
Abstract
Study Design
Computed tomography–based cohort study.
Objective
Although there are publications concerning the relationship between the vertebral artery and uncinate process, there is no practical guide detailing the dimensions of this region to use during decompression of the intervertebral foramen. The purpose of this study is to determine the anatomic parameters that can be used as a guide for thorough decompression of the intervertebral foramen.
Methods
Fifty-one patients with three-dimensional computed tomography scans of the cervical spine from 2003 to 2012 were included. On axial views, we measured the distance from the midline to the medial and lateral cortices of the pedicle bilaterally from C3 to C7. On coronal reconstructed views, we measured the minimum height of the uncinate process from the cranial cortex of the pedicle adjacent to the posterior cortex of vertebral body and the maximal height of the uncinate process from the cranial cortex of the pedicle at the midportion of the vertebral body bilaterally from C3 to C7.
Results
The mean distances from midline to the medial and lateral cortices of the pedicle were 10.1 ± 1.3 mm and 13.9 ± 1.5 mm, respectively. The mean minimum height of the uncinate process from the cranial cortex of the pedicle was 4.6 ± 1.6 mm and the mean maximal height was 6.1 ± 1.7 mm.
Conclusions
Our results suggest that in most cases, one can thoroughly decompress the intervertebral foramen by removing the uncinate out to 13 mm laterally from the midline and 4 mm above the pedicle without violating the transverse foramen.
Introduction
Vertebral artery injury is a catastrophic complication that can occur during anterior decompression of the cervical foramen. The distance between the uncinate tip and the vertebral artery was found to be as short as 1 mm on cadaveric specimens. 1 , 2 There are controversies regarding the width of the uncinate process that needs to be resected for adequate decompression of the intervertebral foramen; the recommended widths based upon cadaveric studies has been variously reported as 3.5 to 4.5 mm, 2 4 mm, 3 5 mm, 4 , 5 or 6 mm. 6 None of these studies, however, provide the most important information about the location of the vertebral artery and the height of the uncinate process that needs to be resected to achieve adequate decompression of the intervertebral foramen.
The aim of the present study is to determine the anatomic parameters between the various structures near the intervertebral foramen and the transverse foramen where the vertebral artery lies.
Materials and Methods
This study was approved by the institutional review board (number: 2013-I141) at the institution of the corresponding author. It was a retrospective radiologic study of 51 patients who were randomly selected from a larger group of 1,939 patients. They had undergone three-dimensional (3D) computed tomography (CTs) of the cervical spine as part of their workup for neck pain, radiating arm pain, or difficulty with ambulation, from January 2003 to January 2012 at the first author's academic institution. Scanning parameters of the cervical spine 3D CT consisted of 2-mm thickness and 2-mm interval slices. We excluded patients with a previous history of spinal trauma or any operations for trauma, infection, or tumor. The mean age was 66.6 years. There were 30 men and 21 women.
We measured the distance between the midline and the uncinate process, as well as the transverse foramen, which we used as the location of the vertebral artery. On the axial view, we drew a line bisecting the vertebral body to identify the midpoints of the anterior and posterior cortices (Fig. 1). From the midpoint of the anterior cortex of the vertebra, we drew lines to the medial and lateral cortices of the pedicle bilaterally from C3 to C7. We measured the distance along the posterior cortex of the vertebral body to the structures involved in the foraminal decompression (Fig. 1). The distance from the midline to the medial pedicle cortex (red line) represents the central canal (Fig. 1). The distance from the midline to the lateral cortex of the pedicle (yellow line) represents the central canal plus the intervertebral foramen to the lateral border of the uncinate process (Fig. 1).
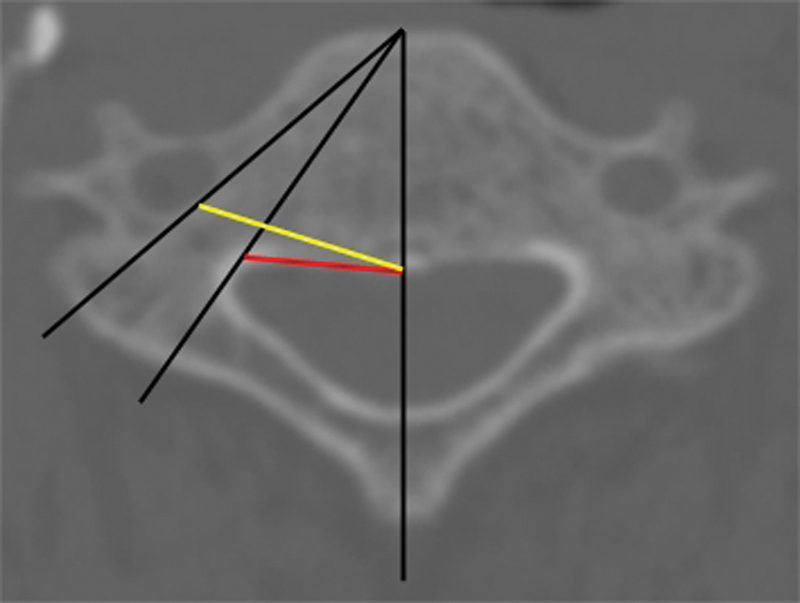
The axial view of a cervical vertebra demonstrating all the measured parameters, the distance from the midline to the medial pedicle cortex (red line), and the distance from the midline to the lateral pedicle cortex (yellow line).
