
Abstract
Diabetic neuropathy (DN), one of the most common late complications of diabetes mellitus, significantly affects distinct regions of the nervous system. Pain management is challenging in DN as no effective therapies exist that reverse the pathological course of DN. Several drugs are recommended as the first-line treatment for painful DN, but these are associated with various side-effects in the long term. This report presents two cases with painful DN who underwent lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion. The two cases were followed for 30 days. Lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion offered effective pain relief and improved the health-related quality of life in two patients with DN over this time period.
Keywords
Introduction
Diabetes mellitus is a syndrome characterized by high blood glucose concentration, frequent urination and increased thirst and hunger. Diabetic neuropathy (DN), one of the most common late complications of diabetes mellitus, significantly affects distinct regions of the nervous system. 1 The rate of DN in diabetes mellitus varies widely, ranging from 7.5% to 23.5%.2,3 Although the symptoms of DN are different in different patients, over one-third of the diabetic population has reported to be affected by neuropathic pain. 4 Painful symptoms take many forms, including burning, tingling, shooting and lancing; and over time, pain can co-exist with sensory loss. A previous study demonstrated that the progression of neuropathic pain initially occurs in toes and feet with typical ‘glove and stocking’ pattern of distribution. 5 Furthermore, DN can change over time. Neuropathic pain becomes worse at night and affects sleep, but it should be noted that not all patients with diabetes mellitus develop the symptoms of DN. For example, it has been reported that almost half of neuropathic patients can be asymptomatic. 6
Continuous epidural analgesia through percutaneous epidural catheters with or without steroids is effective in treating acute and chronic pain. Previous studies have reported that continuous epidural analgesia has been used to treat many diseases such as childbirth analgesia and acute herpes zoster pain.7,8 However, little information is known about the treatment of DN with nerve blocks. This report describes the use of lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion in two cases to treat the symptoms of pain associated with DN and to improve quality of life.
Case reports
Case report 1
The first case was a 73-year-old male with right lower limb pain. In March 2002, the patient was diagnosed with type 2 diabetes mellitus and required antidiabetic drugs (1000 mg metformin orally daily and 0.3 g acarbose orally daily). Three months ago, his right lower limb presented with intermittent intolerable lancinating pain accompanying anaesthesia. He was treated with analgesics (300 mg tramadol orally daily) and anticonvulsants (1800 mg gabapentin orally daily; 150 mg pregabalin orally daily) to reduce the pain. The drugs were effective for the first few days but became ineffective over time. The pain was sharp and severe. At night, the right lower limb pain seemed to be particularly aggravating and seriously affected the patient’s quality of sleep. Therefore, the patient was admitted to the Department of Pain Management, Wuhan First Hospital, Wuhan, Hubei Province, China in May 2017. Physical examination showed allodynia or hyperalgesia of the right lower limb. A significantly decreased sensation coexisted with the pain. Electromyography of the bilateral lower limbs showed the peripheral nervous system of the lower limbs was damaged. No diabetic ulcers were observed on the skin. Blood tests showed the level of blood glucose was 6.4 mmol/l, glycosylated haemoglobin (HbA1c) was 7.1% and C-reactive protein was 3.11 mg/l.
Case report 2
The second case was a 57-year-old female with a 12-year history of type 2 diabetes mellitus who had numbness and tingling in her right foot. The patient was admitted to the Department of Pain Management, Wuhan First Hospital in March 2017. The patient had a history of peripheral neuropathy and proliferative retinopathy. The patient described her symptom as a burning pain that frequently occurred during the day. The pain was so serious that it not only affected her ability to walk, but it also woke her up from sleep at night. Her medications included antidiabetic drugs (1000 mg metformin orally daily and 0.3 g acarbose orally daily), insulin (8U-12U-10U, insulin aspart, before three meals, subcutaneous injection; 14U, insulin detemir, immediately before sleeping, subcutaneous injection), anticonvulsants (1800 mg gabapentin orally daily; 150 mg pregabalin orally daily), analgesics (300 mg tramadol orally daily) and aspirin (100 mg aspirin orally daily). No significant past medical history was found. On physical examination, the pain mainly occurred in her right foot with an absence of ankle reflexes. Sensation in her right lower limb was decreased. Electromyography showed absent sensory and motor responses, but the strength of the bilateral lower limbs was normal. Laboratory studies showed a high level of blood glucose (12.4 mmol/l) and HbA1c (8.5%).
