
Abstract
Study Design
Retrospective case series.
Objective
Recent studies suggest that baseline hematocrit (Hct) levels may affect the surgical outcomes after orthopedic procedures. The authors examined whether preoperative Hct values had a significant effect on the hospital length of stay (LoS) after lumbar spinal procedures.
Methods
We retrospectively reviewed patients who underwent routine lumbar spine procedures from November 2012 through September 2013. Patients were included if they had both a baseline Hct and hospital LoS recorded. Patients were divided into two groups: those with an Hct ≥ 40% (nonanemic) and those with an Hct < 40% (anemic). LoS after surgery was evaluated for each group.
Results
One hundred seventeen patients underwent lumbar spine procedures for lumbar stenosis (n = 34), symptomatic lumbar disk herniation (n = 39), lumbar spondylolisthesis (n = 26), lumbar adjacent segment disease (n = 8), or symptomatic recurrent lumbar disk herniation (n = 10). Mean LoS was 3.3 and 2.4 days in anemic (27 patients) and nonanemic groups (90 patients), respectively (p = 0.02). The linear regression analysis demonstrated that a decrease in Hct was associated with a longer stay. A decrease from preoperative to postoperative day 1 Hct of 3.5 points resulted in an increased LoS of 1 day (R 2 = 0.145; p = 0.002). The correlation of Hct decrease with longer LoS remained (β = 0.167, p = 0.006) after adjusting for other variables with multivariate regression analysis.
Conclusions
Lower preoperative Hct or a substantial decrease in Hct may contribute to longer hospitalization after lumbar spine surgery. These findings should prompt an investigation into the strategies for optimizing Hct levels in patients with preoperative anemia prior to lumbar spine procedures.
Introduction
As rising health care costs become an area of increasing focus, length of stay (LoS) after routine surgical procedures has become an important consideration. With over $1.5 billion dollars spent each year on the surgical management of lumbar stenosis alone, 1 the identification of factors that affect the associated health care costs could have an outsized impact on the field.
Preoperative anemia has been shown to be a significant risk factor for mortality and morbidity in a wide variety of surgical procedures, 2 , 3 and it has been shown to have an effect on LoS in the colorectal and urologic surgery populations. 4 , 5 None of the studies that have included preoperative anemia among the factors identified as predictors of LoS in lumbar spine surgery in the past have investigated this factor specifically across multiple procedure types. 6 , 7 To better understand the impact of preoperative anemia in this patient population, we examined the effect of low hematocrit (Hct) on LoS in patients undergoing spinal procedures for lumbar stenosis, symptomatic and recurrent lumbar disk herniation, lumbar spondylolisthesis, and lumbar adjacent segment disease. We also examined the effect that a decrease in Hct had on LoS.
Materials and Methods
Patient Selection
After obtaining institutional review board approval, we retrospectively reviewed the medical records of patients enrolled in a national quality registry (The National Neurosurgery Quality and Outcomes Database) who underwent routine lumbar spinal procedures at our tertiary care center from November 2012 through September 2013. Patients with the diagnosis of lumbar stenosis, symptomatic lumbar disk herniation, lumbar spondylolisthesis, lumbar adjacent segment disease, or symptomatic recurrent lumbar disk herniation were identified. Patients were included if they had both a baseline Hct drawn within 3 weeks of the surgery and hospital LoS recorded.
Data collected included age, sex, preoperative diagnosis, surgery type, preoperative Hct, postoperative Hct, LoS, and complications. The preoperative Hct was defined by the most recent Hct value prior to surgery drawn within 2 weeks of the operative date. The postoperative Hct was defined as the first Hct value postoperatively drawn within 48 hours of the procedure. LoS was defined as the period from the time of admission to the time of discharge. Complications tracked included deep vein thrombosis, new neurologic deficit due to magnetic resonance imaging–confirmed stroke, myocardial infarction, urinary tract infection, surgical site infection, surgical site hematoma, new lower extremity deficit, readmission within 31 days postoperatively, readmission between 31 days and 3 months postoperatively, and return to the operating room during the same stay. Surgery type was divided into three categories: microdiskectomy (one- or two-level), laminectomy/decompression, and fusion.
