
Abstract
Study Design
Retrospective study.
Objective
Hyperlipidemia (HL) and hypertension (HT) lead to systemic atherosclerosis. Not only atherosclerosis but also bone fragility and/or low bone mineral density result from diabetes mellitus (DM) and chronic kidney disease (CKD). The purpose of this study was to examine whether these lifestyle-related diseases affected surgical outcomes after posterior lumbar interbody fusion (PLIF).
Methods
The subjects comprised 122 consecutive patients who underwent single-level PLIF for degenerative lumbar spinal disorders. The clinical results were assessed using the Japanese Orthopaedic Association (JOA) score before surgery and at 2 years postoperatively. The fusion status was graded as union in situ, collapsed union, or nonunion at 2 years after surgery. The abdominal aorta calcification (AAC) score was assessed using preoperative lateral radiographs of the lumbar spine.
Results
HL did not significantly affect the JOA score recovery rate. On the other hand, HT and CKD (stage 3 to 4) had a significant adverse effect on the recovery rate. The recovery rate was also lower in the DM group than in the non-DM group, but the difference was not significant. The AAC score was negatively correlated with the JOA score recovery rate. The fusion status was not significantly affected by HL, HT, DM, or CKD; however, the AAC score was significantly higher in the collapsed union and nonunion group than in the union in situ group.
Conclusions
At 2 years after PLIF, the presence of HT, CKD, and AAC was associated with significantly worse clinical outcomes, and advanced AAC significantly affected fusion status.
Keywords
Introduction
Hyperlipidemia (HL) and hypertension (HT) lead to systemic atherosclerosis. Bone fragility and/or low bone mineral density, as well as systemic atherosclerosis, result from diabetes mellitus (DM) and chronic kidney disease (CKD). 1 , 2 Recently, a cross-sectional multicenter study revealed a close association between HT and DM in 50- to 69-year-old patients with lumbar spinal stenosis. 3 Impaired blood flow due to atherosclerosis can facilitate degeneration of the lumbar spine and the neural tissue. Therefore, these lifestyle-related diseases may affect both the clinical results and the fusion status after posterior lumbar interbody fusion (PLIF). Of these lifestyle-related diseases, some surgeons have studied the deleterious effect of DM on the outcomes following lumbar spine surgery. However, the results of their studies remain controversial. 4 , 5 , 6 , 7 Moreover, to the best of our knowledge there has been no report of a study evaluating the deleterious effects of HL, HT, and CKD on the outcomes after surgery for degenerative lumbar spinal disorders. Thus, the purpose of this study was to examine whether these lifestyle-related diseases affect clinical outcomes and fusion status after PLIF.
Materials and Methods
Patients
The subjects comprised 122 consecutive patients (49 men, 73 women; mean age at time of surgery, 69.3 years; age range, 20 to 86 years) who underwent single-level PLIF for unstable degenerative lumbar spinal disorders between May 2009 and June 2011 and were followed for ≥2 years. Patients with rheumatoid arthritis and/or CKD stage 5 needing hemodialysis were excluded from this study. Etiologies of degenerative lumbar spinal disorders were as follows: degenerative lumbar spondylolisthesis in 90 patients; lumbar spinal stenosis in 19; isthmic spondylolisthesis in 12; and lumbar disk herniation in 1. Fused areas were as follows: L4 to L5 in 90 patients; L3 to L4 in 14; L5 to S1 in 12; L5 to L6 in 3; L2 to L3 in 2; and L1 to L2 in 1. All patients were considered for surgery due to unresponsiveness to conservative treatment such as medication and/or epidural block. Preoperative comorbidities were HL in 26 patients, DM in 31, HT in 55, and CKD (stage 3 to 4) in 39. None of the 122 patients in this study had severe obesity (body mass index [BMI] ≥30). The protocol was approved by the institutional review board of the hospital, and written informed consent was obtained from all participants.
Surgical Procedure
The PLIF procedure was performed using the Brantigan I/F cages (DePuy Spine, Inc., Raynham, Massachusetts, United States) filled with local bone graft from the lamina and spinous process and posterior instrumentation with pedicle screws. After the intervertebral disk material and cartilaginous end plates were removed, two cages were inserted into the intervertebral space, and local bone blocks were inserted lateral to the cages.