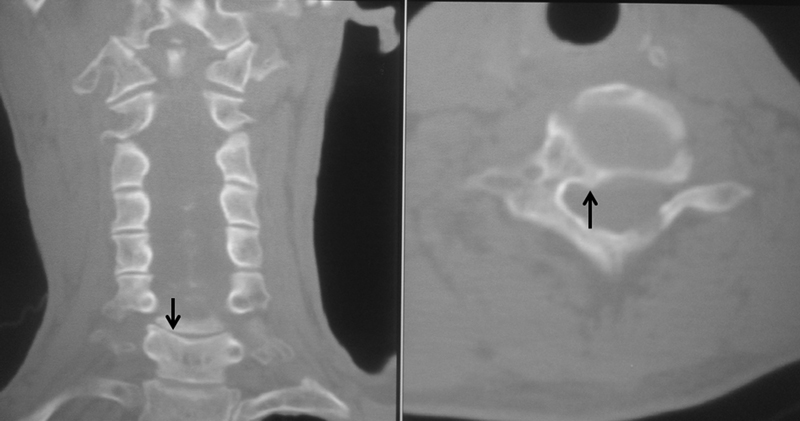
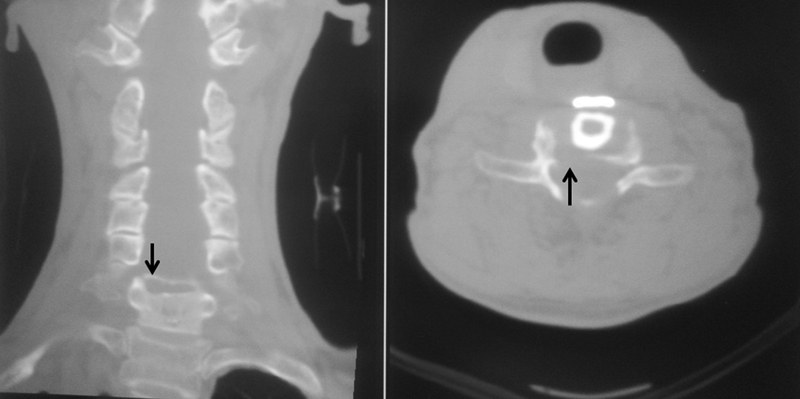
We measured the height of the uncinate process bilaterally from C3 to C7 on two coronal 3D CT views of the cervical spine: at the level of the posterior cortex of the vertebral body (Fig. 2) and at the midportion of the vertebral body (Fig. 3). These two views represent, respectively, the minimal and maximal heights of the uncinate process from the cranial cortex of the pedicles.
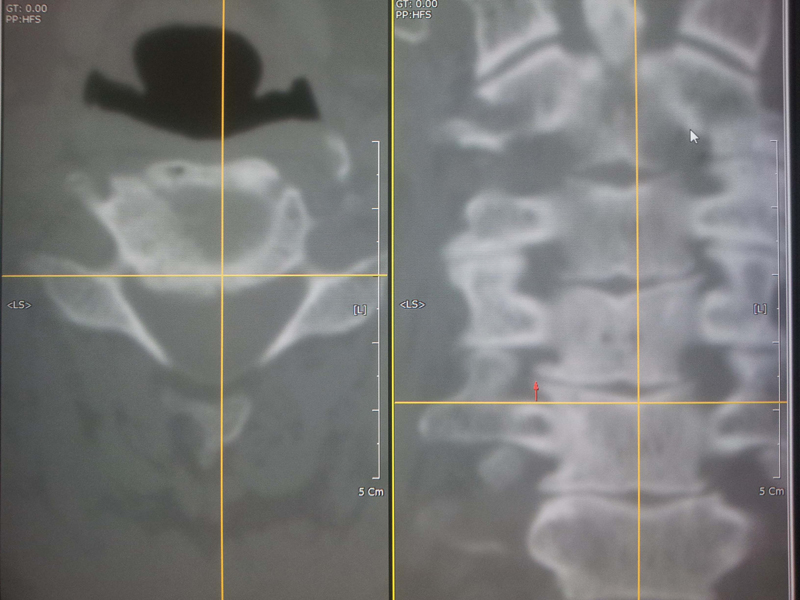
The horizontal line on the axial image on the left depicts the location of the coronal cut on the right. The coronal view is adjacent to the posterior cortex of the vertebral body. The minimum height of the uncinate process (red arrow) is measured from a horizontal line connecting the cranial cortex of the pedicles.