Data Analysis
The Centers for Disease Control guidelines for anemia use an Hct level of 40% based on normative laboratory values as a threshold.8 For the evaluation of the effect of preoperative Hct, we divided the patients into two groups using this threshold. Student t test was used to compare LoS as well as other parametric variables in the anemic (<40%) and nonanemic (>40%) groups, with a level of p < 0.05 considered significant. Nonparametric data was analyzed by chi-square analysis. Means are reported with standard deviation. Linear and multivariate regression analysis was performed on Hct change data, with significance defined as p < 0.05. All calculations were performed using SPSS (IBM, Armonk, New York, United States).
Results
We analyzed 117 patients in this study, including 65 men (56%) and 52 women (44%) with an average age of 57.8 years (Table 1). The average preoperative Hct for all patients was 43.2%, with a range of 29.8 to 51.6%; the mean change in Hct from pre- to postoperatively was 6.2%. The average LoS for all patients was 2.6 days.
Characteristics of 117 patients who underwent routine lumbar spinal surgery
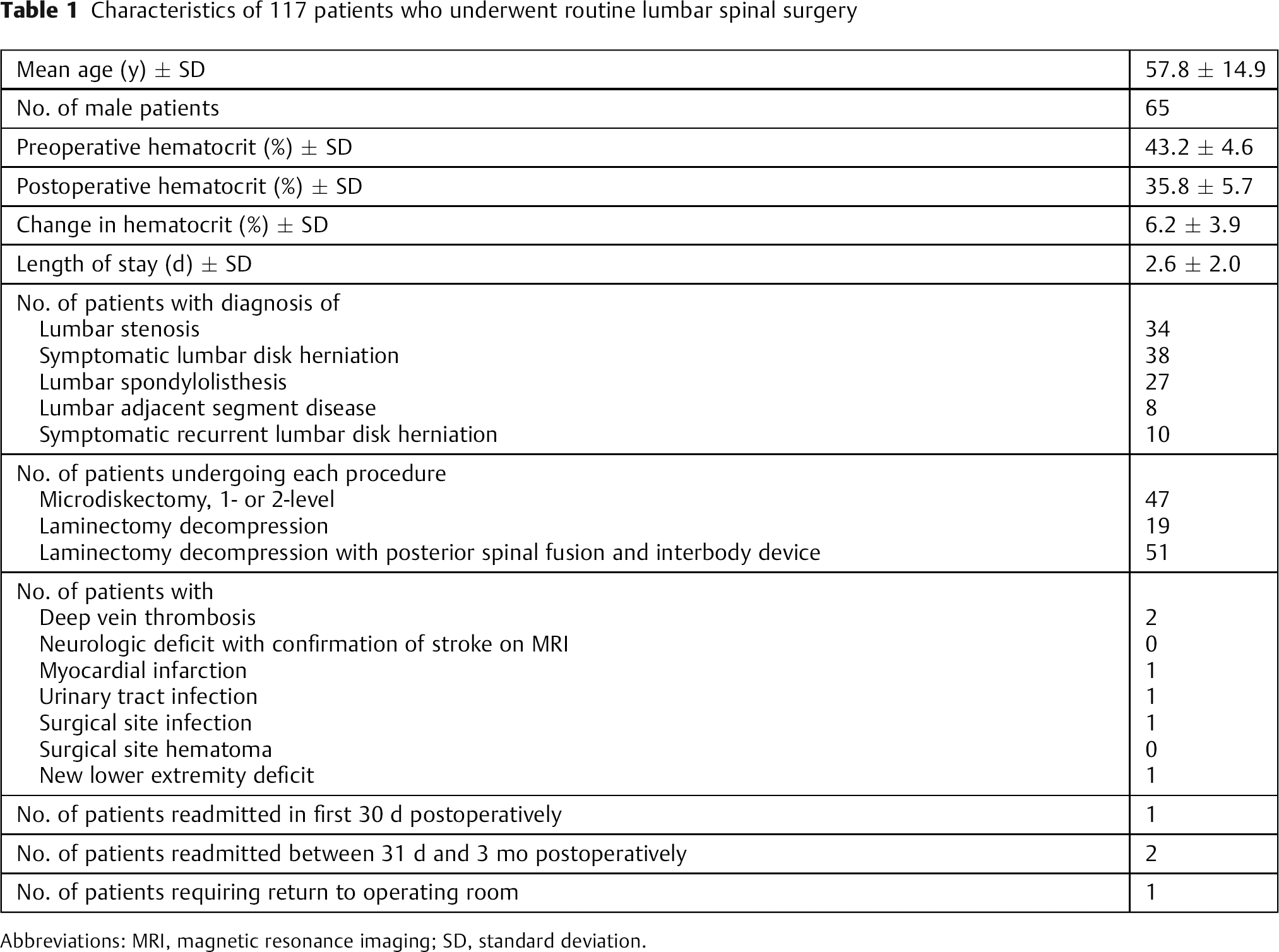
Abbreviations: MRI, magnetic resonance imaging; SD, standard deviation.
Twenty-seven subjects were anemic preoperatively; these patients had a mean preoperative Hct of 37% (Table 2). In the 90 patients who were not anemic preoperatively, the mean preoperative Hct value was 45.3%. There was no significant difference in the preoperative diagnosis or type of surgery performed for these groups, and women were significantly more likely to fall into the anemic category (p = 0.001). In addition, anemic patients were more likely to be older (p = 0.05). There was a significant difference (p = 0.02) in LoS for the patients in the anemic group (3.3 days) compared with those in the nonanemic group (2.3 days). There were no significant differences in the rates of deep vein thrombosis, new stroke confirmed on magnetic resonance imaging, myocardial