
Abstract
Study Design
Retrospective cohort study.
Objective
To compare sagittal cervical range of motion (ROM) and alignment in young versus middle-aged adults.
Methods
One hundred four asymptomatic adults were selected randomly out of 791 subjects who underwent lateral cervical radiographs in neutral, flexion, and extension positions. They were divided into two groups: young (age 20 to 29, 52 people) and middle-aged adults (age 50 to 59, 52 people). We determined the ROMs of upper cervical (occipital–C2 angle), midcervical (C2–C7 angle), and cervicothoracic spine (cervicosternal angle). We compared the alignment differences of the two groups by calculating the distances between C2 and C7 plumb lines, and C2 central-offset distance.
Results
In neutral position, there was no significant difference between young and middle-aged adults. However, in flexion, C2–C7 angle, distance between C2–C7 plumb lines, and C2 central-offset distance decreased with age. In extension, C2–C7 angle and C2 central-offset distance decreased with age. During flexion and extension, midcervical ROM and the range of C2 central-offset distance decreased in the middle-aged group. However, there was no difference between the two age groups in the ROM of the upper cervical and the cervicothoracic regions during flexion and extension.
Conclusion
We found that, despite of the presence of age-related cervical alignment changes, the only difference between the two groups was in the sagittal ROM of the midcervical spine during flexion and extension. Only the ROM of the midcervical spine appears to change significantly, consistent with findings that these levels are most likely to develop both symptomatic and asymptomatic degenerative changes.
Introduction
The sagittal cervical range of motion (ROM) in healthy adults is between 117 and 140 degrees by quantitative motion analysis. 1 , 2 , 3 With aging, cervical ROM declines in all primary planes. 4 , 5 , 6 , 7 , 8 Cervical sagittal ROM is composed of upper cervical ROM (occipital [Oc]–C2 angle), lower cervical ROM (C2–C7 angle), and ROM between the cervical spine and chest (cervicosternal angle). 7 , 9 , 10 , 11 In a cervical dynamic radiographic study, 1,230 asymptomatic volunteers were found to have a lower cervical ROM of 67.7 ± 17.0 degrees in the third decade, which decreased to 45.0 ± 12.5 degrees in the eighth decade. 7 In other studies, C2–C7 plumb line distances were reported to be distributed in a narrow range. 12 , 13 The C7 plumb line shows the sagittal alignment of the thoracic and lumbar spine and moves forward with aging. 14 The sagittal alignment by C2 and C7 plumb lines shows the sagittal alignment of the cervical spine and is maintained with aging. 15 However, to our knowledge, there has been no report regarding changes to the upper cervical and cervicosternal ROM and only one article regarding to the sagittal alignment by C2 and C7 plumb lines in older people. 15 The purpose of this study is to investigate the age-related changes in the sagittal ROM of the cervical spine and the sagittal alignment by C2 and C7 plumb lines.
Materials and Methods
Patient Recruitment
Seven hundred ninety-one healthy asymptomatic adults underwent neutral and dynamic cervical radiographs from January 2009 to December 2011. They visited our clinic because of back pain. They had no symptoms and signs correlated to the cervical spine. The cervical and lumbar spines were evaluated together voluntarily. A total of 104 asymptomatic adults were selected randomly out of the 791 healthy adults for the current study using a random number generator, and their information was blinded to the selecting researcher. The exclusion criteria included those with previous history of cervical trauma or operations. They were composed of people in their 20s (20 to 29 years) and 50s (50 to 59 years). The young group (20s) contained a total 52 people (16 men, 36 women), and the middle-aged group (50s) was composed of 52 people (14 men, 38 women). Mean age was 24.8 ± 3.1 years old in young group and 53.4 ± 2.9 years old in the middle-aged group. The mean body mass index (BMI) of young group and middle-aged group was 22.8 ± 3.6 kg/m2 and 23.6 ± 2.4 kg/m2, respectively. The sex and mean BMI were not significantly different between the two groups (p > 0.05). Institutional board approval was obtained before initiating this study, and an approved informed consent form was signed by all patients who were enrolled.