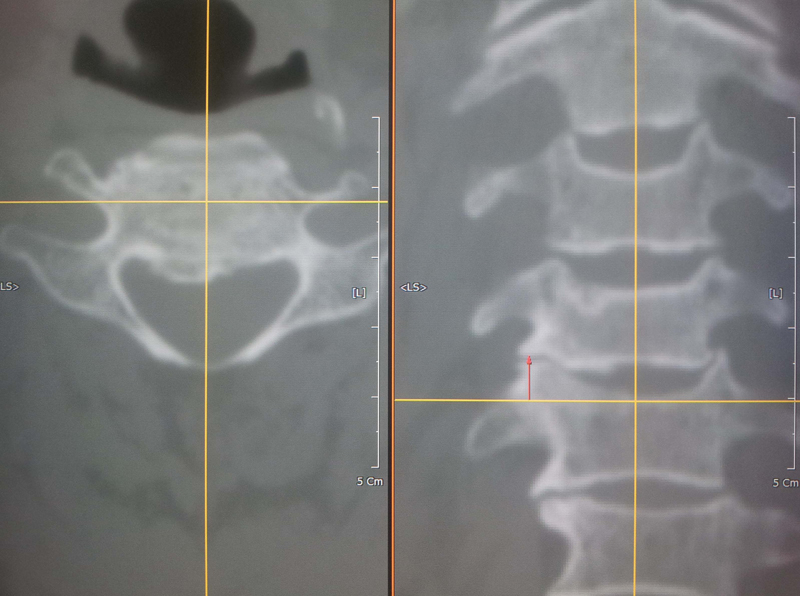
The horizontal line on the axial image on the left depicts the location of the coronal cut on the right. On the right side is the coronal view at the midportion of the vertebral body. The maximal height of the uncinate process (red arrow) is measured from a horizontal line connecting the cranial cortex of the pedicles.
Results
The mean distances from the midline to the medial and lateral cortices of the pedicle were 10.1 ± 1.3 mm and 13.9 ± 1.5 mm, respectively (Table 1). The mean distance from the midline to the medial cortex of the pedicle increased from C3 to C5 or C6 with a minimum of 9.2 ± 1.1 mm on the right and a minimum of 9.3 ± 1.1 mm on the left at C3 (Table 1). Therefore, a complete decompression of the spinal canal would have to extend at least 20 mm from side to side (Figs. 4, 5, 6). The mean distance from midline to the lateral cortex of the pedicle gradually increased from C3 to C6 with a minimum 13.1 ± 1.4 mm on the right and minimum 13.2 ± 1.7 mm on the left at C3 (Table 1). This data suggests that to thoroughly decompress the foramina bilaterally, one has to extend a minimum of 26 mm from side to side. Further lateral would place the vertebral artery at risk.
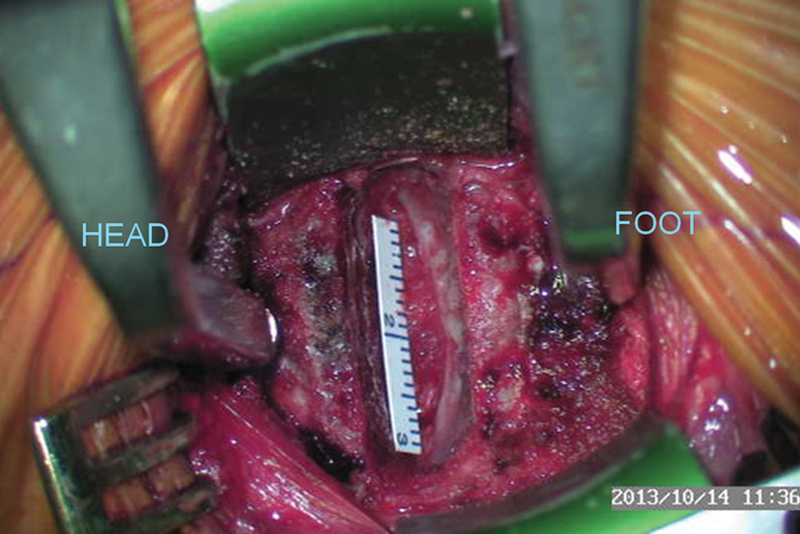
Paper ruler of 20 mm necessary for thorough decompression of the spinal canal.
The computed tomographic views showing the osteophyte (black arrows) medial to the right pedicle compressing spinal cord at C6–C7 disk level before the decompressive surgery under the authors’ practical guide.
The computed tomographic views showing the complete removal of the osteophyte (black arrows) medial to the right pedicle compressing spinal cord at C6–C7 disk level after the decompressive surgery under the authors’ practical guide of up to 10 mm laterally from the midline to medial cortex of the pedicle.
