
Abstract
Study Design
Case report and review of the literature.
Objective
To present a unique case of L5 radiculopathy caused by a sacral stress fracture without neurologic compression.
Methods
We present our case and its clinical evolution and review the available literature on similar pathologies.
Results
Relief of the unusual mechanical loading causing sacral stress fracture led to rapid resolution of radiculopathy.
Conclusion
L5 radiculopathy can be caused by a sacral stress fracture and can be relieved by simple mechanical treatment of the fracture.
Introduction
Stress fractures are uncommon skeletal injuries that are separated into fatigue and insufficiency-type injuries. The first sacral stress fracture was reported in 1982, and since that time several cases have been reported in athletes, civilians, military personnel, postpartum patients, patients with lumbosacral arthrodesis, and elderly patients with osteoporosis. We report a unique presentation of a sacral stress fracture in a healthy young police officer with an insidious onset of lower back pain and right leg radiculopathy while participating in an intense equestrian training program. The patient was conservatively managed with analgesics, rest, and temporary cessation of her horse-riding activities, followed by range of motion and aquatic-based physical therapy exercises. Her symptoms completely resolved over 6 weeks, and the patient was allowed to gradually return to full activities with no restrictions or sequelae. Although the prevalence of sacral stress fractures may be rare, physicians should be aware of their existence and consider them in patients who present with a suggestive history and known risk factors.
Case Report
A healthy 26-year-old female police officer was referred to our clinic for lower back pain associated with right leg radiculopathy. She denied any history of trauma or constitutional symptoms but had recently been transferred to a mounted patrol unit requiring the completion of an intense 4-month equestrian training program. Within 2 months of her training, the patient developed insidious onset of worsening lower back pain, followed by intermittent right leg numbness and sciatica down to her toes 3 weeks later. The pain was localized to her lower back and sacral region, worse at the end of the day, aggravated by horse-riding and forward-flexed positions, and relieved by rest. Numbness was present over the L5 distribution along the lateral leg and dorsum of her right foot. On physical examination, the patient was noted to have flattening of her lumbar spine with a stiffened pattern of trunk kinetics, acute pain on single right leg stance, and limited hip flexion with inability to touch her knees. Physical examination revealed 4/5 strength of her right extensor hallucis longus muscle, normal bilateral lower limb reflexes, and a positive straight leg raise and Lasègue test. Plain radiographs did not demonstrate any significant abnormalities except for a loss of normal lumbar lordosis, and considering the clinical findings, a temporary diagnosis of L5 degenerative disk compression was made.
Magnetic resonance imaging (MRI) scan of her lumbar spine was initially reported as negative and so was complemented with a scan of the pelvis. The MRIs (Figs. 1 and 2) demonstrated a 39-mm vertically oriented low-signal cleft along her right hemisacrum on both T1- and T2-weighted axial images lateral to, but with no extension into, the sacral neural foramina. The fracture was surrounded by bony edema presenting as an area of hyperintense signal on T2-weighted images, and the right L5 nerve was within 3-mm proximity of the fracture line and embedded within a proximal area of suggested periostitis. No other significant abnormalities were reported along the surrounding lumbar and sacral spine, and therefore a diagnosis of right sacral stress fracture with L5 nerve irritation was established. The patient was prescribed nonsteroidal anti-inflammatory drugs, and a period of rest was advised with limited impact activities and a temporary cessation of her equestrian training program. At her follow-up 2 weeks later, the patient's symptoms had significantly improved and she was sent for a dual-energy X-ray absorptiometry scan and referred to physiotherapy for range of motion exercises and aquatic-based muscle conditioning. At the follow up, ∼6 weeks from the day of her initial referral, her symptoms had completely resolved, and her bone mineral density investigations were reported as normal. The patient was allowed to gradually return to full activities and resume her equestrian training. No further complications or sequelae were noted.