Clinical and Radiologic Evaluations
Medical records were examined by a single observer (H.S.). Clinical results were assessed using the Japanese Orthopaedic Association (JOA) scoring system for assessment of the results of treatment for low back pain before surgery and at 2-year postoperative follow-up. 8 In brief, the JOA score consists of the rating of subjective symptoms (low back pain, 3 points; leg pain, 3 points; and gait, 3 points), clinical signs (straight-leg-raising test, 2 points; sensory disturbance, 2 points; and motor disturbance, 2 points), restriction of activities of daily living (14 points), and urinary bladder function (minus 6 points). Thus, the total JOA score is 29 points in normal populations (Table 1).
Japanese Orthopaedic Association scoring system for assessing the results of treatment for low back pain
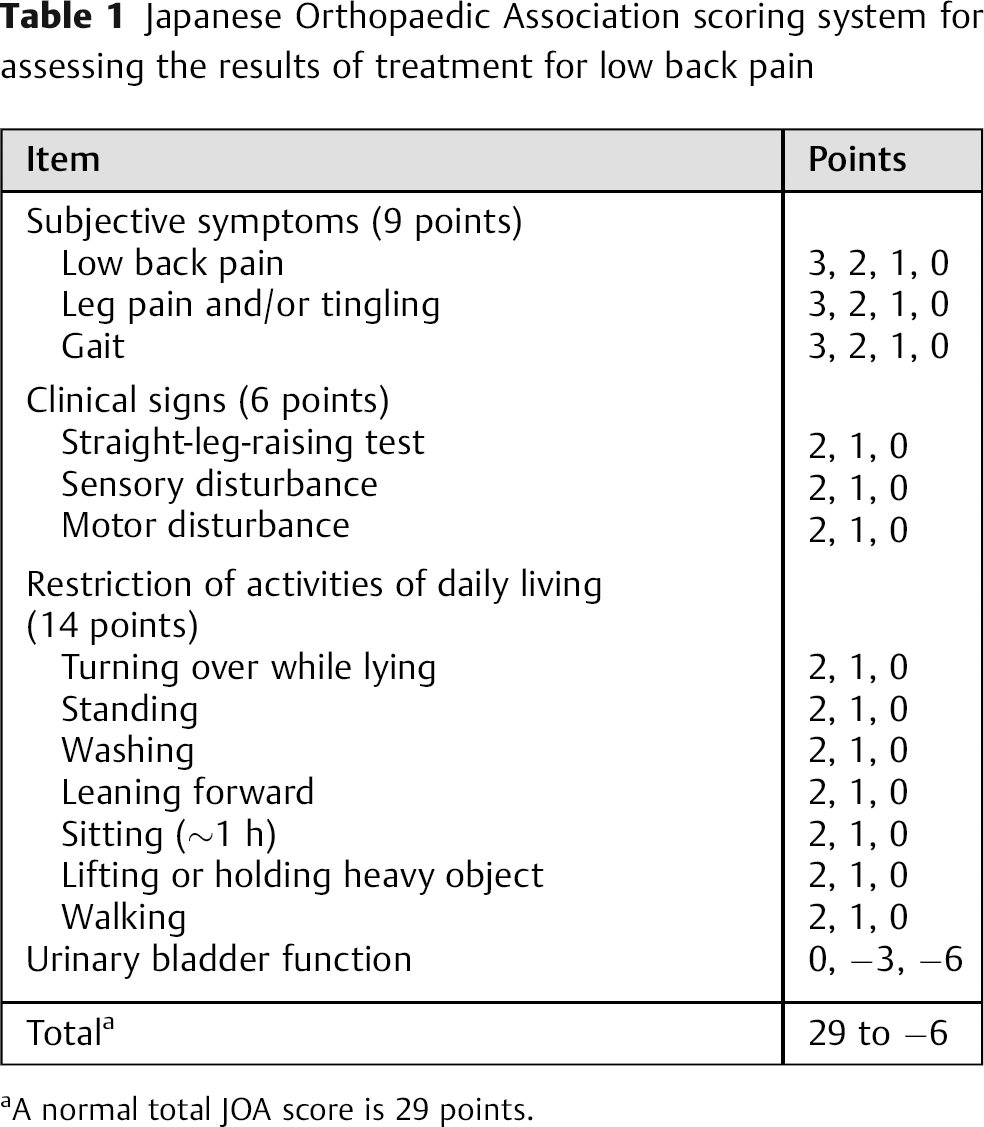
A normal total JOA score is 29 points.