Measurement of Radiographic Parameters
All patients had cervical spine lateral radiographs in neutral, flexion, and extension positions. The images were obtained with the patients standing and looking straight ahead. Lateral radiographs were performed using standard radiographic techniques wherein the tube was centered on the C3–4 intervertebral disk. We confirmed the true lateral image of thoracic vertebral body to show the anterior edge of sternal manubrium and prevent sternal rotation. The radiographic film cassette was 72 inches from the tube, and radiographs were taken without magnification. The digital X-ray images were obtained on the PACS system (Π view, Infinitt, Seoul, Korea), which was used to obtain measurements related to alignment. We chose lordotic curves to be expressed as negative values and kyphotic curves were given positive values. Four standard lines were made on the neutral lateral radiographs that were obtained as follows: line A represented the McGregor line, from the hard palate to the inferior edge of the occiput; line B represented the inferior end plate of the axis; line C represented the inferior end plate of C7; line D represented the anterior edge of the sternal manubrium (Fig. 1). The angles formed between the following lines were measured: A to B (representing the Oc–C2 angle), B to C (representing the C2–C7 angle), and C to D (representing the cervicosternal angle; Fig. 1). We measured the distances between the C2 and C7 plumb lines, as well as the C2 central-offset distance. C2 and C7 plumb lines were defined, respectively, as a vertical line from the center of the second and seventh cervical vertebral bodies (diagonal contact point, Fig. 2). C2 central-offset distance is the perpendicular distance between the center of the C2 vertebral body and a line extended from the C7 posterior vertebral border (Fig. 3). We arbitrarily assigned a positive value when the upper of two parameters was located anterior to the lower one on the lateral views. For example, if the center of the C2 vertebral body was anterior to the line extended from the C7 posterior vertebral border, the parameter was a positive value. We compared the two age groups for all of the previously listed radiologic parameters. Two experienced spine surgeons measured each of the radiographs on two separate occasions separated by 1 month.
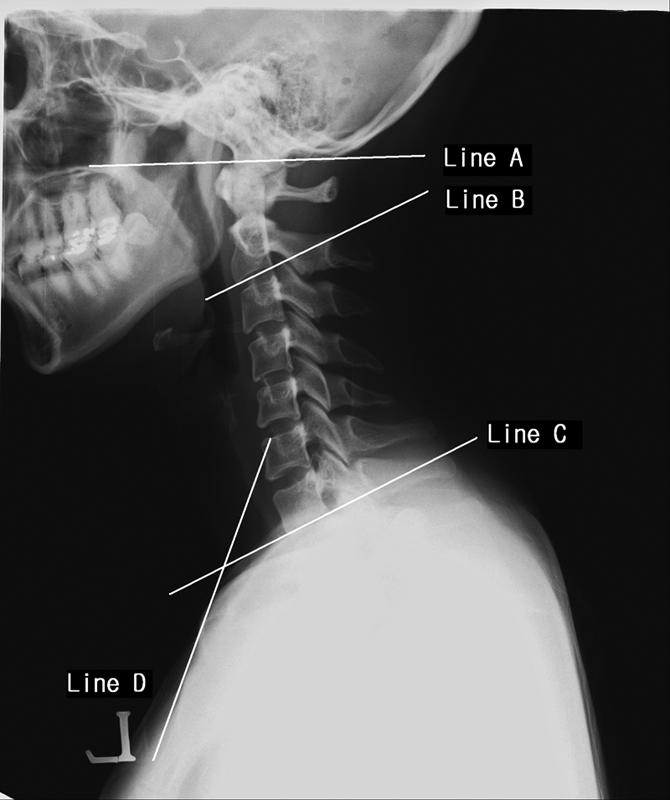
McGregor line was measured from the hard palate to the inferior edge of the occiput (line A); the inferior end plate of the axis (line B); the inferior end plate of C7 (Line C); the anterior edge of sternal manubrium (line D).

Distance between the C2 and C7 plumb lines. Plumb line was defined as the vertical line from the center of cervical spinal vertebral body (diagonal contact point).