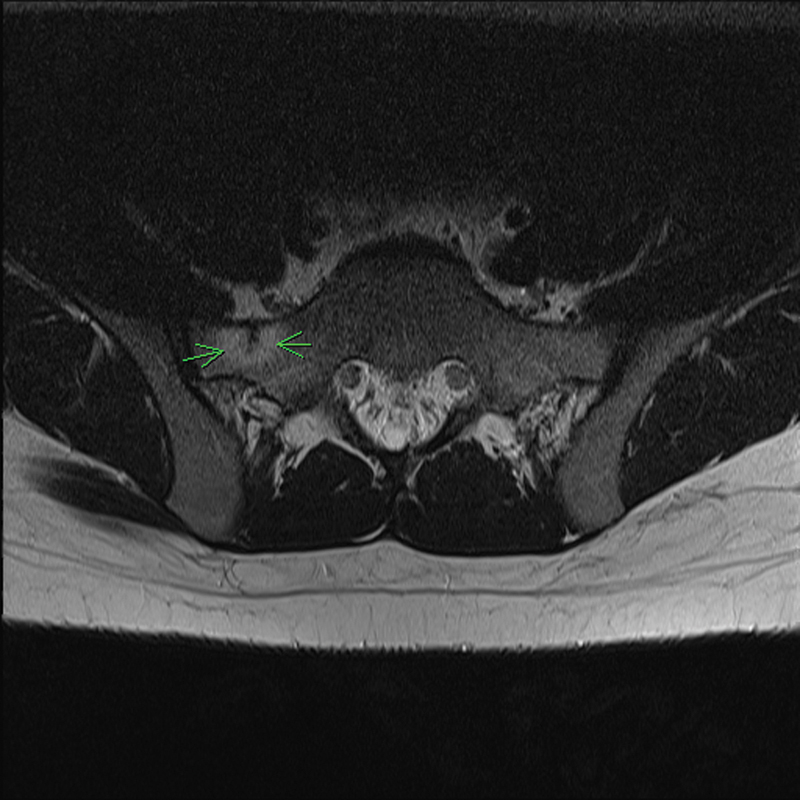
T1-weighted axial lumbar magnetic resonance image demonstrating an incomplete upper sacral fracture line surrounded by an area of bone edema.
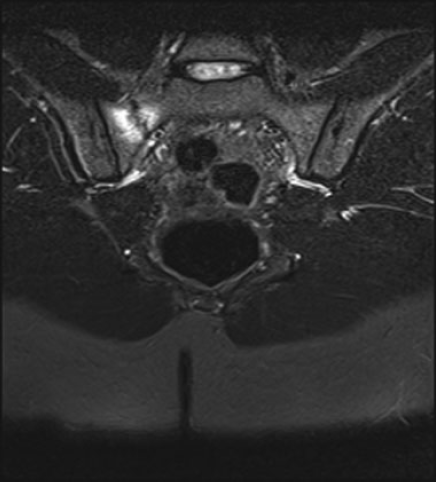
T2-weighted pelvis magnetic resonance image demonstrating the degree of bony edema surrounding the fracture line, which is parallel to the sacroiliac joint.
Discussion
Background
Stress fractures were first described in 1855 by the Prussian military surgeon Briethaupt who noted their occurrence among soldiers after long marches. 1 The classification system commonly employed today was proposed by Pentecost in 1964 and separates stress fractures into fatigue fractures and insufficiency fractures: Fatigue fractures occur in normal bone exposed to excessive stress loads, and insufficiency fractures occur in pathologic bone (e.g., osteoporotic) exposed to normal physiologic stress loads. 1 The first case of a sacral stress fracture was presented by Lourie in 1982, and since that time several other case reports have been published on the subject of both sacral insufficiency fractures (SIFs) and sacral fatigue fractures (SFFs). 1
In general, sacral stress fractures are uncommon injuries, and their true prevalence is unknown due to their frequent misdiagnosis, lack of specific symptoms, and successful resolution with time and observation. 2 However, SIFs are reportedly much more common than SFFs, with SIFs being almost exclusively reported in women over the age of 55 years. 3 SFFs, on the other hand, are relatively rare but have been documented in military personnel and athletes across a range of activities including running, basketball, soccer, volleyball, tennis, and hockey. 4 , 5 It is estimated that 0.5 to 2% of high-level athletes or military personnel will sustain a stress fracture during their careers, of which sacral fractures are estimated to account for less than 1.5% of all stress-fracture injuries. 5 , 6 , 7 Of course, the distinction between SFF and SIF is not always clear as fractures can occur secondary to normal physiologic loads in patients with normal bone densities; this is best demonstrated by reports of stress fractures in patients after lumbosacral arthrodesis as a form of adjacent segment disease and in postpartum women. 5 , 8 To our knowledge this is the first case report of an SFF sustained from horse-riding activities.
