
Abstract
Study Design
Systematic review.
Clinical Questions
(1) Is autologous local bone (LB) graft as safe and effective as iliac crest bone graft (ICBG) in lumbar spine fusion? (2) In lumbar fusion using ICBG, does a single-incision midline approach reduce postoperative iliac crest pain compared with a two-incision traditional approach?
Methods
Electronic databases and reference lists of key articles were searched up to October 2014 to identify studies reporting the comparative efficacy and safety of ICBG versus LB graft or comparing ICBG harvest site for use in lumbar spine surgery. Studies including allograft, synthetic bone, or growth factors in addition to ICBG and those with less than 80% of patients with degenerative disease in the lumbar spine were excluded. Two independent reviewers assessed the level of the evidence quality using the Grades of Recommendation Assessment, Development and Evaluation criteria, and disagreements were resolved by consensus.
Results
Seven studies were identified as using ICBG fusion for degenerative disease in the lumbar spine. There were no differences in the fusion, leg pain, low back pain, or functional outcomes between patients receiving LB versus ICBG. There was a higher incidence of donor site pain and sensory loss in patients receiving ICBG, with no donor site complications attributed to LB. Compared with patients with the graft harvested through the two-incision traditional approach, patients with the graft harvested through the single-incision midline approach had lower mean pain scores over the iliac crest, with a higher proportion reporting no iliac crest tenderness. In patients with ICBG harvested through the single-incision midline approach on either the right or the left side of the ilium, only 36% of the patients were able to correctly identify the side when asked whether they knew which iliac crest was harvested. Only 19% of the patients with ICBG harvested through the single-incision midline approach on either the right or the left side of the ilium reported pain that was concordant with the side that was actually harvested.
Conclusions
LB is as safe and efficacious as ICBG for instrumented fusion in the lumbar spine to treat degenerative disease. When ICBG is used, graft harvest through the single-incision midline approach reduces postoperative iliac crest pain compared with a two-incision approach.
Study Rationale and Context
Solid bone fusion is the primary goal of all fusion procedures for lumbar degenerative disease. Autologous iliac crest bone has long been considered the gold standard for these fusion procedures. However, there are recognized drawbacks to depending on iliac crest bone graft (ICBG), including increased operative time, increased blood loss, increased donor site morbidity, and a limitation to the amount that can be realistically harvested for multilevel fusion. There are alternatives for “expanding” the amount of ICBG including aspiration systems; however, this option potentially substantially increases the cost of these procedures and the aspirations are not as enriched with osteoinductive elements as harvested iliac crest marrow. The other readily available autologous bone source in these fusion procedures is local bone (LB) graft harvested at the time of decompression, which is often referred to as “bad bone” by many surgeons compared with the “good bone” of ICBG. However, there is growing interest and supportive evidence for the utilization of LB alone or in combination with ICBG or other bone extenders as the primary fusion substrate, which is especially true for shorter segment fusions; the practice requires efficient harvest of all available LB as opposed to using the drill primarily for the decompression. It also involves a meticulous preparation of the harvested bone including removal of soft tissue elements and morselization to increase the surface area for fusion. In addition, regardless of the fusion substrate, there is no substitution for meticulous preparation of the fusion bed before placement of the fusion substrate. The first systemic review question is designed to address the utilization of LB graft compared with ICBG.
When the decision is made to use ICBG, there are numerous methods described to reduce donor site morbidity, including persistent pain, which is a major concern. One of the fundamental questions is whether to harvest the crest through the same midline incision used for the primary procedure or to use a separate incision. There are advocates and arguments for both procedures including cosmesis, fewer incisions (same incision), less soft tissue undermining and dead space, and better closure of the fascia overlying the crest (separate incisions). The second systemic review question is designed to address these issues.
Clinical Questions
Is autologous LB graft as safe and effective as ICBG in lumbar spine fusion?
In lumbar fusion using ICBG, does a single-incision midline approach reduce postoperative iliac crest pain compared with a two-incision traditional approach?
Materials and Methods
Details about methods can be found in the online supplementary material.
Results
We identified seven comparative studies that met the inclusion criteria (Fig. 1). A list of excluded studies can be found in the online supplementary material.
Three studies compared fusion for degenerative disease in the lumbar spine with either autologous LB or autologous ICBG, one randomized controlled trial (RCT) 2 and two retrospective cohorts 3 , 4 , 5 (Table 1).
Four studies, one RCT 6 and three retrospective cohorts, 7 , 8 , 9 evaluated the origin of donor site morbidity in the lumbar spine using autologous ICBG. Of these, two studies compared the single-incision midline approach with the two-incision traditional approach. 6 , 7 The other two studies evaluated whether patients were able to correctly identify the side of harvest site based on pain (Table 2). 8 , 9
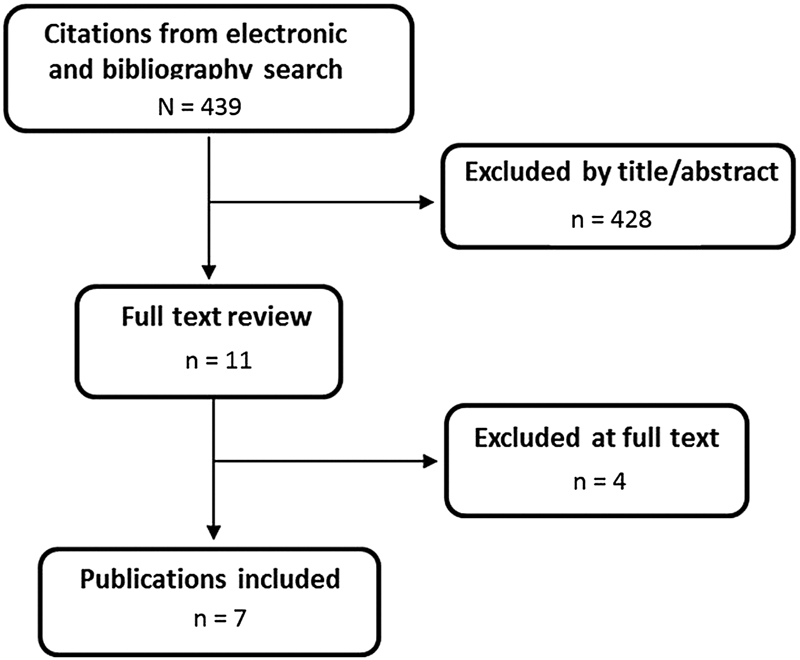
Flowchart showing results of literature search.