Distance from midline to the medial and lateral cortices of the pedicle
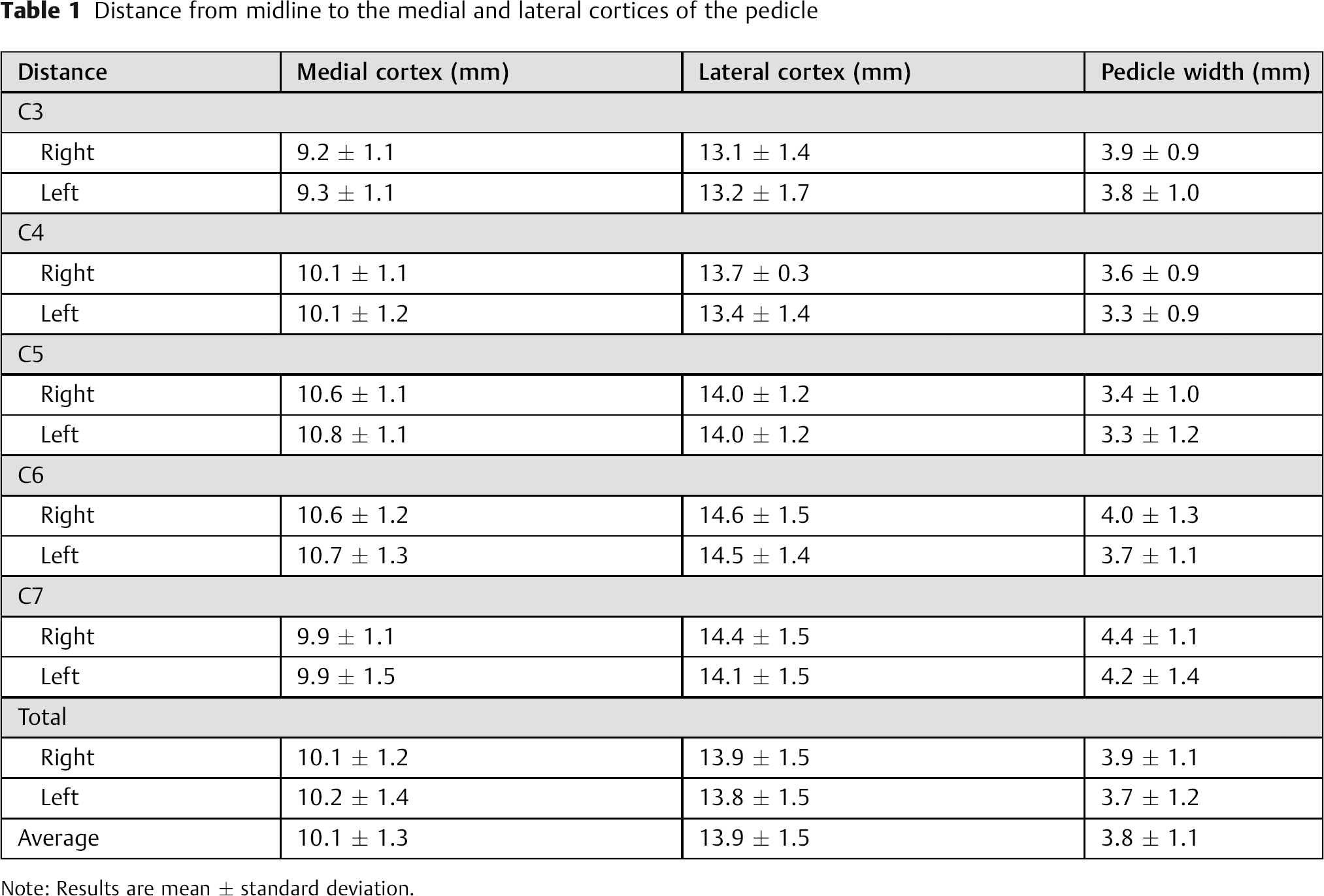
Note: Results are mean ± standard deviation.
To determine the width of the pedicles, we took the difference between the distances to the medial and lateral cortices of the pedicle. The average was 3.8 ± 1.1 mm. The size decreased from C3 to C5, increased from C5 to C7, and was smallest at C5 (Table 1).
The mean minimal height of the uncinate process from the cranial cortex of the pedicle was 4.6 ± 1.6 mm and the mean maximal height was 6.1 ± 1.7 mm (Table 2). The mean minimal height of the uncinate process was highest at C3 and lowest at C6 (Table 2). The mean maximal height of the uncinate process decreased from C3 to C7 (Table 2). Because these are the normal values, in uncinate hypertrophy that causes root compression, the decompression of the uncinate process would need to extend more than 4 mm and less than 6 mm above the level of the pedicle to thoroughly decompress the foramen.