infarction, urinary tract infection, spinal cord injury, new lower extremity deficit, readmission, or return to the operating room between the anemic and nonanemic groups. There was no significant difference in LoS in the anemic patients when analyzed within the surgical groups (data not shown).
Analysis of baseline characteristics, length of stay, and complications in anemic (Hct ≤40) and nonanemic patients
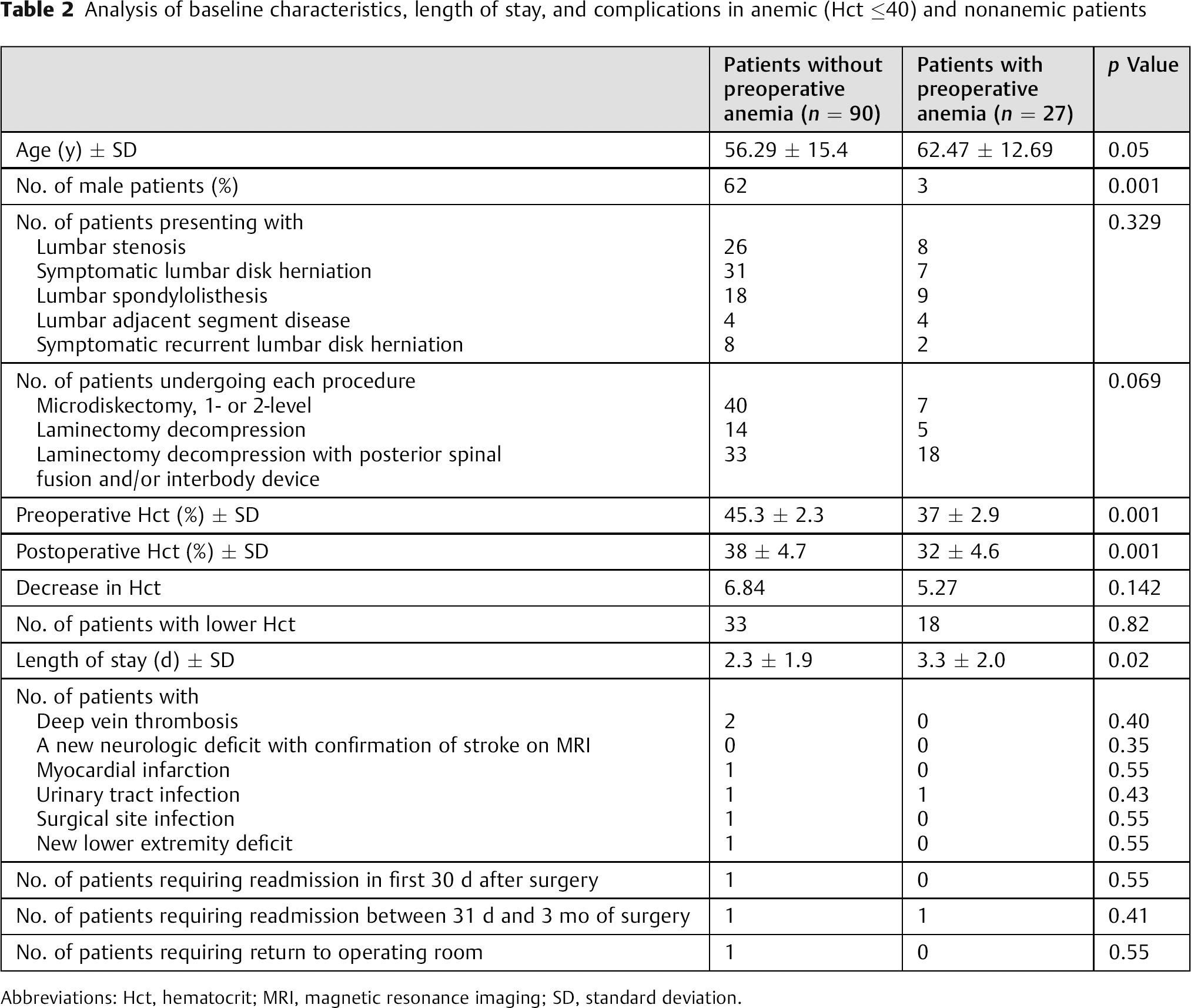
Abbreviations: Hct, hematocrit; MRI, magnetic resonance imaging; SD, standard deviation.
Fifty-one patients had postoperative Hct drawn and were included in Hct change calculations (Fig. 1). The linear regression analysis demonstrated a significant correlation of Hct change and the surgery type with increased LoS, with a decrease of 3.47% predicting a 1-day increase in LoS (R2 = 0.145, p = 0.002). This effect was maintained in the multivariate analysis after accounting for sex, age, surgery type, and complications (R2 = 0.522, p = 0.001, Table 3).
