
Abstract
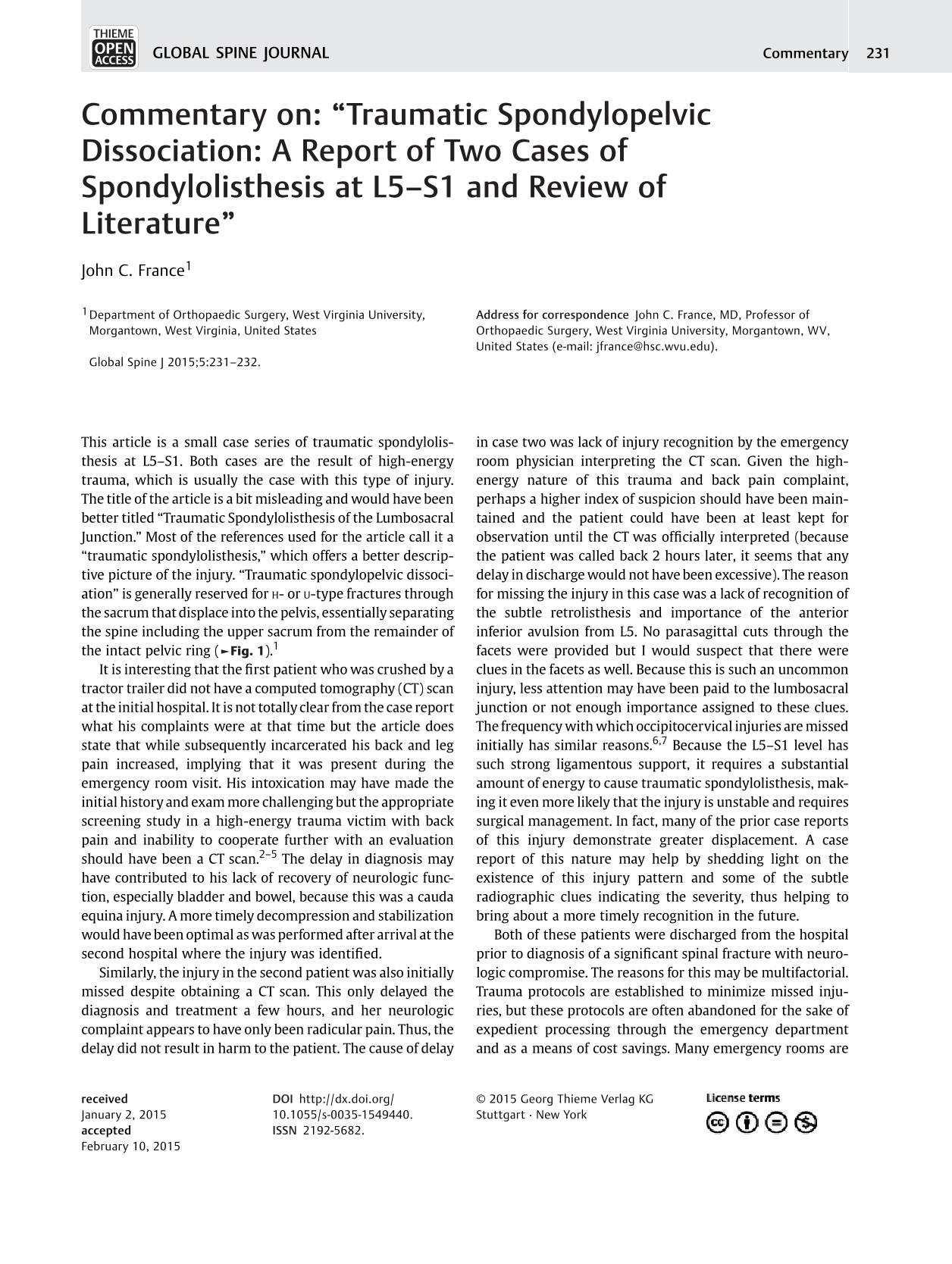
This article is a small case series of traumatic spondylolisthesis at L5–S1. Both cases are the result of high-energy trauma, which is usually the case with this type of injury. The title of the article is a bit misleading and would have been better titled “Traumatic Spondylolisthesis of the Lumbosacral Junction.” Most of the references used for the article call it a “traumatic spondylolisthesis,” which offers a better descriptive picture of the injury. “Traumatic spondylopelvic dissociation” is generally reserved for

A midsagittal computed tomography of a sacral u-type fracture with spondylopelvic dissociation. The spine and upper sacrum have broken free from the pelvic ring allowing the spine to displace anteriorly and inferiorly into the pelvis.
It is interesting that the first patient who was crushed by a tractor trailer did not have a computed tomography (CT) scan at the initial hospital. It is not totally clear from the case report what his complaints were at that time but the article does state that while subsequently incarcerated his back and leg pain increased, implying that it was present during the emergency room visit. His intoxication may have made the initial history and exam more challenging but the appropriate screening study in a high-energy trauma victim with back pain and inability to cooperate further with an evaluation should have been a CT scan. 2 , 3 , 4 , 5 The delay in diagnosis may have contributed to his lack of recovery of neurologic function, especially bladder and bowel, because this was a cauda equina injury. A more timely decompression and stabilization would have been optimal as was performed after arrival at the second hospital where the injury was identified.
Similarly, the injury in the second patient was also initially missed despite obtaining a CT scan. This only delayed the diagnosis and treatment a few hours, and her neurologic complaint appears to have only been radicular pain. Thus, the delay did not result in harm to the patient. The cause of delay in case two was lack of injury recognition by the emergency room physician interpreting the CT scan. Given the high-energy nature of this trauma and back pain complaint, perhaps a higher index of suspicion should have been maintained and the patient could have been at least kept for observation until the CT was officially interpreted (because the patient was called back 2 hours later, it seems that any delay in discharge would not have been excessive). The reason for missing the injury in this case was a lack of recognition of the subtle retrolisthesis and importance of the anterior inferior avulsion from L5. No parasagittal cuts through the facets were provided but I would suspect that there were clues in the facets as well. Because this is such an uncommon injury, less attention may have been paid to the lumbosacral junction or not enough importance assigned to these clues. The frequency with which occipitocervical injuries are missed initially has similar reasons. 6 , 7 Because the L5–S1 level has such strong ligamentous support, it requires a substantial amount of energy to cause traumatic spondylolisthesis, making it even more likely that the injury is unstable and requires surgical management. In fact, many of the prior case reports of this injury demonstrate greater displacement. A case report of this nature may help by shedding light on the existence of this injury pattern and some of the subtle radiographic clues indicating the severity, thus helping to bring about a more timely recognition in the future.
Both of these patients were discharged from the hospital prior to diagnosis of a significant spinal fracture with neurologic compromise. The reasons for this may be multifactorial. Trauma protocols are established to minimize missed injuries, but these protocols are often abandoned for the sake of expedient processing through the emergency department and as a means of cost savings. Many emergency rooms are coming under greater pressure from both of these fronts and although not specifically addressed in this case report, one has to wonder if these issues contributed to the delay in diagnosis and treatment of both of these patients.
The authors appear to have done a nice job in recognizing the severity of the injury and facilitating prompt decompression and stabilization. They offer some valid tips regarding surgical techniques used to verify that a decompression has been achieved and stability provided prior to leaving the operating theater.