Characteristics of included studies using ICBG versus LB for question 1 (Is autologous LB graft as safe and effective as ICBG in lumbar spine fusion?)
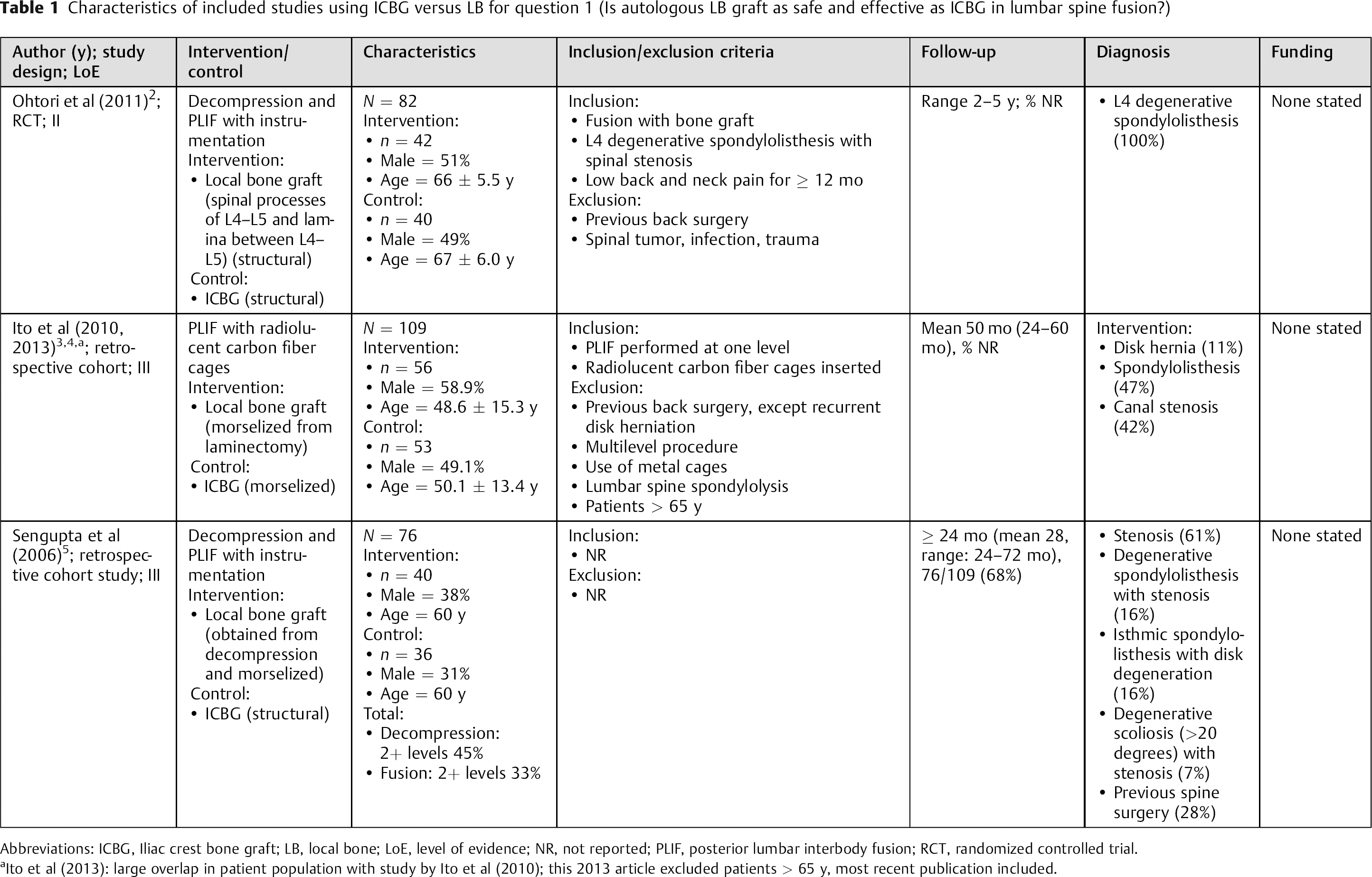
Abbreviations: ICBG, Iliac crest bone graft; LB, local bone; LoE, level of evidence; NR, not reported; PLIF, posterior lumbar interbody fusion; RCT, randomized controlled trial.
Ito et al (2013): large overlap in patient population with study by Ito et al (2010); this 2013 article excluded patients > 65 y, most recent publication included.
Characteristics of included studies using ICBG for question 2 (In lumbar fusion using ICBG, does a single-incision midline approach reduce postoperative iliac crest pain compared with a two-incision traditional approach?)