In general, the majority of equestrian-related injuries are due to falls from horses (75%), but other mechanisms have been described and include collisions, mounting or dismounting injuries, stirrup injuries, and saddle-horn injuries. 9 We performed a structured PubMed and Medline literature search using the terms “sacral,” “sacrum,” “stress fracture,” “fatigue fracture,” “equestrian,” and “horse-riding” in various combinations, and expanded the search using the “search-related” option. Only one other case of an equestrian-related stress fracture has been reported in a femur. 10 Of course, although equestrian activities are undoubtedly dangerous in the sense that riders are unrestrained, travel on unpredictable animals, and can reach speeds of over 60 km/h, studies have shown that ∼70% of injuries occur in recreational participants, with over 55% of cases presenting among first-time riders. 11 , 12 Interestingly, reports of lower back pain are relatively common among professional equestrians with 56% of riding instructors reporting lower back pain and female riders being affected twice as commonly as men. 13 , 14 For this reason, the diagnosis of a sacral stress fracture among healthy young horse riders can be easily missed or ignored.
Pathophysiology
Biomechanically, the sacrum is the keystone of the pelvic arch and functions to transfer and distribute upper torso loads across the pelvis toward the limbs. 15 The average sacral inclination is 41 degrees oblique to the horizontal and allows the spine to maintain a normal lumber lordosis to disperse axial stress loads into both compressive and shear forces; changes to the normal lumbar alignment while seated on horse saddles may convert these balanced forces to solely compressive or shear forces with excessive stress on the surrounding osteoligamentous structures. 4 Positional changes to the lumbar spine's alignment while seated may explain why lower back pain complaints were reportedly twice as common among users of traditional-style saddles compared with deep-seated saddles. 13 Furthermore, as the sacrum becomes increasingly overloaded during intense periods of training, its ability to repair microfractures becomes overwhelmed with eventual bony fatigue and a resulting frank fracture. 16 These factors may explain why women are more susceptible to sacral stress fractures than men; the gynecoid shape of their pelvises may be less efficient at distributing axial stress loads, their bones’ ability to remodel areas of microfractures may be compromised by generally lower dietary calcium intake, and their bones’ compressive strength and mineral density may be reduced due to a combination of hormonal and menstrual irregularities that are known to affect bone metabolism. 1 , 15 Regardless of mentioned gender issues, our patient's participation in the equestrian training program may represent a period of strenuous activity with excessive axial loads to her sacrum occurring during various gait forms (e.g., ambling or galloping) or training exercises (e.g., dismounting). Nevertheless, the bone mineral density scans were able to confirm that her injuries were of the fatigue fracture type and not related to fragility.