The minimum and maximum heights of the uncinate process from the cranial border of the pedicle
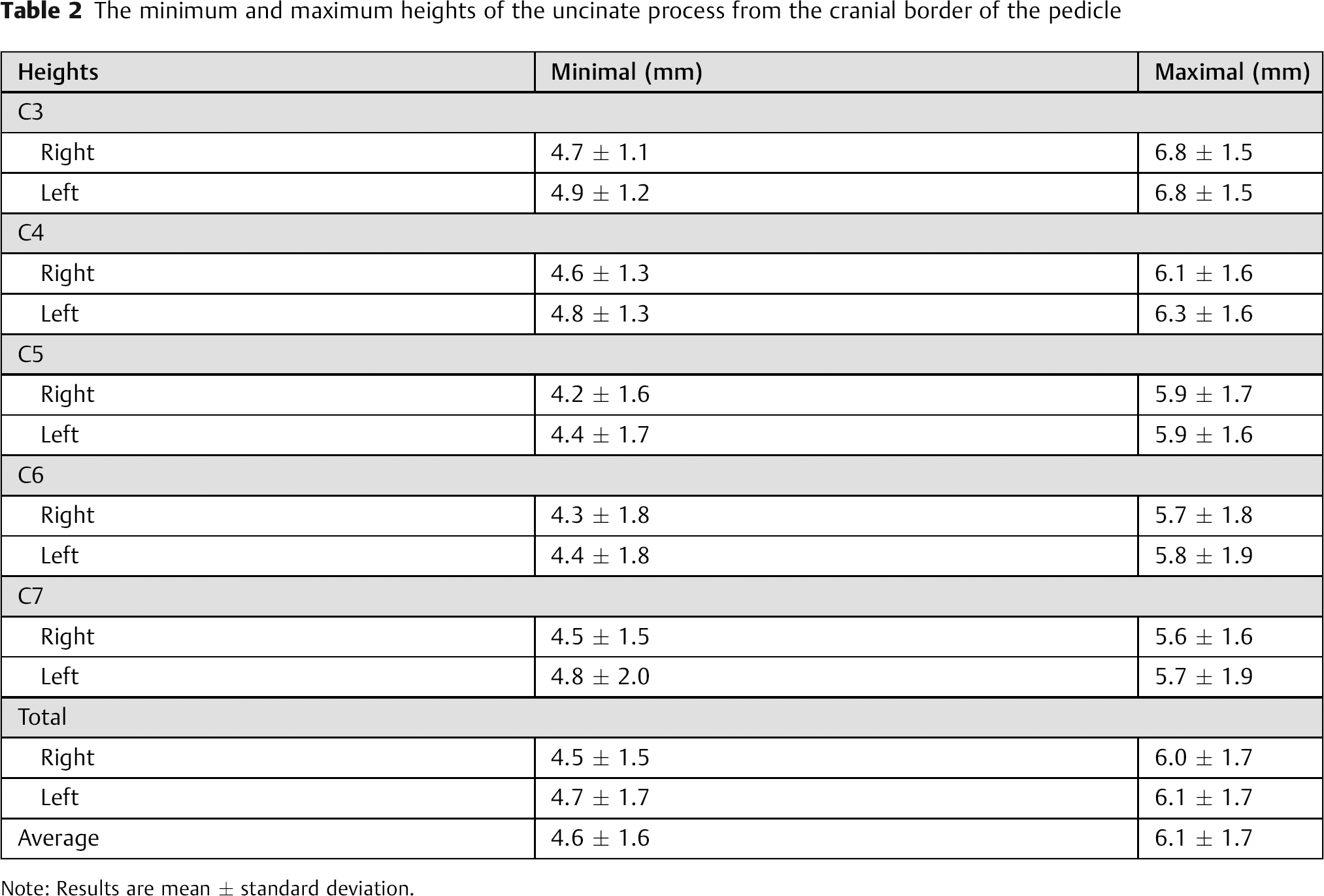
Note: Results are mean ± standard deviation.
Discussion
Injury to the vertebral artery, which is at risk during anterior foraminal decompression, can result in catastrophic consequences such as massive bleeding, cerebellar or brainstem infarction, and death. 1 , 2 , 7 Previous studies have determined that the uncinate process has a width from 3.5 to 6 mm. 2 , 3 , 4 , 5 , 6 However, the studies did not provide information regarding the location of the vertebral artery and the height of the uncinate process. The purpose of the present study is to determine the anatomic parameters of the uncinate process and vertebral artery, which can be used as a guide for thorough decompression of the foramen.
We found that the mean distances from the midline to the medial and lateral cortices of the pedicle were 10.1 ± 1.3 mm and 13.9 ± 1.5 mm, respectively. The pedicle width was an average of 3.8 ± 1.1 mm. The mean height of the uncinate process above the cranial border of the pedicle (measured from coronally reconstructed CTs) was 4.6 ± 1.6 mm at the level of the posterior cortex and 6.1 ± 1.7 mm at the midvertebral body level.
The mean distances from the midline to the medial cortex of the pedicle were longer at C5 and C6 and shorter at C3. The distance was greater at C6 than C7 in the current study. These results were not consistent with the previous studies, 8 , 9 which found that the interpedicular distance was smallest at C3 and greatest at C7 (Table 3). 8 , 9 The difference might be explained by the fact that the interpedicular distance was measured by the maximal distance between the medial aspects of the pedicles in previous studies, 8 , 9 and we measured the distances from the midline to the medial cortex of the pedicle where the pedicle meets the vertebral body (Fig. 7).
