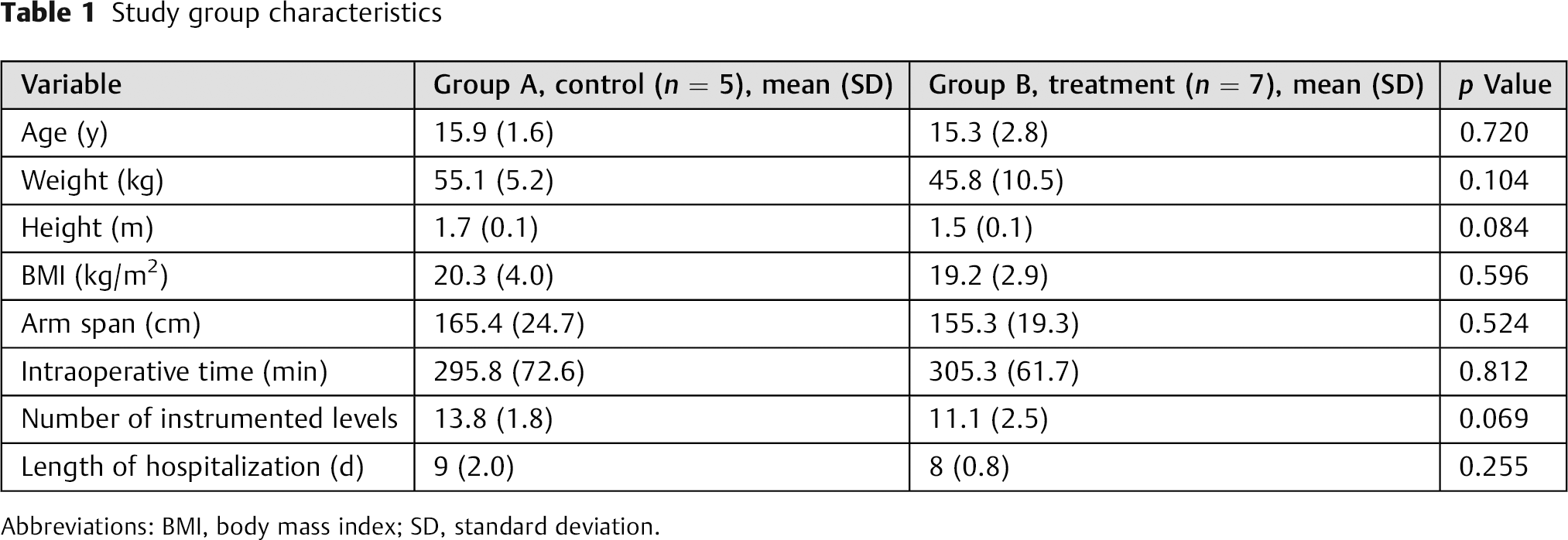
Abbreviations: BMI, body mass index; SD, standard deviation.
Characteristics of patients’ spinal deformity and operative profile
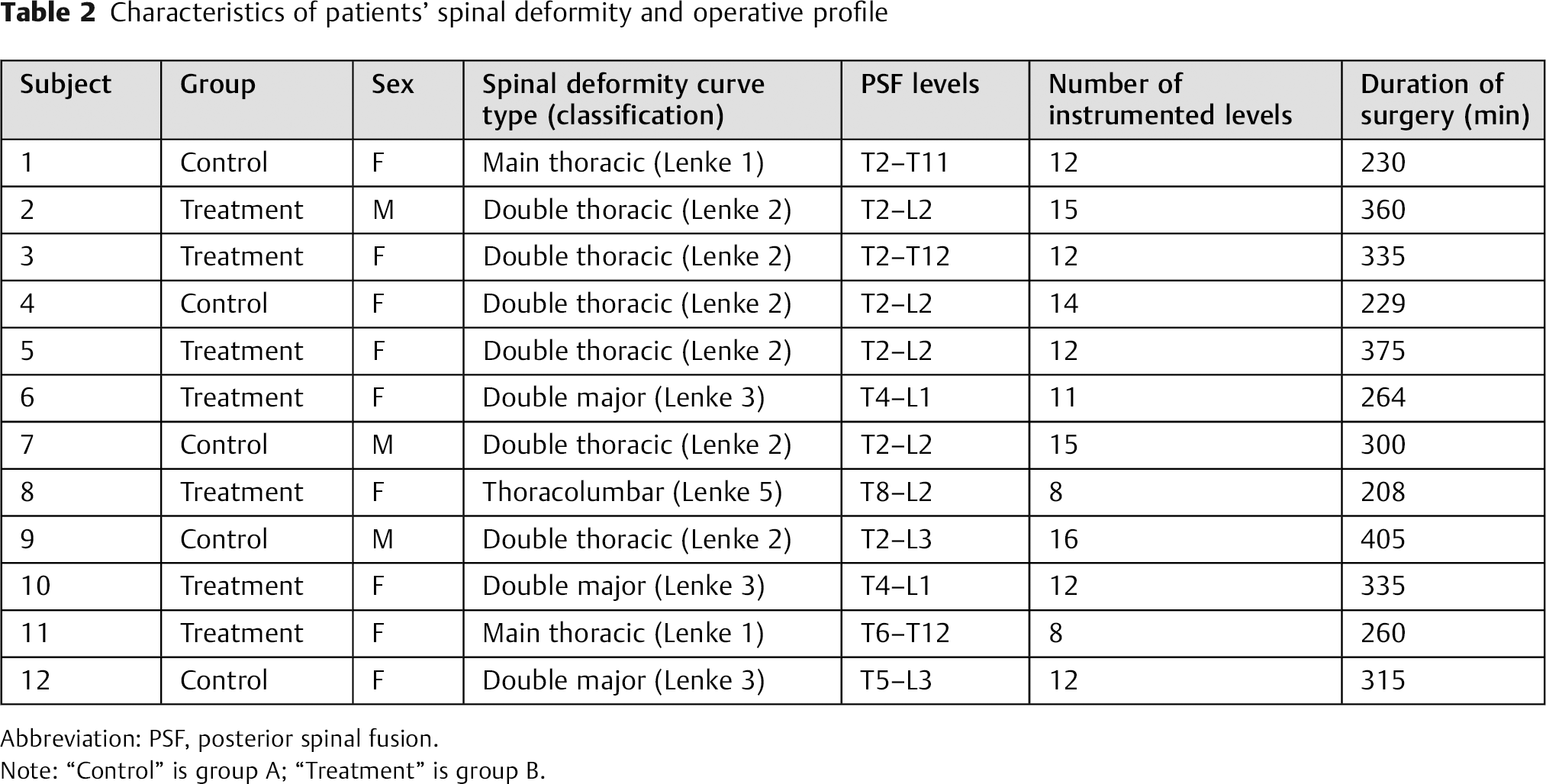
Abbreviation: PSF, posterior spinal fusion.
Note: “Control” is group A; “Treatment” is group B.
No statistically significant difference was noted between groups in pain scores at baseline (p > 0.05). Postoperatively, no statistically significant difference was noted at the primary spine surgical site between the groups throughout hospitalization (p > 0.05). There was up to a twofold decrease in ICBG and contralateral iliac crest pain in group B (cases) as compared with group A (controls) in the first 2 days after surgery, which coincided with the conclusion of their 47-hour intervention (p > 0.05; Fig. 2). The mean VAS pain scores at the ICBG site during postoperative days 1 and 2 were 4.0 (standard deviation [SD] ± 3.7) and 3.4 (SD ± 2.2), respectively, for group A. The mean VAS pain scores at the ICBG site during days 1 and 2 were 2.6 (SD ± 2.8) and 2.3 (SD ± 1.8), respectively, for group B. The mean VAS pain scores for the contralateral iliac crest site during postoperative days 1 and 2 were 3.50 (SD: ± 4.1) and 1.2 (SD: ± 1.8), respectively, for group A. The mean VAS pain scores during days 1 and 2 were 1.4 (SD: ± 1.9) and 0.6 (SD: ± 1.0), respectively, for group B. At the conclusion of the intervention, the mean McGill pain scores for group B (mean: 3.8; SD: ± 6.3) had approximately a fourfold decrease as compared with controls (mean: 15.3; SD: ± 14.8; p = 0.158; Fig. 3).