The fusion status 2 years after surgery was graded as union in situ (a solid fusion without loss of graft height), collapsed union (graft bone collapse or cage subsidence into the adjacent vertebral body), or nonunion using multiplanar reconstruction computed tomography and dynamic lateral radiographs of the lumbar spine. 9
According to the scoring system by Kauppila et al, 10 atherosclerosis of the abdominal aorta (as a marker of systemic atherosclerosis and a predictor for low bone mineral density) was assessed using the preoperative lateral radiographs of the lumbar spine. Briefly, the calcified deposits in the lumbar aorta adjacent to each lumbar vertebral segment (L1 to L4) were assessed separately for the anterior and posterior walls of the aorta. Each wall at each segment was graded for the presence of calcified deposits with a score from 0 to 3 points (0 point: no deposits; 1 point: less than one-third of the aortic wall length covered with calcified deposits; 2 points: one-third or more to less than two-thirds of the aortic wall length covered with deposits; 3 points: more than two-thirds of the aortic wall length covered with deposits). The sum of the scores at each segment both for the anterior and posterior walls was taken as the abdominal aorta calcification (AAC) score. Thus, the maximum possible AAC score was 3 (0 to 3 points) × 2 (anterior and posterior walls) × 4 (L1 to L4 segments) = 24 points.
Statistical Analysis
The Mann-Whitney U test and Spearman rank correlation were used for statistical analysis with JMP 5.0.1 software (SAS Institute, Cary, North Carolina, United States), as appropriate. Values of p < 0.05 were considered significant.
Results
Clinical Results
HL, DM, HT, and CKD (stage 3 to 4) had no significant deleterious effects on the preoperative JOA score (Tables 2 to 5). HL did not significantly affect the JOA score at 2 years postoperatively or its recovery rate (Table 2). On the other hand, the JOA score at 2 years after surgery and its recovery rate were lower in the DM group than in the non-DM group; however, the differences between the two groups were not significant (JOA score at 2 years after surgery, p = 0.067; JOA score recovery rate, p = 0.18; Table 3). HT had significant deleterious effects on the JOA score at 2 years postoperatively and on its recovery rate (Table 4). CKD also had significant deleterious effects on the JOA score at 2-year follow-up and on its recovery rate (Table 5).
Clinical outcomes in patients with or without hyperlipidemia

Abbreviations: JOA, Japanese Orthopaedic Association; SD, standard deviation.
Clinical outcomes in patients with or without diabetes mellitus

Abbreviations: JOA, Japanese Orthopaedic Association; SD, standard deviation.
Clinical outcomes in patients with or without hypertension
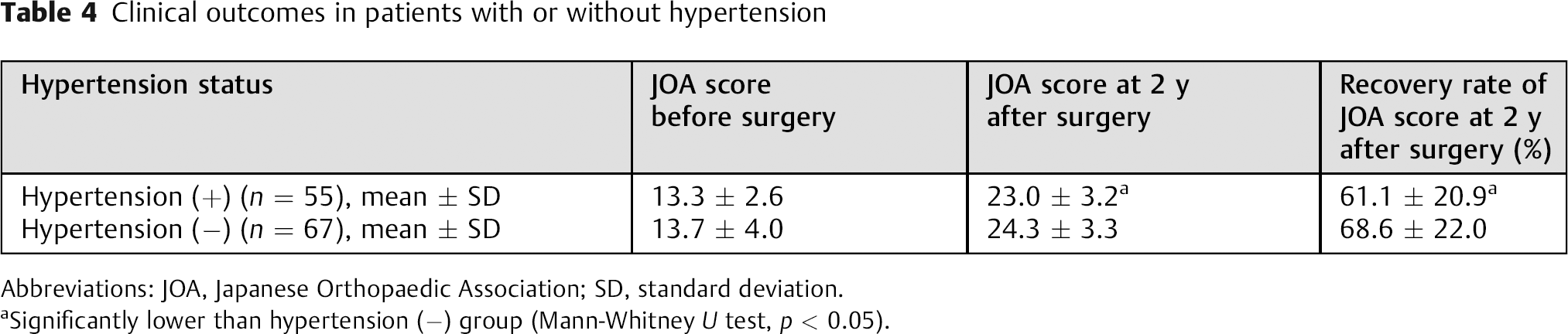
Abbreviations: JOA, Japanese Orthopaedic Association; SD, standard deviation.
Significantly lower than hypertension (−) group (Mann-Whitney U test, p < 0.05).