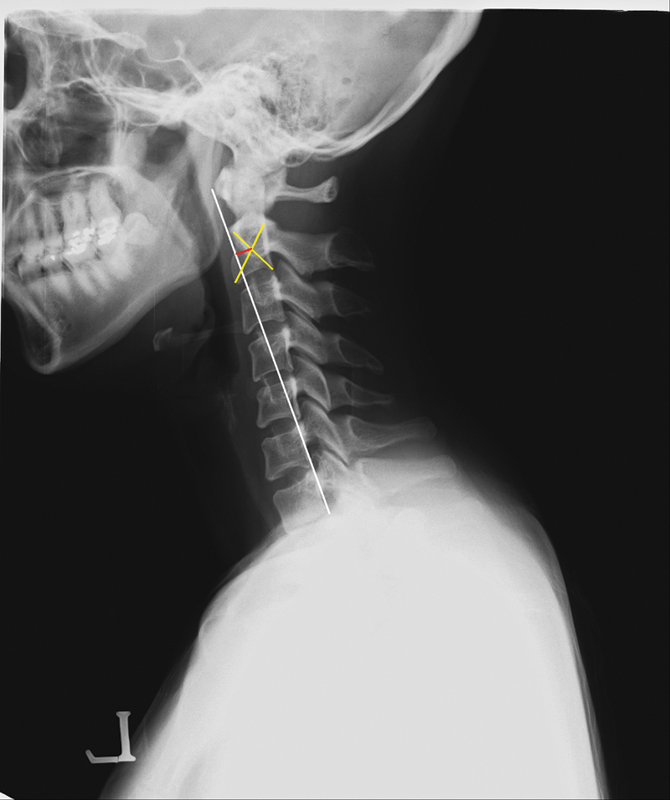
C2 central-offset distance is the distance from the center of C2 vertebral body (diagonal contact point) to the extension line from the C7 posterior border.
Statistical Methods
We analyzed data statistically with SPSS version 13.0 for Windows (Chicago, Illinois, United States). To determine the difference of the two groups in sagittal cervical spinal ROM, unpaired t tests were used. Power analysis was performed by G*Power version 3.1.5 (Universität Kiel, Germany). Power was 0.95 for unpaired t tests with the effect size of 0.8. The sample size in each group should be more than 42. The statistical significance level was set at p < 0.05. The intraobserver and interobserver reliabilities were calculated using the reliability statistics by intraclass correlation (ICC) for the Cobb angle and the distance. The ICC values were graded using previously described semiquantitative criteria: excellent for values in the 0.9 to 1.0 range, good for 0.7 to 0.89, fair/moderate for 0.50 to 0.69, low for 0.25 to 0.49, and poor for 0.0 to 0.24.
Results
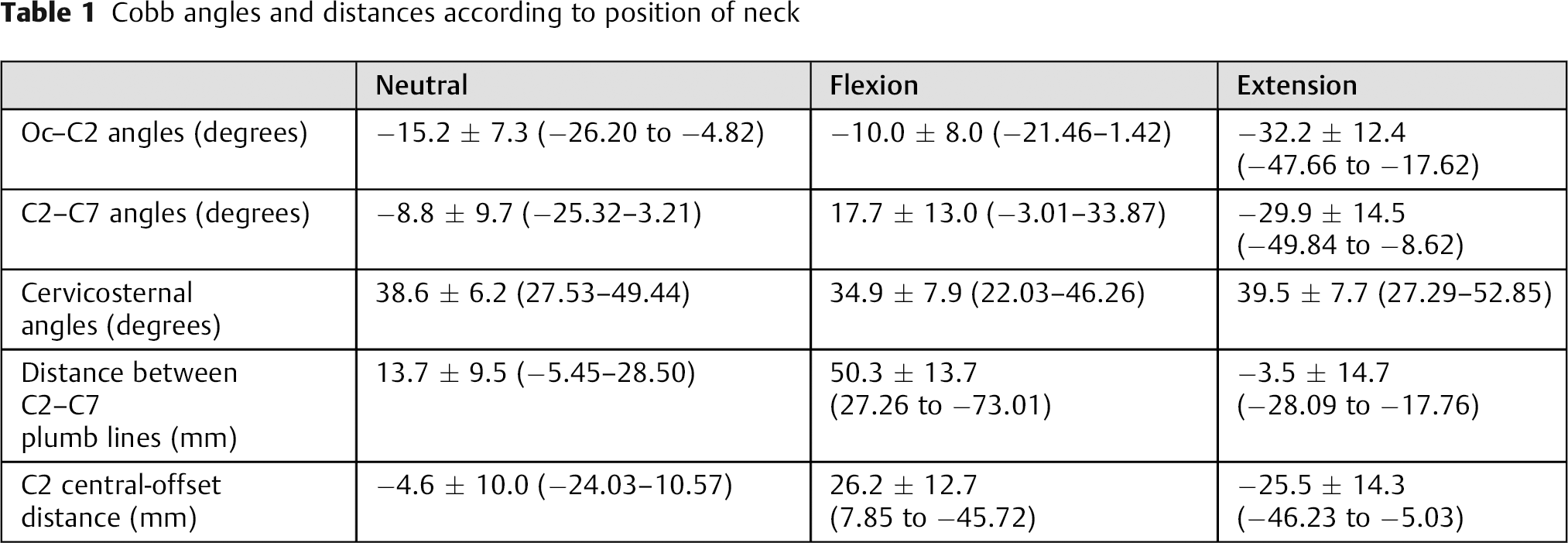
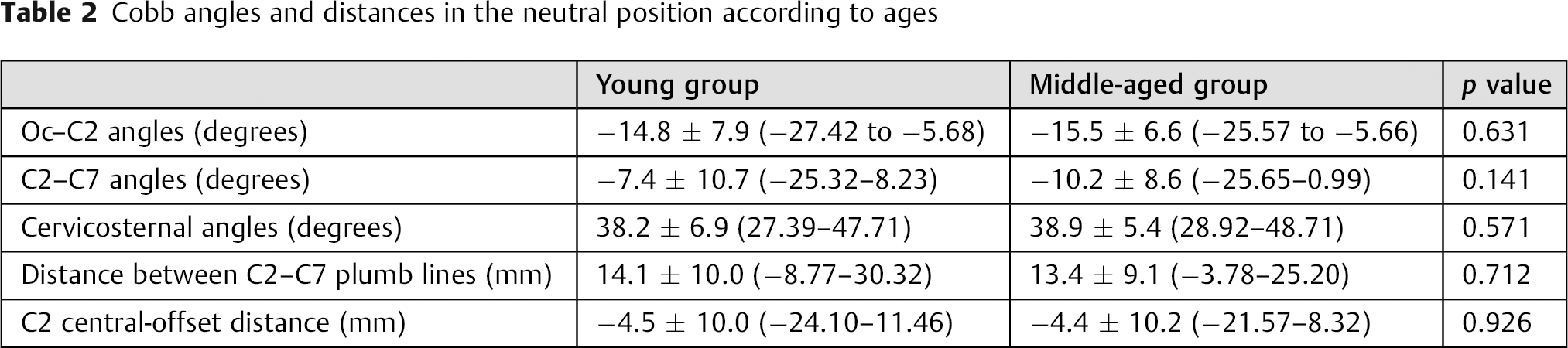
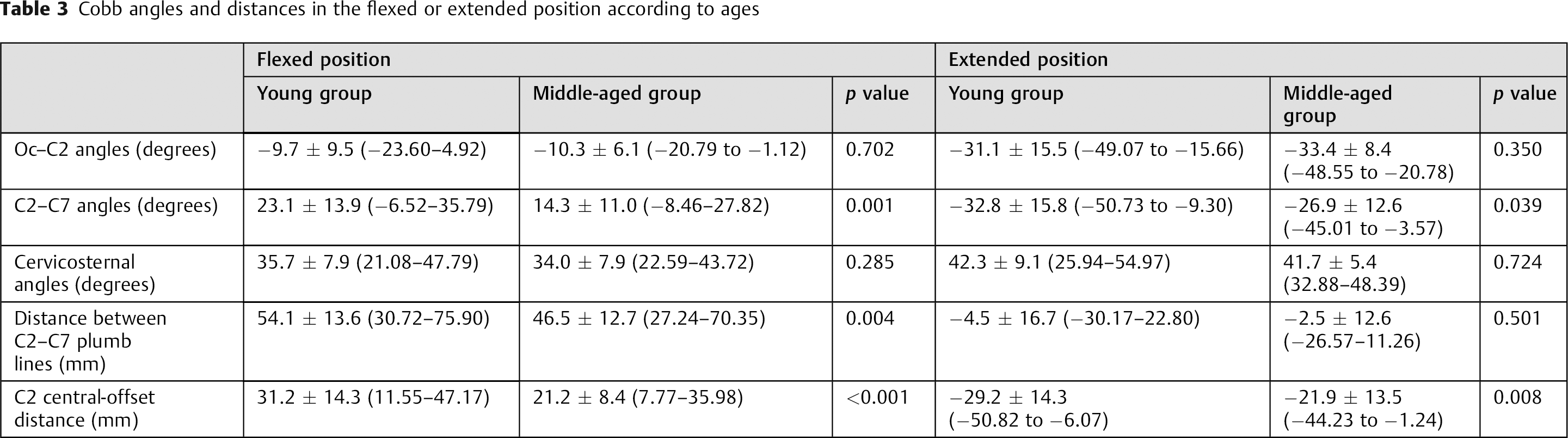
The Oc–C2 angle, C2–C7 angle, cervicosternal angle, C2–C7 plumb line distance, and C2 central-offset distance were measured in neutral, flexion, and extension positions (Table 1). In the neutral position, there was no significant difference between