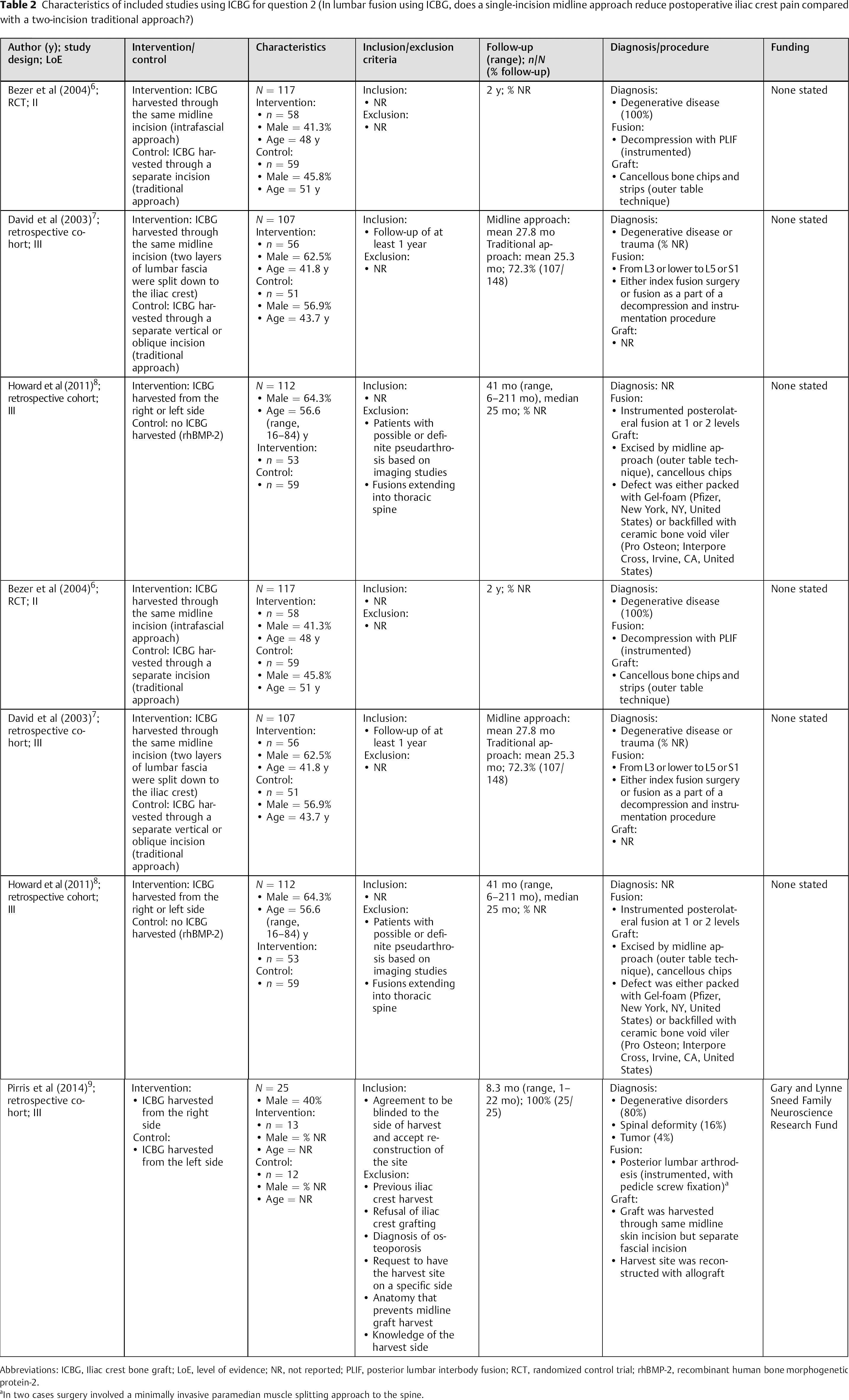
Abbreviations: ICBG, Iliac crest bone graft; LoE, level of evidence; NR, not reported; PLIF, posterior lumbar interbody fusion; RCT, randomized control trial; rhBMP-2, recombinant human bone morphogenetic protein-2.
In two cases surgery involved a minimally invasive paramedian muscle splitting approach to the spine.
Local Bone versus Iliac Crest Bone Graft for Fusion in the Lumbar Spine
There were no differences in fusion, leg pain, low back pain, or functional outcomes between the patients receiving LB or ICBG in one RCT and two retrospective cohorts (Table 3). 2 , 4 , 5
In the patients receiving LB versus ICBG, there was a higher incidence of donor site pain (0 versus 15%, respectively, p = 0.025) and sensory loss (0 versus 20%, respectively, p = 0.01) (Table 4). 2 , 4 , 5
There were no donor site complications attributed to LB grafting (Table 4). 4 , 5