Clinical outcomes in patients with or without chronic kidney disease
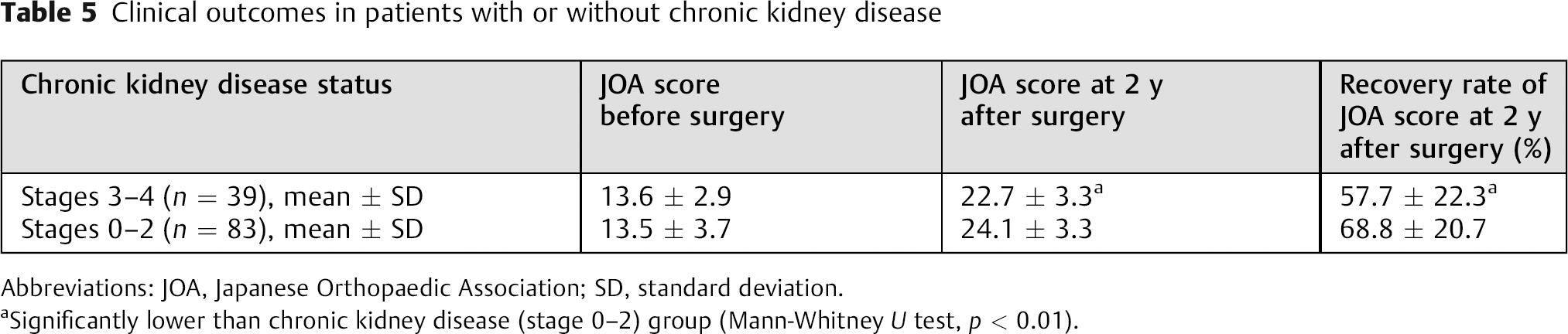
Abbreviations: JOA, Japanese Orthopaedic Association; SD, standard deviation.
Significantly lower than chronic kidney disease (stage 0–2) group (Mann-Whitney U test, p < 0.01).
The AAC score had relatively weak but significant negative correlations with the preoperative JOA score (p = 0.002, r = − 0.261), the JOA score at 2 years after surgery (p = 0.0001, r = − 0.321), and the JOA score recovery rate (p = 0.001, r = − 0.279; Figs. 1 2 to 3).
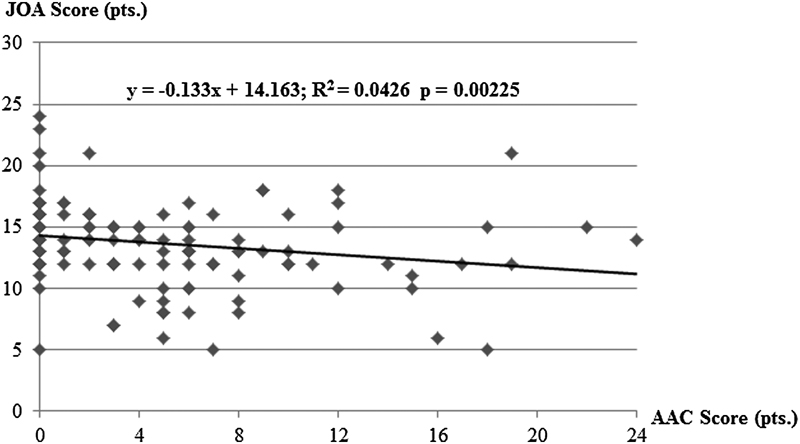
Correlation between the abdominal aorta calcification (AAC) score and the Japanese Orthopaedic Association (JOA) score before surgery. The preoperative AAC score has a relatively weak but significant negative correlation with the preoperative JOA score.
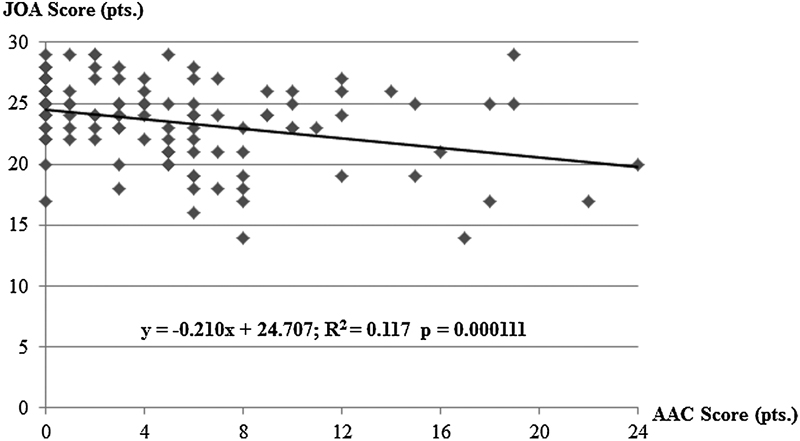
Correlation between the abdominal aorta calcification (AAC) score and the Japanese Orthopaedic Association (JOA) score at 2 years after surgery. The AAC score before surgery has a relatively weak but significant negative correlation with the JOA score at 2-year follow-up.