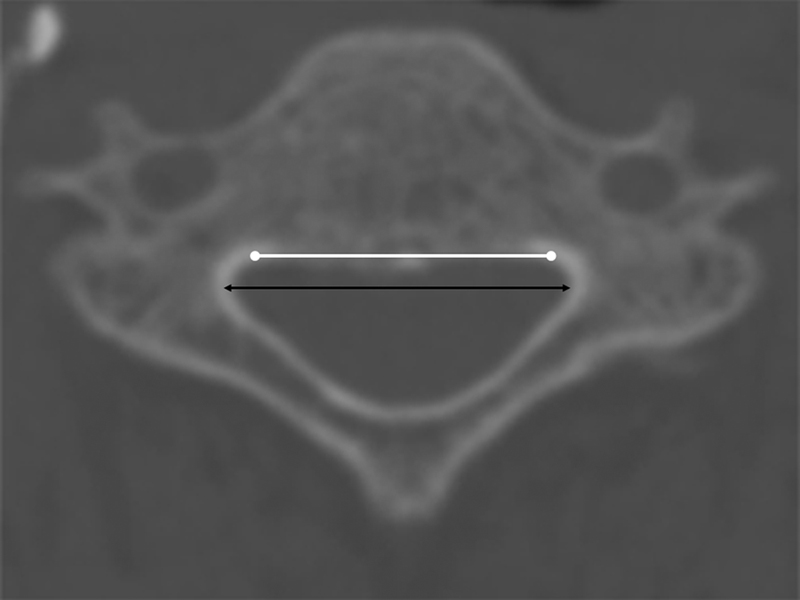
The maximal interpedicular distance in the previous studies between the medial aspect of the pedicles (black line) and the interpedicular distance in the current study between the medial cortices of the pedicle where the pedicle meets the vertebral body (white line).
Maximum interpedicular distance and the interforaminal distance reported in the literature
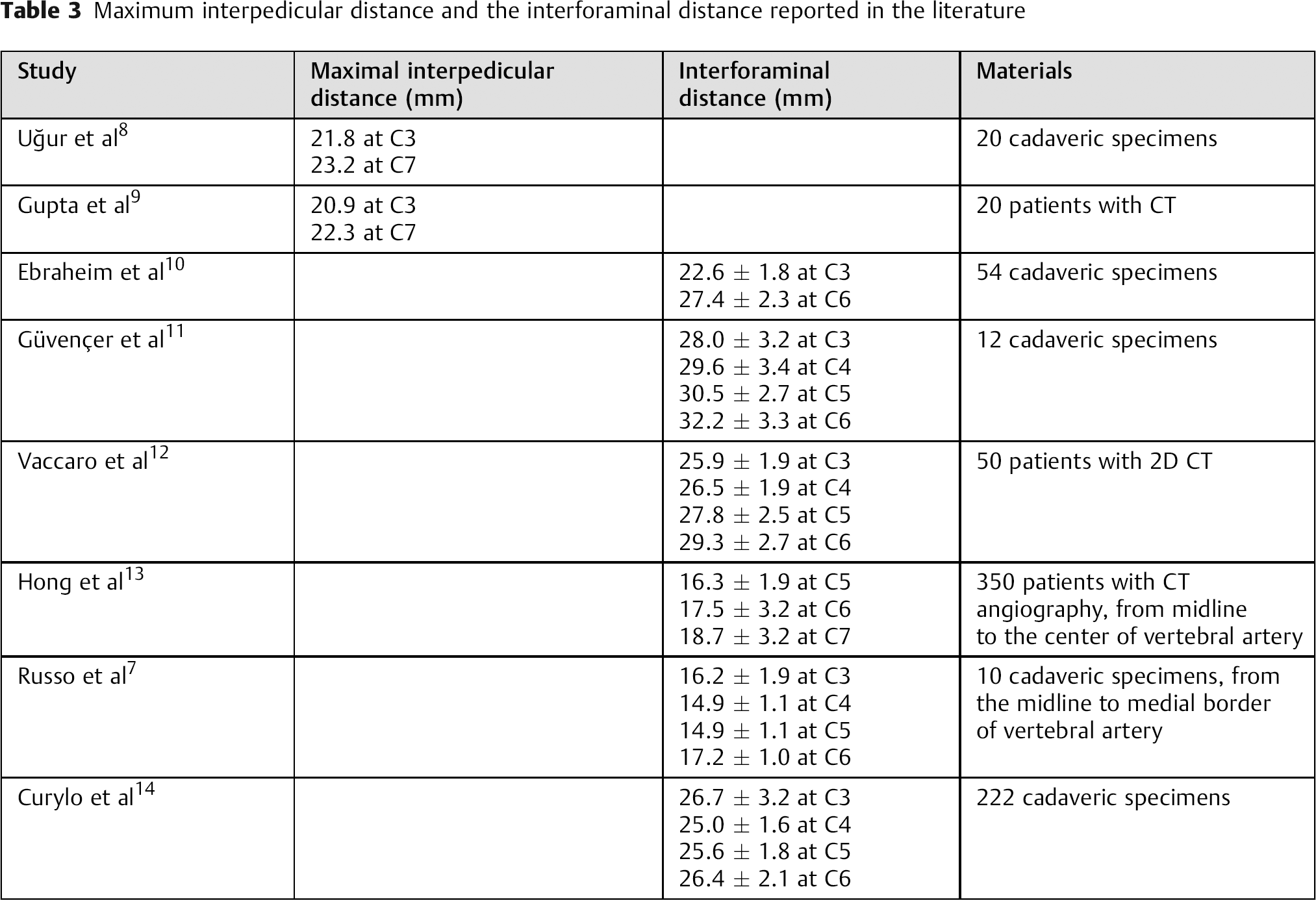
The mean distance from the midline to the lateral cortex of the pedicle was longer at C6 and shorter at C3. These results showing increasing distance from C3 to C6 are similar to four of the previous studies (Table 3). 10 , 11 , 12 , 13 Two of these were cadaveric, 10 , 11 and two were CT studies (Table 3). 12 , 13 However, two other cadaveric studies found no obvious pattern of increasing or decreasing distances as one went from C3 to C7 (Table 3). 7 , 14 It might be explained by the fact that Russo et al had measured the distance from the midline to the medial border of the vertebral artery infused with colored silicone, not the distance between the lateral cortices of cervical pedicles. 7 Curylo et al had measured the distance between the right and left transverse foramena. 14
In the current study, the pedicle width was 3.8 ± 1.1 mm. The pedicle width was smallest at C5, decreasing from C3 to C5 and increasing from C5 to C7. In contrast to previous studies, we did not measure the width of the uncinates. The purpose of the previous studies was to elucidate the anatomic features of the uncinate process including the uncinate width. 1 , 2 , 6 In contrast, our purpose is to show the safe margin for avoiding vertebral artery injury. For this purpose, the most important landmark is the lateral margin of the pedicle, which is also the medial wall of the foramen transversarium, where the artery lies.
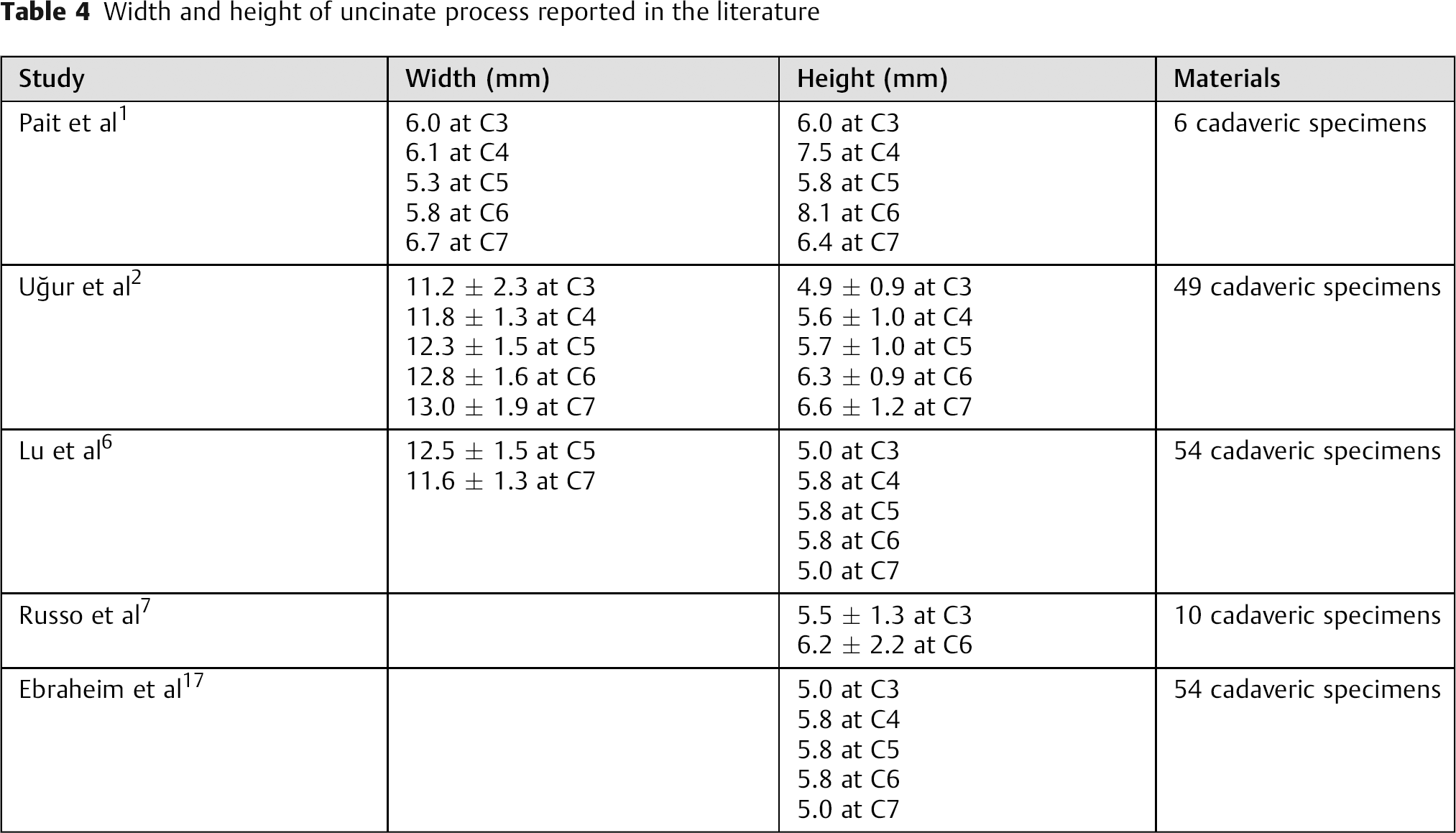