There were no differences between the treatment groups with respect to complications not related to the donor site, such as infection, dural tears, pedicle screw misplacement, or instrumentation failure (Table 5). 2 , 4 , 5
Fusion, pain, and patient-reported outcomes following lumbar fusion with local bone compared with iliac crest bone graft
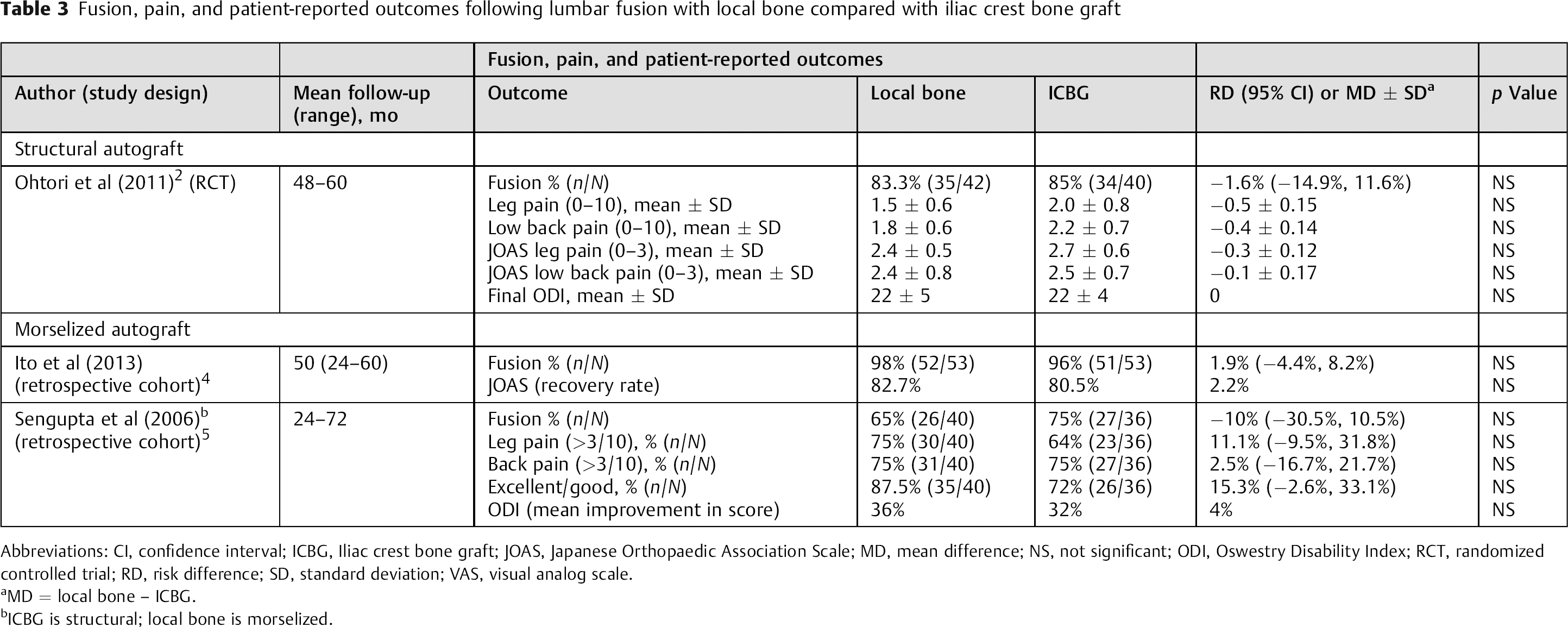
Abbreviations: CI, confidence interval; ICBG, Iliac crest bone graft; JOAS, Japanese Orthopaedic Association Scale; MD, mean difference; NS, not significant; ODI, Oswestry Disability Index; RCT, randomized controlled trial; RD, risk difference; SD, standard deviation; VAS, visual analog scale.
MD = local bone – ICBG.
ICBG is structural; local bone is morselized.
Donor site complications at final follow-up comparing local bone graft with ICBG
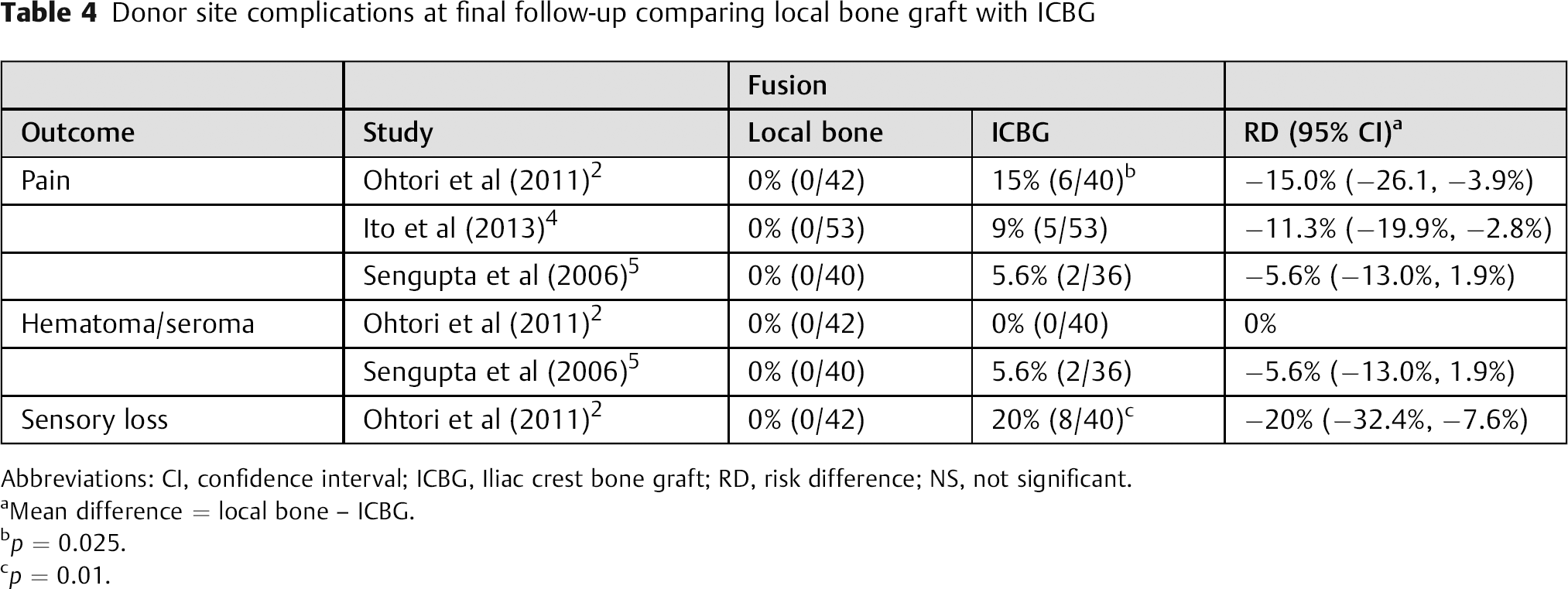
Abbreviations: CI, confidence interval; ICBG, Iliac crest bone graft; RD, risk difference; NS, not significant.
Mean difference = local bone – ICBG.
p = 0.025.
p = 0.01.
