
Abstract
Introduction
Options for treating two-level symptomatic disc degeneration after failure of nonoperative care includes fusion, total disc replacement (TDR), or a hybrid with fusion at one level and TDR at the other. Often the hybrid procedure involved an instrumented 360 fusion. However, the option for a standalone ALIF in a hybrid has rarely been addressed. The purpose of this study was to compare the outcomes of hybrid TDR/fusion surgery for ALIF versus 360 at the fusion level.
Methods
The study group included 135 patients undergoing hybrid surgery using TDR at one level and either ALIF (n = 83) or instrumented 360 fusion (n = 52) at the adjacent segment. The majority of cases were performed with TDR at L4–L5 and fusion at L5–S1. Only patients who had surgery at least 12 months before this study were included. The mean length of follow-up was similar in the two groups (∼24 months in both groups). Outcome measures included Oswestry Disability Index (ODI), visual analog scales (VAS) assessing back and leg pain, and reoperations.
Results
The mean operative blood loss was significantly less in the hybrid/ALIF group compared with the hybrid/360 group (71.7 vs. 142.1 mL; p < 0.01). The mean ODI scores before surgery were approximately 46 in both the groups. The scores improved significantly in both groups to the means of about 30 (p < 0.01) with no significant difference between the two groups (p > 0.40). Mean VAS back and leg pain scores also improved significantly in both groups with no significant differences between groups (Fig. 1).
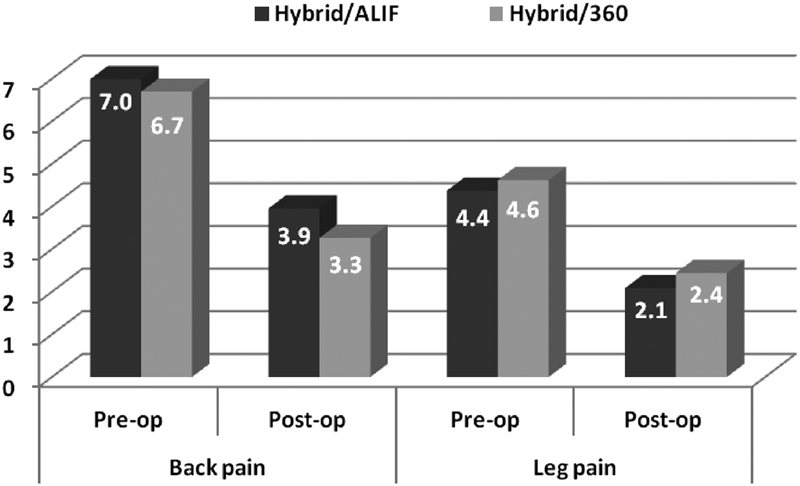
Mean VAS back and leg pain scores improved in both groups (p < 0.01) with no significant differences between groups. post-op, postoperative; pre-op, preoperative; VAS, visual analog scales.
The reoperation rate was significantly greater in the hybrid/360 group than in the hybrid/ALIF group (23.1 vs. 3.6%; p < 0.01). Reoperations in the hybrid/360 group included six reoperations for removal of painful posterior instrumentation, one to treat a wound infection, one decompression of the fusion level of the hybrid, three were for treatment of a symptomatic adjacent segment, and two were due to TDR malpositioning or displacement. Hybrid/ALIF reoperations included two patients undergoing decompression for stenosis and one underwent fusion two levels above the index surgery.
Discussion
This study found that the outcomes are similar between hybrids performed with ALIF versus 360 fusion adjacent to the TDR level with the exceptions of a significantly greater reoperation rate and mean blood loss in the hybrid/360 group. These results support that unless there is a defined indication for the posterior procedure, standalone ALIF is a viable option for lumbar hybrid surgery.