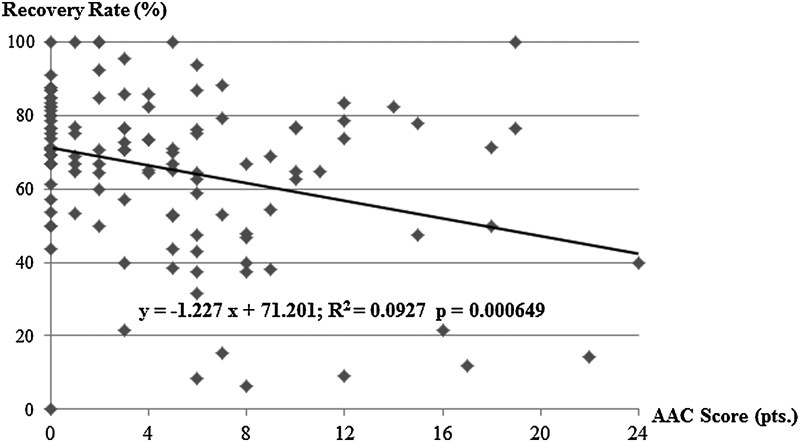
Correlation between the abdominal aorta calcification (AAC) score and the recovery rate of the Japanese Orthopaedic Association (JOA) score at 2 years after surgery. The preoperative AAC score has a relatively weak but significant negative correlation with the recovery rate of the JOA score at 2 years postoperatively.
Fusion Status
At 2-year follow-up, 64 patients achieved union in situ, and collapsed fusion occurred in 48 patients. Nonunion was found in 10 patients. Thus, 112 (91.8%) of the 122 patients achieved solid spinal fusion. The fusion status was not significantly affected by HL, DM, HT, or CKD; however, the AAC score was significantly higher in the collapsed union and nonunion group than in the union in situ group (Table 6).
Abdominal aorta calcification score and fusion status
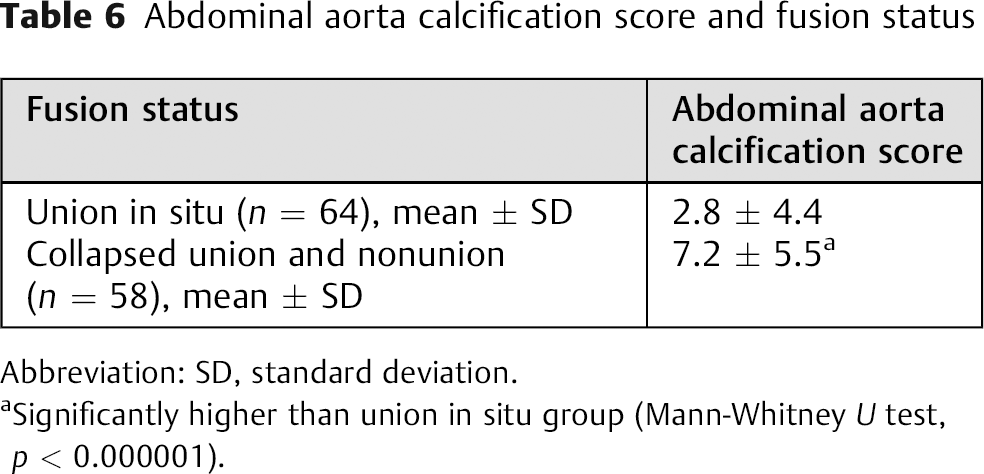
Abbreviation: SD, standard deviation.
Significantly higher than union in situ group (Mann-Whitney U test, p < 0.000001).
Surgery-Related Complications
Surgery-related complications occurred in 14 patients (11.5%). Transient radicular pain occurred in 6 patients (4.9%) whose leg pain had been alleviated with oral medication. Transient motor weakness occurred in 1 patient (0.8%); this patient developed mild motor weakness of the left tibialis anterior just after surgery, and her mild paralysis had recovered fully with rehabilitation by 3 postoperative months. Delayed wound healing was noted in 1 patient (0.8%) whose wound successfully healed with debridement and resuture by 3 weeks after surgery. Four patients (3.3%) required revision surgery for evacuation of an epidural hematoma after the initial surgery. Two patients (1.6%) developed a deep wound infection; both patients were successfully treated with debridement and irrigation without removal of the implants. However, surgery-related complications were not significantly affected by HL, DM, HT, or CKD.