Other complications (other than donor site complications) at final follow-up comparing local bone graft with ICBG in lumbar fusion: non-ICBG autograft versus ICBG
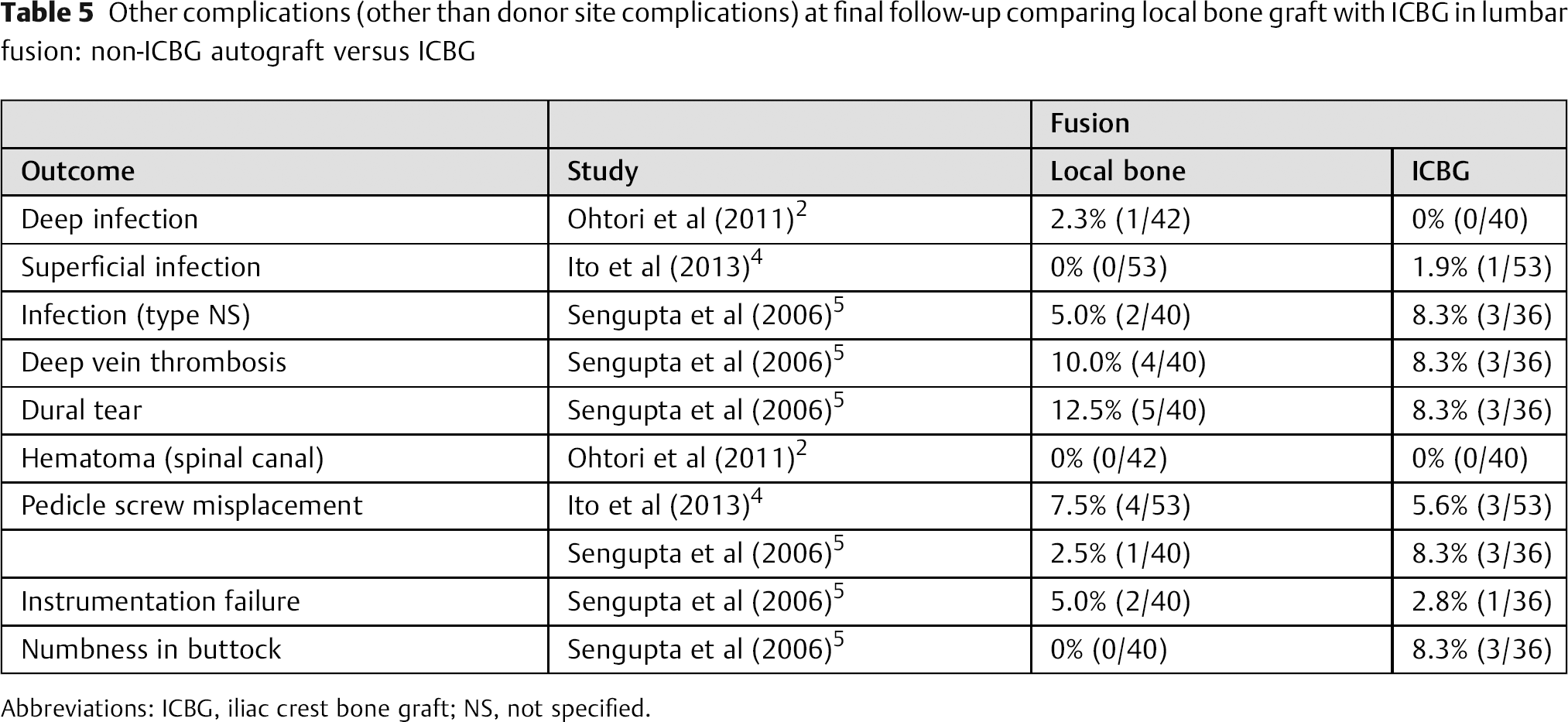
Abbreviations: ICBG, iliac crest bone graft; NS, not specified.
Origin of Graft Site Morbidity in Patients Receiving ICBG for Fusion in the Lumbar Spine
Midline versus Traditional Approach
Patients with graft harvested through the single-incision midline approach had lower mean pain scores over the iliac crest compared with those patients with graft harvested through the two-incision traditional approach (0.25 versus 2, respectively, p < 0.0001), 6 with a higher proportion reporting no iliac crest tenderness (82.1 versus, 45.1%, respectively; Figs. 2 and 3). 7
A higher proportion of the patients having grafts harvested through the single-incision midline approach were satisfied with the graft procedure and cosmesis than the patients with grafts harvested through the two-incision traditional approach (96.5 versus 81.3%, p < 0.5). 6
No statistical difference in complications (sacroiliac penetration, donor site pain > 1 year, residual donor site numbness, seroma, temporary sensory loss, donor site pain >30 days, reoperation, or surgical complications) was found between the single-incision midline approach and the two-incision traditional approach for graft harvest (Table 6).