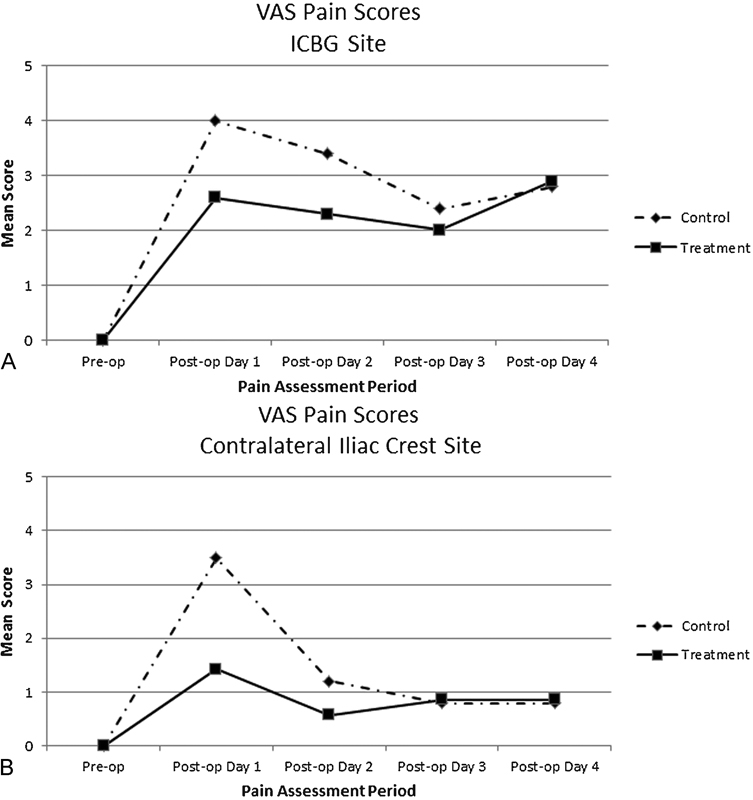
Visual analog scale (VAS) pain assessment outcomes. (A) Pain at the iliac crest bone graft (ICBG) site and (B) pain at the contralateral iliac crest site. Note that “Control” is group A and “Treatment” is group B.
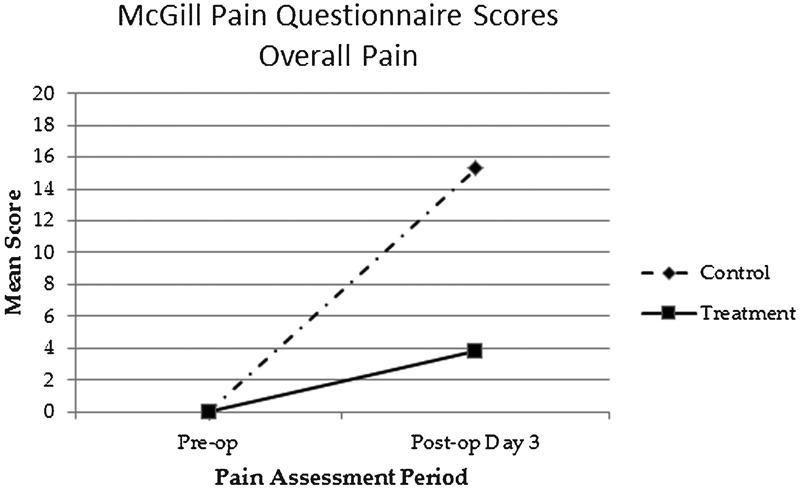
McGill Pain Questionnaire scores assessing overall physical pain. Abbreviations: pre-op, preoperative; post-op, postoperative.
The mean cumulative PCA morphine doses received at the conclusion of the intervention were 20.8 mg (SD: ± 13.0 mg) and 25.7 mg (SD: ± 20.5 mg) for groups A and B, respectively (p = 0.650). However, 80% of group A as opposed to 72.1% of group B had pressed the PCA button more times than allowed (p = 1.000). Although these results were not statistically significant, those patients who did not require more analgesia than their PCA maximum had lower mean VAS pain scores in the first postoperative day at the primary surgical spine site (2.3 versus 3), contralateral iliac crest site (0.5 versus 1), and ICBG site (4 versus 6). This result was similar for the second postoperative day for the primary surgical spine site (1.5 versus 3.5) and the ICBG site (3.8 versus 5.8). The contralateral iliac crest pain on postoperative day 2 was the same (VAS 1) for both groups.
Postoperative complications included only one wound dehiscence noted at the ICBG site in group A, which required a single debridement procedure and closure 5 days after the initial surgery. No complications of hematoma, allergic response, or overdose to medications were noted. There were also no analgesic-related complications, such as dizziness, nausea, or vomiting.
Discussion
Our level I randomized controlled trial is the first in young patients with AIS to assess the efficacy of continuous anesthetic (i.e., levobupivacaine) infusion at the ICBG site in comparison with a control group receiving saline. Our preliminary findings noted that continuous infusion of anesthetics decreased pain at the ICBG site almost twofold and also decreased overall physical pain fourfold in a group of Southern Chinese participants. These early findings are promising as to the potential pain management options for patients with AIS whereby bone graft is still harvested from the iliac crest site.