The height of the uncinate process was reported as 4.8 mm in a study with 40 cadaveric specimens and 6 mm in a study with 30 cadaveric specimens. 15 , 16 The maximum height of the uncinate process gradually decreased from C3 to C7 in the current study. However, some previous studies showed results contrary to our results (Table 4). 2 , 7 The other previous studies did not show any tendency of the uncinate process height to decrease from C3 to C7 (Table 4). 1 , 6 , 17 This discrepancy might be explained by the fact that they had a different definition of uncinate process height. 1 , 2 , 6 , 7 , 17 The height of the uncinate process was measured as the distance from the tip of the process to the superior surface of the vertebral body, 2 , 6 , 17 or to the rostral edge of the superior surface of the vertebral body. 1 The advantage to our measuring method is that if a spine surgeon wants to thoroughly decompress the foramen, they must remove any spurs that lie cranial to the pedicle and not just those above the edge of the vertebral body, because spurs often extend caudally down to the cranial border of the pedicle.
Width and height of uncinate process reported in the literature
As with any study, the present investigation has several limitations. First, some of the measurements were made on normal uncinates. In such cases, the surgeon does not need to decompress the foramen. The numbers are likely to differ in cases where there is severe uncinate hypertrophy, which is the kind of situation where one has to do an uncinate resection. Therefore, the lateral aspect of the uncinate would likely be different. However, the dimensions of the pedicle would not be affected by uncinate hypertrophy and should be valid. Second, the study was done in Korean subjects, and the size may be different in other races. Third, our images were not angiogram CTs. Therefore, our measurements cannot determine the true distance between the artery and the bony structures. Instead, we used the transverse foramen as the location of the artery. The foramen itself is probably 1 to 2 mm medial to the artery. Therefore, using the transverse foramen as the