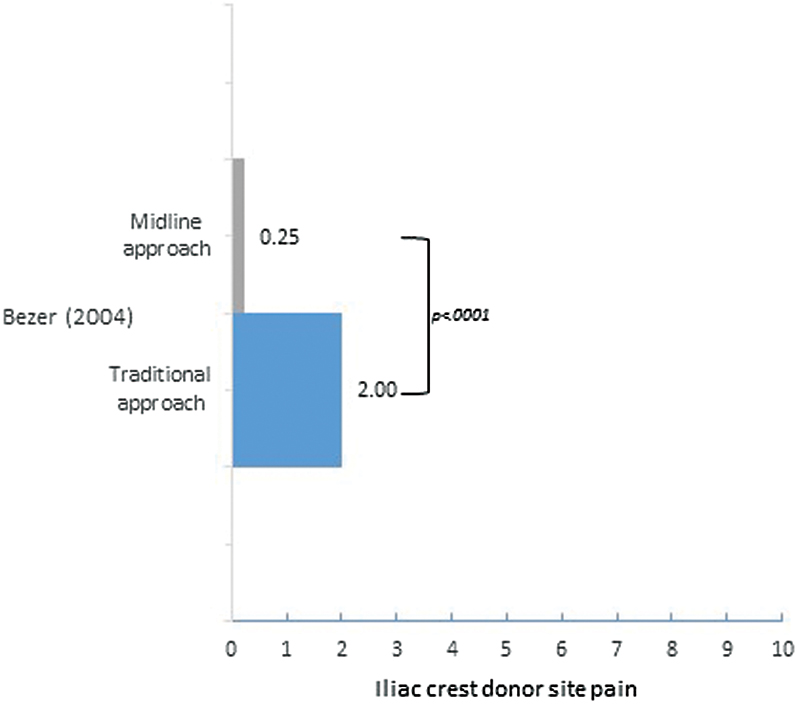
Mean pain level comparing a two-incision traditional approach with a single incision with a midline approach in one randomized controlled trial of patients receiving lumbar fusion. 6
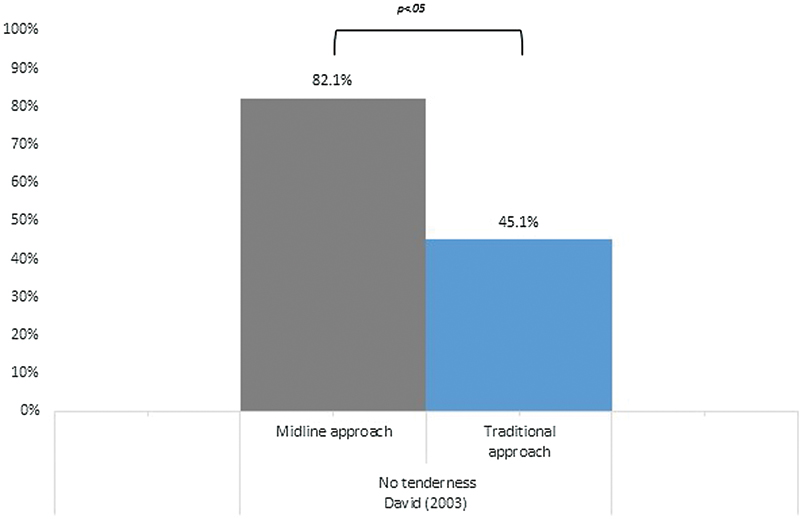
Proportion of patients with iliac crest tenderness reported by David et al. 7
Complications in included studies using ICBG for question 2

Abbreviation: ICBG, iliac crest bone graft.
Right versus Left Side Harvest Site
In the patients with ICBG harvested through the single-incision midline approach on either the right or the left side of the ilium, only 36% of the patients were able to correctly identify the side when asked whether they knew which iliac crest was harvested. Of these, only 8% had confidence in their answer (Fig. 4). 9
Only 19% of the patients with ICBG harvested through the single-incision midline approach on either the right or the left side of the ilium reported pain that was concordant with the side that was actually harvested (i.e., right side harvest site, right side pain reported; Fig. 4). 8
When comparing patients receiving lumbar fusion without ICBG (rhBMP-2 used) with the patients with ICBG harvested through the single-incision midline approach, there was no difference in the proportion of patients reporting pain or tenderness (50.8 versus 56.6%, respectively; Fig. 4). 8
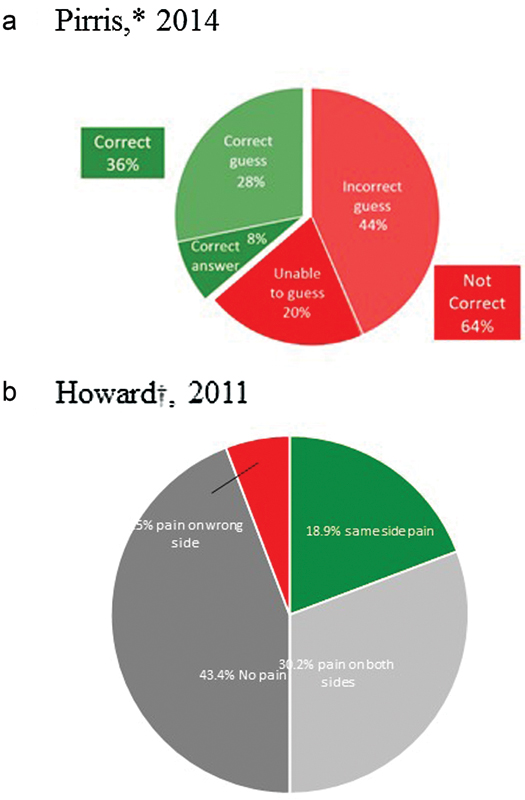
Percentage of patients correctly identifying side of harvest site based on pain. Patients were asked to guess from which side of the pelvis (left or right) the iliac crest bone graft was taken. 9
Clinical Guidelines
None found.
Evidence Summary
There was no difference in effectiveness or safety in lumbar fusion comparing ICBG with LB grafts (Table 7). The strength of the evidence for this conclusion was very low.
There was less pain and tenderness over the iliac crest harvest site when a single-incision midline approach was used compared with a two-incision traditional approach in lumbar fusion (Table 8). The strength of evidence for this conclusion was very low.
Strength of evidence summary for question 1 (Is autologous local bone graft as safe and effective as ICBG in lumbar spine fusion?)