Multivariate analysis of hematocrit change in predicting length of stay
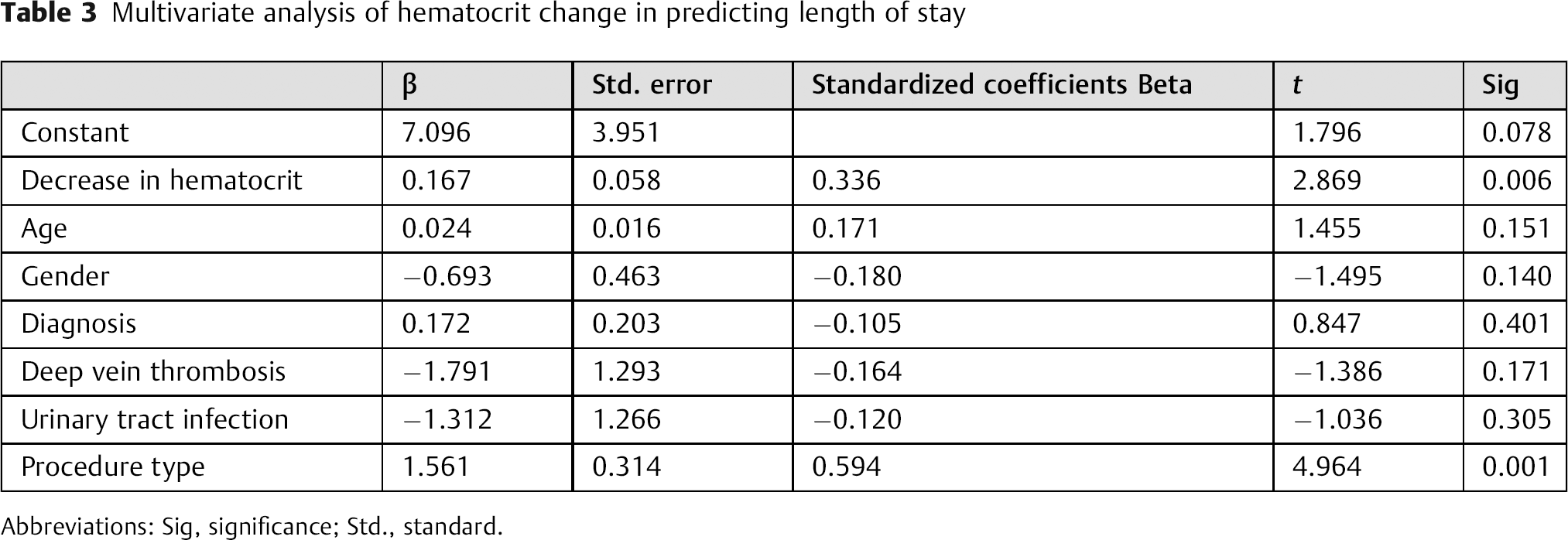
Abbreviations: Sig, significance; Std., standard.
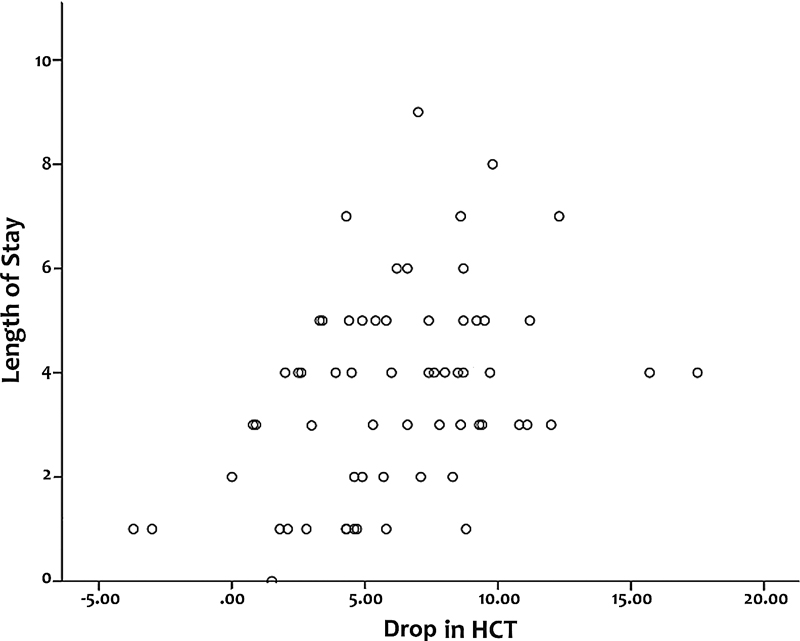
Graph showing linear regression analysis of hematocrit (HCT) change (as a percent of blood) and length of stay (days). Linear regression demonstrated a significant correlation between greater change in hematocrit and length of stay (β = 3.465, R = 0.381, R 2 = 0.145, p = 0.002).