On admission to hospital, the two cases were evaluated by radiological imaging (transabdominal ultrasound, computed tomography and magnetic resonance imaging) and had no nerve abnormalities related to disc extrusion with compression of the nerve roots. Electromyography showed that the muscles of the lower limbs in each patient had neurogenic changes. The study was conducted in accordance with the principles of the Declaration of Helsinki and the guidelines of Wuhan First Hospital. Written informed consent was obtained from both patients.
Lumbar sympathetic pulsed radiofrequency with continuous epidural infusion
The plasma glucose level in the patients was routinely examined 1 h before therapy. Patients were taken to the operating room and placed in the prone position. The puncture sites (usually L4/L5 or L5/S1) were localized using X-rays of the patients. The puncture needle was guided into the lumbar nerve root in the lateral view. Careful examination was needed to make sure that the puncture needle was placed at the expected position in the posterior-anterior view. The core of the puncture needle was retracted and the electrode was inserted into the lumbar nerve root though the puncture needle. At the same time, heat from the radiofrequency energy was provided at 40 °C and 60 °C in two cycles.
Next, under the guidance of X-rays, a puncture point was selected at L2/L3 and the puncture needle was inserted into the epidural space. After successful puncture, a catheter was placed close to the lumbar nerve root at the fourth lumbar vertebra. Meanwhile, contrast medium was injected into the epidural space to ensure that the catheter arrived at the destination point. Then 5 ml of liquid local anaesthetic mixture (2% lidocaine + 1.5 mg/ml betamethasone +0.9% normal saline) was injected into the lumbar nerve root. Finally, the catheter was connected to an analgesic pump with 250 ml of liquid local anaesthetic mixture (70 ml 2% lidocaine + 180 ml 0.9% normal saline) for continuous infusion at a rate of 3 ml/h. The continuous infusion was continued for 1 week.
Pain assessment and health-related quality of life
The pain assessment of the two cases was evaluated using a visual analogue scale (VAS). The VAS score ranges from 0 to 10: 0–3 indicates no pain; 4–6 indicates mild pain; and 7–10 indicates severe pain. The two cases were evaluated before therapy (baseline) and at intervals of 1, 3, 5, 7, 14 and 30 days after therapy. The two patients had severe DN pain before therapy (case 1, VAS score 7; case 2, VAS score 6) (Figure 1). The pain in both cases reduced after therapy. However, it should be noted that pain recurred on days 3 and 5 after therapy. By day 30, the VAS scores of the two cases had reduced to < 3 and the patients reported satisfactory pain relief (case 1, VAS score 1; case 2, VAS score 0). In addition, a lower dosage of tramadol per day was consumed after the therapy compared with baseline (50 mg versus 300 mg, respectively; one case discontinued tramadol and the other used 50 mg per day).

Assessment of pain using a visual analogue scale (VAS) score in two patients with painful diabetic neuropathy at baseline and after undergoing lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion.
The short-form (SF)-36 questionnaire was used to evaluate health-related quality of life. 9 The questionnaire has eight domains: physical functioning (PF), physical role functioning (RP), bodily pain (BP), general health perceptions (GH), emotional role functioning (RE), vitality (VT), mental health (MH) and social role functioning (SF). The two cases were assessed using the SF-36 questionnaire before therapy (baseline) and at 30 days after therapy. Compared with baseline, the mean quality of life of the two cases had improved at 30 days after therapy: PF 51.65 versus 73.75; RP 50.00 versus 75.00; GH 38.75 versus 65.00; VT 40.00 versus 79.00; SF 60.85 versus 78.25; RE 50.00 versus 91.65; MH 37.50 versus 77.45; respectively) (Figure 2). However, the BP domain was lower at 30 days after therapy compared with baseline (22.55 versus 76.60, respectively).