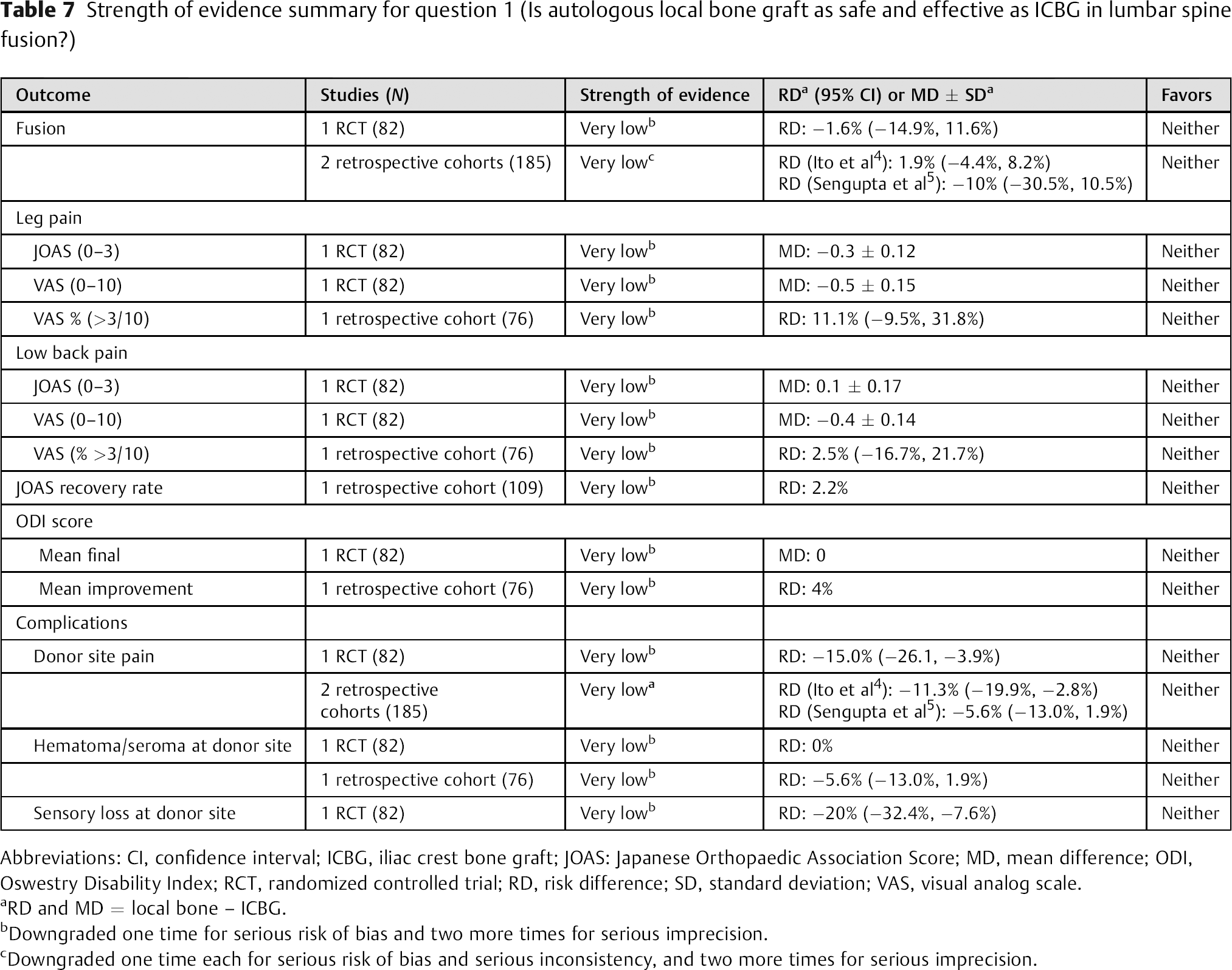
Abbreviations: CI, confidence interval; ICBG, iliac crest bone graft; JOAS: Japanese Orthopaedic Association Score; MD, mean difference; ODI, Oswestry Disability Index; RCT, randomized controlled trial; RD, risk difference; SD, standard deviation; VAS, visual analog scale.
RD and MD = local bone – ICBG.
Downgraded one time for serious risk of bias and two more times for serious imprecision.
Downgraded one time each for serious risk of bias and serious inconsistency, and two more times for serious imprecision.
Strength of evidence summary for question 2 (In lumbar fusion using iliac crest bone graft, does a single-incision midline approach reduce postoperative iliac crest pain compared with a two-incision traditional approach?)
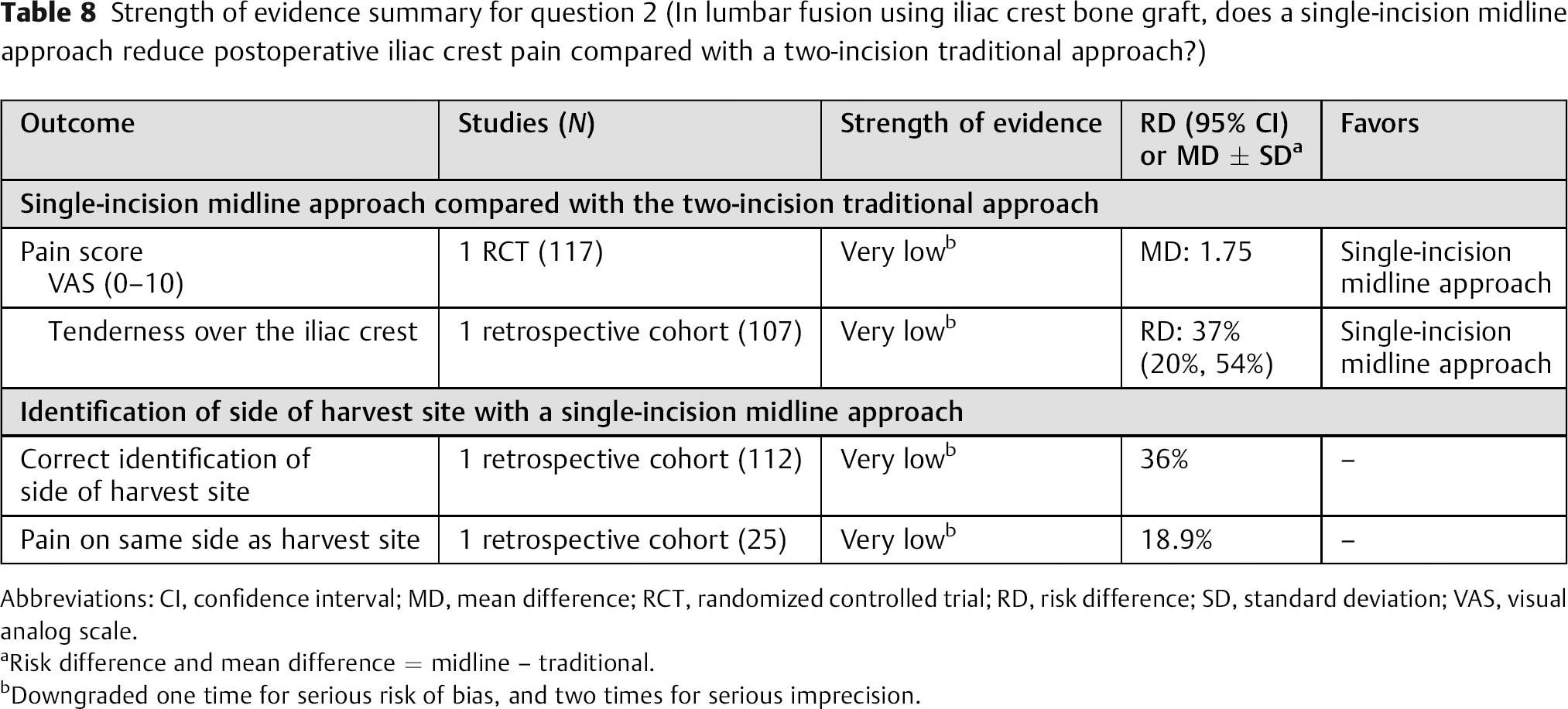
Abbreviations: CI, confidence interval; MD, mean difference; RCT, randomized controlled trial; RD, risk difference; SD, standard deviation; VAS, visual analog scale.