Discussion
The aim of this study was to determine whether preoperative Hct level had a significant effect on the LoS in patients undergoing routine lumbar spinal procedures. Anemia has been shown to be a predictor of poor outcome across multiple surgical procedures. 2 , 3 With the high blood loss often associated with lumbar spinal procedures, 9 it stands to reason that this population may be especially vulnerable to baseline anemia. Our study suggests that preoperative anemia is indeed associated with a longer hospital stay, with the average LoS 1 day (30%) longer for patients who were anemic preoperatively. Considering that the cost of hospitalization itself, without considering surgeon fees, now approaches $14,000 for patients undergoing lumbar laminectomy, 10 a reduction in LoS by any amount could have significant benefits to both the patient and the health care system as a whole.
Our study also found that a decrease in Hct from preoperative to postoperative had a significant effect on LoS, which is in agreement with other studies that suggest that higher blood loss intraoperatively has a negative effect on time to discharge. 6 These studies, however, tend to use estimated blood loss as recorded intraoperatively for their calculations, which can often be difficult to objectively quantify. 11 Although Hct can itself be an inaccurate assessment of hematologic status because of subjective factors such as amount of blood loss and perspective of the evaluator (anesthesiologist versus surgeon), 12 our results suggest that Hct could provide an objective measure for surgical and postoperative planning.
We believe our study supports the hypothesis that preoperative Hct level has a significant effect on LoS; however, the study was limited by several factors. The first limitation is the retrospective nature of the analysis itself. Although the anemic and nonanemic groups in this study were comparable in regard to many factors including the diagnosis, type of surgery performed, Hct change, and evaluable complication rates, women were significantly more likely to be in the anemic group than men and there was a strong but nonsignificant trend toward higher age in the anemic group. Some studies do suggest that women and older individuals tend to have longer hospitalizations postoperatively, 1 although these increases are generally modest and are not seen in all investigations. 6 Nevertheless, there could be some interaction between these variables and the effect of Hct on LoS. There was no significant difference in the complication rates between the two groups, but complications overall were rare. As a result, only urinary tract infection and deep vein thrombosis occurred frequently enough to be included in statistical analysis. When broken down into surgery types, no individual category demonstrated a significant difference in LoS for anemic patients. We believe, however, that this result is likely secondary to the relatively small number of patients in each subgroup. Larger patient cohorts could help evaluate whether the preoperative Hct level has an effect on the complication rates and what impact anemia has on the LoS for specific lumbar surgeries.
With the myriad risks that preoperative anemia has been shown to augment in the surgical population, future studies in the modification of this risk factor would be beneficial. Some studies have evaluated the benefits of preoperative administration of agents such as erythropoietin and iron in anemic patients, 13 although the transfusion requirements rather than the hospitalization duration have usually been the primary focus. A 2004 study by Colomina et al considered the impact of preoperative erythropoietin administration on patients undergoing posterior spinal fusion with instrumentation and posterolateral interbody fusion. 14 These authors found no significant difference in LoS between the patients receiving erythropoietin and those who did not, but the erythropoietin group had a significantly higher intraoperative blood loss than the control group, which may have interfered with the LoS analysis.
Conclusion
We found that the patients who presented for lumbar spinal procedures with preoperative anemia and those who experienced a large drop in Hct postoperatively were at greater risk for prolonged hospitalizations. Further investigation is needed to determine the role of anemia management in this population.
Disclosures
Jian Guan, none
Michael Karsy, none
Meic H. Schmidt, none
Erica F. Bisson, Consultancy: nView Medical
Footnotes
Acknowledgments
We thank Kristin Kraus, M.Sc., for her assistance on preparation of this paper.