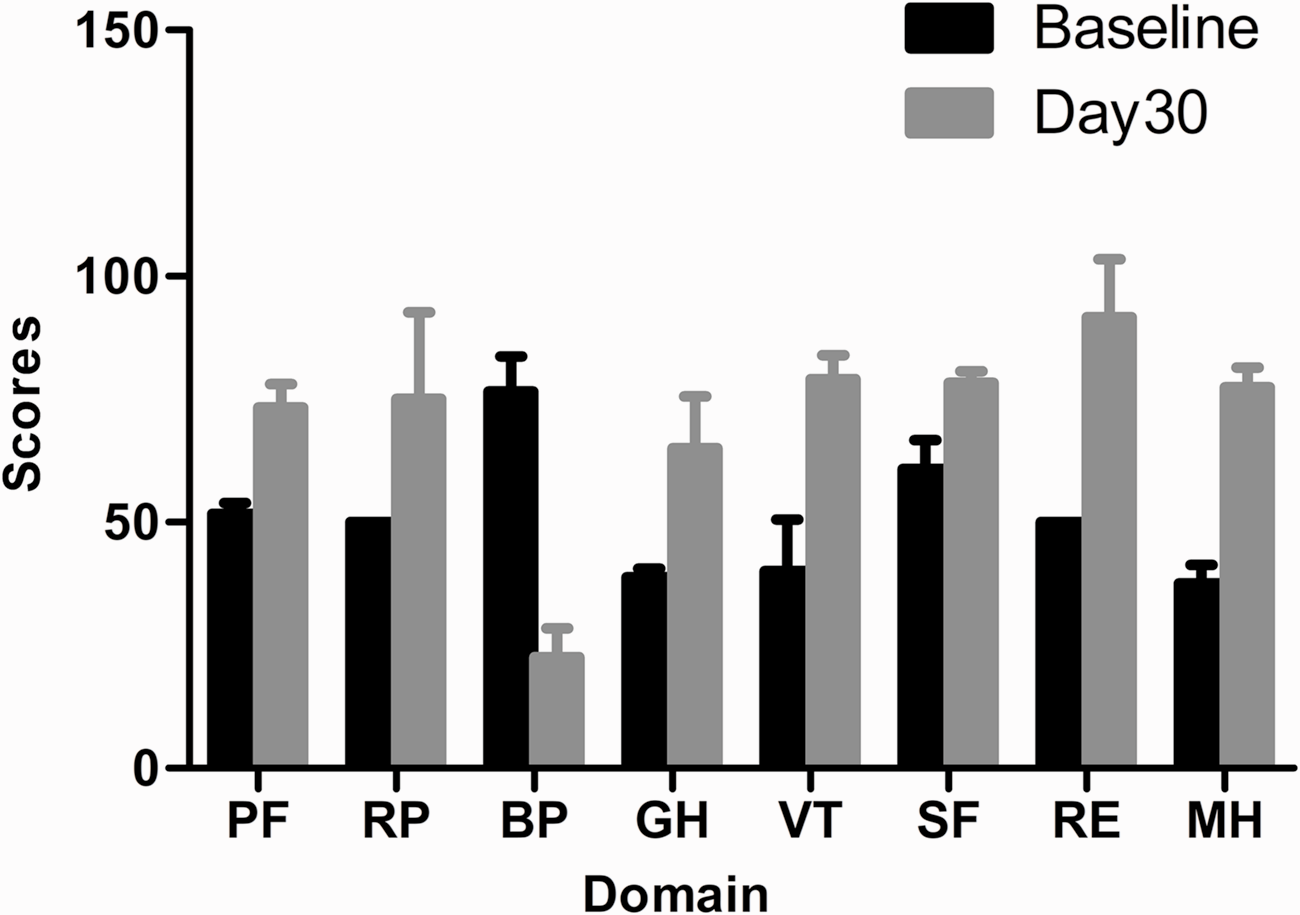
Assessment of health-related quality of life in two patients with painful diabetic neuropathy at baseline and at 30 days after undergoing lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion. Data presented as mean ± SD. PF, physical functioning; RP, physical role functioning; BP, bodily pain; GH, general health perceptions; VT, vitality; SF, social role functioning; RE, emotional role functioning; MH, mental health.