Discussion
Clinical Outcomes
A recent cross-sectional multicenter study revealed a close association between HT and DM in 50- to 69-year-old patients with lumbar spinal stenosis. 3 Regarding effects of lifestyle-related diseases on surgical outcomes for lumbar degenerative diseases, there have been some reports concerning a deleterious effect of DM on the outcomes following lumbar spine surgery; however, the results of the studies remain controversial. Some surgeons reported that clinical results after surgical decompression for lumbar spinal stenosis and/or lumbar disk disease were poorer in patients with DM than in patients without DM. 4 , 7 Others reported that the clinical outcomes after decompression surgery or posterolateral fusion with instrumentation were similar in the DM and non-DM groups. 5 , 6 Moreover, to the best of our knowledge, there has been no report of a study evaluating the deleterious effects of HL, HT, and CKD on the outcomes after surgery for degenerative lumbar spinal disorders. In the present study, HT and CKD had significant deleterious effects on the JOA score at 2 years after PLIF and on the JOA score recovery rate. The JOA score at 2 years after PLIF and its recovery rate were lower in the DM group than in the non-DM group, although the differences between the two groups were not significant.
Systemic atherosclerosis results from DM, HT, and CKD. Impaired blood flow due to atherosclerosis can facilitate the degeneration of the lumbar spine and the neural tissue. In fact, in the present study, the AAC score had relatively weak but significant negative correlations with the preoperative JOA score, the JOA score at 2 years after PLIF, and the JOA score recovery rate. The AAC score is a significant surrogate marker of systemic atherosclerosis. 11 In addition, clinical studies have shown that AAC was associated with both low back pain and lumbar intervertebral disk degeneration. 12 Taken together, it appears that advanced systemic atherosclerosis resulting from these lifestyle-related diseases may lead to poor clinical recovery after PLIF for degenerative lumbar spinal disorders.
In association with these lifestyle-related diseases, severe obesity (BMI ≥30) has been reported as a poor prognostic factor for outcomes after surgery for degenerative spondylolisthesis. 13 However, there were no severely obese patients with BMI ≥30 in this study. Therefore, we did not add obesity (BMI ≥30) as a separate analysis.
Fusion Status
The vertebral fracture risk is increased in patients with DM because their bone fragility is related to bone-quality deterioration. 1 CKD is associated with unique metabolic mineral disorders related to low bone mineral density and increased fracture risk 2 ; therefore, we hypothesized that these lifestyle-related diseases may affect fusion status after PLIF. However, in the present study, HL, DM, HT and CKD did not significantly affect fusion status, but the AAC score, a significant surrogate marker of systemic atherosclerosis, was significantly higher in the collapsed union and nonunion group than in the union in situ group. The AAC was reportedly inversely related to bone mineral density and directly related to fractures not only at the hip but also at the thoracolumbar spine. 14 , 15 Thus, these results suggest that atherosclerosis of the abdominal aorta resulting from lifestyle-related diseases such as HL, DM, HT, and CKD may affect fusion status after PLIF.
There are several limitations in this retrospective study. The first is that the number of patients was relatively small. The second is that some patients had multiple lifestyle-related diseases, whereas others had only one or none of them. The third is that smoking history, which is a significant risk factor for systemic atherosclerosis, was unclear. Therefore, a future study in a larger patient population is needed to precisely analyze which lifestyle-related disease or whether a confounder such as smoking history is an independent risk factor for poor surgical outcomes after PLIF using the multivariate analysis.
In conclusion, the presence of HT and CKD was significantly associated with worse JOA scores at 2 years after PLIF and a worse JOA score recovery rate. The JOA score at 2 years after PLIF and its recovery rate were lower in the DM group than in the non-DM group, although the differences between the two groups were not significant. The AAC score had relatively weak but significant negative correlations with the preoperative JOA score, the JOA score at 2 years after PLIF, and the JOA score recovery rate, and advanced AAC significantly affected fusion status. As prognostic factors of PLIF, systemic atherosclerosis resulting from these lifestyle-related diseases should be kept in mind and explained to the patient during the process of obtaining informed consent.
Disclosures
Hironobu Sakaura, none
Toshitada Miwa, none
Tomoya Yamashita, none
Yusuke Kuroda, none
Tetsuo Ohwada, none