Risk difference and mean difference = midline – traditional.
Downgraded one time for serious risk of bias, and two times for serious imprecision.
Discussion
Question 1: Is Autologous Local Bone Graft as Safe and Effective as Iliac Crest Bone Graft in Lumbar Spine Fusion?
When patients do not improve after lumbar fusion, the question always becomes “Did we achieve adequate fusion?” Fusion cannot be completely evaluated radiographically and is not always associated with outcome, but continues to be our ultimate goal. The choices of fusion substrate are numerous but fiscal restraints and long-term efficacy/ safety studies would still argue that an autologous source would be ideal. We have tried to address the issue of safety and efficacy with autologous sources (local autograft versus ICBG) in the available literature. This issue is especially pertinent in shorter-segment fusions and fortunately the available studies that met the screening criteria all involved short-segment fusions for degenerative disease. Based on the available evidence, the LB graft is a reasonable alternative to ICBG for single-level instrumented fusions for lumbar degenerative disease at a very low evidence level.
Weaknesses of this study include that there were only three studies that met the criteria for inclusion, of which one was an RCT (level 2) and two were retrospective cohort studies (level 3). All of the studies used interbody fusion and posterior instrumentation, and so it is harder to extrapolate to posterolateral fusions in addition to instrumentation or noninstrumented fusions. The RCT had relatively small numbers and no report of percent follow-up. The two cohort studies had no percentage follow-up in one and 68% follow-up in the other. These factors contribute to a very low evidence level and suggest the need for larger controlled studies with better follow-up.
Question 2: In Lumbar Fusion Using Iliac Crest Bone Graft, Does a Single-Incision Midline Approach Reduce Postoperative Iliac Crest Pain Compared with a Two-Incision Traditional Approach?
When the decision is made to harvest ICBG, consideration must be given to reducing donor site morbidity, including long-term pain, which is a major factor. There is considerable surgeon variability with regard to harvesting ICBG including the use of one incision or two incisions. Two studies met the screening process and addressed the choice of incisions specifically: one RCT (level 2) and one retrospective cohort studies (level 3). One cohort study looked at ICBG harvest versus no harvest (bone morphogenetic protein) and one study had the patients blinded to the side of harvest through a separate incision and patients underwent reconstruction of the defect at the time of harvest. At a very low level of evidence, there was less pain over the iliac crest harvest site, better patient satisfaction, and comparable complication rates for graft harvested through the midline incision. There was also a low concordance rate for correctly identifying the side of iliac crest harvest when it was harvested through the midline incision. Based on the available literature, harvesting graft through the same midline incision may be a better option than a using a separate incision.
Again, this review was based on a relatively small number of low- to moderate-quality studies available in the literature. There was variability in the inclusion and exclusion criteria, primary and secondary end points, and again a variable rate of long-term follow-up. Once again, larger and more stringently controlled studies would better address this issue.
Disclosures
John C. France, none
James M. Schuster, none
Katherine Moran, none
Joseph R. Dettori, none
The authors addressed a question of great practical value to all spine surgeons with their formal review: Is locally derived morselized bone collected during neural decompression as good as autologous bone graft harvested from the posterior iliac crest? The authors added some other important factors to the question, such as patient satisfaction with a one- versus two-incision approach and whether patients could accurately identify the side of a posterior iliac crest harvest if done through a single incision. The EBSJ reviewers appreciated the clarity of the authors’ study design and the practical applicability of their findings, namely that local bone graft can be used in good faith as substitute for autologous iliac crest graft for fusions and that a single-incision technique for posterior lumbosacral incisions seems to be preferred by patients to the more traditional two-incision technique. The authors commented on the very low level of evidence of the study at the basis of their conclusions, meaning that a single, larger, better-designed study could change the conclusions of this study.
On a technical note, variables for a future bone graft healing studies would ideally incorporate some attempt at volumetric quantification of morselized bone grafts deployed and also details such as “stretching” of bone graft with allograft or osteobiologics. Associated patient factors, such as age of patient, atherosclerosis, bone healing impairment, and anti-inflammatory use, could also influence results heavily. Such factors are commonly omitted in bone graft-related studies. Nevertheless, the present study provides clear answers to daily practice habits. EBSJ wishes to thank the authors for their helpful contribution.
Footnotes
Acknowledgments
Analytic support for this work was provided by Spectrum Research, Inc. with funding from AOSpine.