location of the artery is not entirely accurate. Nevertheless, in the vast majority of cases, it is reasonable to state that one should keep the decompression of the foramen posterior and medial to the wall of the transverse foramen. Finally, the measurements were made in 51 cases. The small sample size is problematic. There may also be individual variations based on body size such that one cannot blindly trust the numbers that we describe for any given patient. It is recommended that the surgeon preoperatively measure it in all cases where uncinate resection is being planned. Therefore, the main value of our study is in defining the methodology for making the measurements, which surgeons should consider doing prior to uncinate resection surgery. Despite these shortcomings, to our knowledge, this study is the first report providing anatomic measurements that can be used as a guide for decompressing the neural foramen without injuring the artery.
In conclusion, our results suggest that in most cases, one can remove osteophytes between the cervical pedicles within the spinal canal up to 10 mm laterally from the midline and safely remove uncinate process osteophytes up to 13 mm laterally from the midline and up to 4 mm of the height of the uncinate process from C3 to C7 without violating the transverse foramen. It should be noted that these numbers should only serve as a guide to where the artery is most likely to lie but that individual measurements may differ due to anatomic variations. Therefore, it is recommended that the surgeon examine preoperative CT or magnetic resonance images prior to performing such decompressions.
Disclosures
Moon Soo Park, none
Seong-Hwan Moon, none
Tae-Hwan Kim, none
Jae Keun Oh, none
Jae Kyun Jung, none
Hyung Joon Kim, none
K. Daniel Riew, Board membership: CSRS, KASS, AOSpine; Royalties: Osprey, Biomet, Medtronic Sofamor Danek; Stock/stock options: Amedica, Benvenue, Expanding Orthopedics, Nexgen Spine, Osprey, Paradigm Spine, Spinal Kinetics, Spineology, Vertiflex, PSD.