Levobupivacaine is a local anesthetic that temporarily inhibits sodium passage through voltage-gated ion channels in the neuronal membrane, thereby allowing a reversible transmission blockage of action potentials of sensory, motor, and sympathetic nervous fibers. Although excessive dose of the anesthetic or accidental intravascular injection may affect other ion channels and lead to central nervous and cardiovascular complications, the margin of safety of this anesthetic is greater than its counterpart bupivacaine. Furthermore, studies have noted the safety of levobupivacaine in the pediatric population for continuous infusion application. 28
Pain is a complex symptom that can be affected by many parameters including patients’ pain perception and tolerance. Although the cases and controls were similar in terms of PCA usage, the individuals receiving continuous anesthetic infusion (treatment group) reported a lower postoperative VAS score and used the PCA button less than the control group. By subclassifying the subjects into those who were satisfied with the amount of analgesics given (not pressing the button more than allowed) and those who were unsatisfied (pressing the button more than the allowed dosage), we could see that the latter group had worse VAS scores across all parameters as compared with the former group. This observation implied that despite having the same amount of analgesics, those subjects with poor pain tolerance would likely require more pain relief and rank their pain worse than others with better pain tolerance. This finding was more significant in our group of patients because none of them knew whether they received iliac crest infusion or saline and none of the subjects had any adverse effects from PCA use including nausea or vomiting. Likewise, subjects who had improved ICBG VAS pain scores with iliac crest continuous anesthetic infusions also had improved pain scores in the contralateral iliac crest. This observation may be attributed to individual perception of pain relief, referred pain, or perhaps an inability to distinguish the two sites in these young patients.
We would like to discuss several study limitations and strengths. Our study did not achieve any statistically significant difference between different parameters following surgery, which was attributed to the small sample size of our recruitment. However, we did note trends of decreased pain, approximately twofold, in patients who underwent continuous infusion of levobupivacaine at the ICBG site compared with the control group during the entire duration of such intervention (i.e., the first 47 hours after surgery). After the interventions were not available, the pain severity normalized between groups and was similar between all subjects. Although our study is regarded as a pilot study, based on the initial postoperative pain assessment, we have calculated that with 80% power and an α value of 0.05, a sample size of 87 subjects per study arm would be needed to demonstrate a statistically significant difference during the first day following surgery. Interestingly, to achieve a significant effect for overall physical pain relief via this intervention method, a minimum of 16 subjects per study arm would be needed. As such, our study forms the foundation for future, larger-scale studies assessing such pain management in patients with AIS. In addition, our study focused on a homogenous ethnic group of Southern Chinese patients, which is a particular strength. Ethnic variations may affect pain reporting and management, 29 which further underscores the importance to address pain parameters in AIS in a specified ethnic group, such as Chinese, which represents a quarter of the world's population. Nonetheless, our findings, which noted a trend of decreased pain with continuous anesthetic use at the ICBG site compared with control subjects, further replicates what other studies have noted in adult subjects and in non-Chinese patients. 9 , 15 , 17 , 18 , 19 As such, our findings may be generalized to other ethnic groups and populations.
Conclusions
To our knowledge, this study is the first randomized controlled trial to assess the efficacy of continuous infusion of analgesia into the ICBG site in young patients with AIS. The preliminary results based on our pilot study have noted a trend that continuous anesthetic infusion reduces pain overall and at the ICBG site. Such a finding may have potential to improve postoperative pain management, which can lead to further decreases in health care costs, improved utility, and enhanced outcomes in young children with spinal deformities. However, larger studies are needed to further address these issues and validate our preliminary findings, which may affect clinical decision making. This study further established a sample size calculation to facilitate future large-scale studies addressing these parameters.
Disclosures
Dino Samartzis, none
Cora Bow, none
Jason Pui Yin Cheung, none
Phoebe Sham, none
Kin-Cheung Mak, none
Wai-Yuen Cheung, none
Yat-Wa Wong, none
Keith D. K. Luk, none
Kenneth M. C. Cheung, none
Jean-Claude Lawmin, none
Footnotes
Acknowledgments
The authors thank the Hong Kong Theme-Based Research Scheme (T12-708/12N) for their support of this study. We would also like to thank the orthopedic nursing staff at the Duchess of Kent Children's Hospital, Pokfulam, Hong Kong for all their help with the recruitment of participants, equipment maintenance, and data collection for this study. In addition, we appreciate the pharmacy staff at the hospital for their assistance in preparing the solutions for the infusion pump.