Discussion
The management of painful DN is challenging. No effective therapies exist that reverse the pathological course of DN. DN not only impacts on quality of life and prevents patients from going to work, but it may also reduce their life expectancy. 10 There is general consensus that controlling the symptoms of pain is an important issue in the management of DN. Most recommendations suggest that medical therapies should be used as the first step in treating pain. 11 Agents such as pregabalin, gabapentin, tricyclic and tetracyclic antidepressants, selective serotonin reuptake inhibitors and analgesics have been widely used to relieve pain. 12 Notably, the goal of medical therapies is to reduce but not eliminate pain. However, research has shown that medical therapies are limited in their ability to control pain. 13 The long-term benefits of medical therapies are uncertain due to their various side-effects.14,15
As an interventional strategy, lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion was used to alleviate pain in the two cases described in this current report. This technique was an effective treatment for neuropathic pain in two patients with DN. This therapy not only reduced the dosage of tramadol used each day, but it also relieved pain and improved the health-related quality of life. One patient discontinued tramadol and the other used only 50 mg per day after therapy. On analysing the VAS scores in the two patients, there was an improvement in pain scores at day 1 day after therapy. Although the pain recurred on days 3 and 5 for no obvious reason, the positive effect was sustained until day 30 after therapy. Health-related quality of life as assessed by the SF-36 questionnaire was improved in patients with DN compared with baseline.
The mechanisms underlying the positive effects of lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion remain elusive. Metabolic disorders including chronic hyperglycaemia, dyslipidaemia, visceral adiposity and hypertension are the primary cause of diabetic neuropathy.16–19 In the early stage of diabetes, the increased levels of glucose and fructose can lead to the generation of reactive oxygen species and increase the production of sorbitol, generating osmotic stress that can lead to not only oxidative stress, but also Schwann cell damage and nerve fibre degeneration.20,21 When cells are exposed to abnormal metabolic conditions, neural Na+/K+-ATPase activity is decreased, resulting in the impairment of impulse conduction and nerve dysfunction. 22 With time, hyperalgesia and allodynia can occur. 11 Small thinly myelinated Aδ fibers and unmyelinated C fibers are injured. 13 Axonopathy, demyelination, nerve degeneration and hypoalgesia exist in patients with blood glucose abnormalities. 23
Lumbar sympathetic pulsed radiofrequency might relieve pain via plastic change of the central pain pathway. 24 Previous research has demonstrated that the inflammatory process could be inhibited by electric fields that reduce cytokine release. 25 Electric fields could lead to pathway changes, such as the descending noradrenergic and serotonergic inhibitory pathways, which are known to be associated with the process of DN. 23 Continuous epidural infusion can facilitate the direct penetration of the local anaesthetic into the spinal nerve. The local anaesthetic (2% lidocaine) may decrease neuronal inflammation, exerting a membrane stabilizing effect on C fiber transmission, resulting in pain relief. 24
As for the complications associated with lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion, it is reported that the rate of spinal epidural abscesses varies from 18% to 54% due to diabetes mellitus. 25 Other complications, such as catheter dislodgement, infection and leakage are thought to be associated with continuous epidural infusion. 26 However, no complications occurred in the two cases presented in this report. Notably, glucose control was a key issue. Optimized glycaemic control can not only reduce complications, but it can also improve pain. 10
There are several limitations of this case report. First, only two cases underwent lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion. Secondly, the follow-up duration was relatively short at 30 days. Future research will collect more data and design a randomized, double-blind clinical trial to assess the efficacy of this therapy. Thirdly, little information was known concerning lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion for managing DN. There are no effective measures to monitor the changes and signs of lumbar nerve root block in the presence of DN. Therefore, future studies that examine the efficacy of this therapy will need to identify reliable ways to test the changes in the lumbar nerve root block. Finally, the lumbar sympathetic pulsed radiofrequency was performed at the same time as the epidural infusion, so it was impossible to determine whether it was the lumbar sympathetic pulsed radiofrequency or the epidural infusion that had the positive effect on pain. A previous study demonstrated that continuous epidural analgesia could relieve the acute pain due to herpes zoster. 7 Lumbar sympathetic pulsed radiofrequency was helpful in making a diagnosis and managing pain in a patient with primary erythromelalgia of the lower extremities. 27 Unfortunately, these studies were also case reports, so data are limited.
In conclusion, lumbar sympathetic pulsed radiofrequency combined with continuous epidural infusion offered effective pain relief and improved health-related quality of life in two patients with DN. This treatment represents a new therapeutic approach for patients with DN and warrants further research.
Footnotes
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.