Diagnosis
A review by Kahanov et al found that ∼95% of patients with sacral stress fractures initially presented with lower back pain or buttock pain and that neurologic symptoms were an uncommon presenting complaint with radicular symptoms occurring in only 2% of cases. 17 , 18 Back pain symptoms are typically localized to one sacral area, worse with standing or activity, and relieved by rest or lying flat, and they may be associated with strenuous impact activities in cases of SFF. Although no physical examination features are specific to sacral stress fractures, findings include an antalgic gait, localized tenderness over the sacral paraspinal area, and positive clinical tests that include the Gaenslen test, squish test, or Patrick test. 17 If present, the commonest radiculopathies involve the S1 or S2 distribution. 19 Unfortunately, the differential diagnosis for lower back pain is extensive and includes musculoskeletal sprains, lumbar disk disease, facet arthropathy, sacroiliac joint pathologies, spondyloarthropathies, spondylolysis, spinal stenosis, and neoplasms. 17 , 20 Furthermore, complaints of back pain in association with radicular symptoms can easily distract the physician from the correct diagnosis and may explain why the majority of sacral stress fractures are typically not diagnosed until 4 weeks after the patient's initial presentation. 17
Therefore, a high index of suspicion should be raised when patients present with lower back pain with a background of significant risk factors. Risk factors include but were are not limited to acute changes in the frequency or intensity of a patient's normal activities, limb length discrepancies, factors associated with osteoporosis including the female athlete triad, corticosteroid therapy, rheumatoid arthritis, medications, postmenopausal state, nutritional deficiencies, hyperparathyroidism, osteomalacia, and sacral radiotherapy exposure. 1 , 5 , 6 Blood investigations may reveal abnormal electrolyte or hormone levels but are otherwise generally normal with mildly raised alkaline phosphatase levels. 1
Diagnostic imaging investigations provide the only reliable method for confirming a sacral stress fracture. Due to their relatively low cost and availability, plain radiographs are still considered the first line of imaging for suspected cases, and the fractures classically present as a vertical radiolucent line parallel to the sacroiliac joint with associated endosteal thickening or periosteal new bone formation. 16 , 19 However, due to surrounding anatomic structures and the timeframe necessary for a 30 to 50% change in trabecular bone density, a fracture line may not be easily detectable and therefore plain radiographs are generally not considered reliable for diagnosis. 20 In fact, the reported sensitivity rates for identifying sacral stress fractures have been 15% for plain radiographs, 88% for computed tomography scans, and 99% for MRI. 1 Bone scintigraphy scans have been shown to demonstrate an equally high sensitivity to MRI, 21 but they may be unreliable during the first 72 hours of symptom onset with the classic H or Honda sign described by Ries being found in only 20 to 32% of cases. 22 Otherwise, MRI is now considered the most appropriate tool for diagnosis with typical findings being a distinct low-signal fracture line surrounded by increased low-signal bone marrow edema on T1-weighted images and high signal intensity on T2-weighted images. 20 Currently, no radiographic classification systems specific to sacral fractures are described, and therefore the majority of published articles refer to the Denis classification, which separates sacral fractures into three zones based on their location relative to the sacral foramina. 23
Treatment and Prognosis
Currently, there are no established guidelines for the treatment of stress fractures, but conservative therapy with rest, pain control, and activity modification are generally successful. 24 If not already established, bone density investigations should be considered in all patients to confirm whether osteoporosis treatment should be initiated as well as help guide management and prognosis advice. 16 In general, patients with SFFs can gradually return to full activities once their symptoms have completely resolved. 5 Except for recurrences that have been attributed to a premature return to strenuous activities, no long-term complications have been reported, and patients with SFF can expect to return to their previous activity levels within 4 months of symptom onset. 2 Unlike SIF where some authors have recommended bed rest and symptoms require over 14 months to resolve, no cases have reported the need for surgical intervention. 15 , 24 Interestingly, some authors have recommended that patients with stress fracture avoid the use of nonsteroidal anti-inflammatory drugs due to their associated risk of delayed bone healing, as well as supplementing their nutritional intake with calcium and vitamin D oral supplements. 2 , 16 If indicated, osteoporosis medications should be initiated by a specialist who can select among the various compounds available including bisphosphonates, calcitonin, selective estrogen receptor modulators, and recombinant parathyroid hormone. 2 Furthermore, appropriate equipment changes should be recommended and include changes to footwear, terrain, or, in the case of our patient, saddle type. Educational training regarding correct posture and technique may help prevent injuries. Otherwise, no reports of surgical interventions have been published on SFF, but several cases of either sacroplasty or sacrokyphoplasty have been presented for the management of SIF. 15 , 25
Conclusion
Sacral stress fractures are rare presentations of lower back pain, and their prevalence among the general population is undocumented. They can be divided into sacral fatigue and SIFs, with implications to treatment and prognosis. We present the first reported case of an equestrian-related SFF in a woman presenting as lower back pain with radicular symptoms. Although sacral stress fractures are rare, the possibility should be considered in patients who present with lower back pain in the setting of a suggestive history with known risk factors. Ultimately, the diagnosis is radiographic with MRI being the preferred diagnostic tool and treatment is conservative with pain control, rest, and activity modification. Overall, patients with SFFs can expect a complete resolution of their symptoms within 4 months and a full return to their previous levels of activity thereafter.
Disclosures
Drew A. Bednar, none
Khaled Almansoori, none