the young and middle-aged groups in all measured values (Table 2). However, in the flexed position, the C2–C7 angle, the distance between the C2–C7 plumb lines, and the C2 central-offset distance were lower in the middle-aged group (Table 3). In the extended position, the C2–C7 angle and the C2 central-offset distance were lower in the middle-aged group (Table 3). During flexion and extension, the lower cervical ROM, as defined by the C2–C7 angle, and the range of variation of the C2 central-offset distances were lower in the middle-aged group (Table 4). However, there was no difference between the two age groups in the upper cervical ROM, as measured by the Oc–C2 angle. Likewise, there was no difference between the two groups for ROM measured by the cervicosternal angle during flexion and extension. During flexion, the range of variation in the distance between the C2–C7 plumb lines was lower in the middle-aged group, whereas there was no difference between the two groups during extension (Table 4). The reliability statistics by ICC for the Cobb angle showed the 0.979 for the intraobserver reliability and 0.966 for interobserver reliability. The reliability statistics using ICC for the distance resulted in 0.978 for the intraobserver reliability and 0.926 for interobserver reliability.
Cobb angles and distances according to position of neck
Cobb angles and distances in the neutral position according to ages
Cobb angles and distances in the flexed or extended position according to ages
ROM and variation of distances from neutral to flexed or extended positions according to ages

Abbreviation: ROM, range of motion.
Discussion
There is general agreement in the literature that the ROM of the cervical spine decreases with increasing age. 4 , 5 , 6 , 7 , 8 Cervical sagittal ROM is composed of upper cervical and lower cervical ROM between the cervical spine and chest (cervicosternal angle). 7 , 9 , 10 , 11 Also C2–C7 plumb line distances were reported to be distributed in a narrow range 12 , 13 and maintained with aging. 15 However, there are only two articles regarding the changes in lower cervical ROM in older adults, 7 , 8 and there has been no report regarding the changes in the upper cervical and cervicosternal ROM, as well as sagittal alignment measured by C2 and C7 plumb lines. The purpose of this study is to investigate the age-related changes in the sagittal ROM of the cervical spine and the sagittal alignment using C2 and C7 plumb lines.
In the current study, there was no significant difference between the young and middle-aged groups in the Oc–C2 angle, C2–C7 angle, cervicosternal angle, C2–C7 plumb line distance, and C2 central-offset distance in the neutral position. During the flexion and extension of neck from the neutral position, the lower cervical ROM by C2–C7 angle decreased more in the middle-aged group. However, for upper cervical ROM and the ROM by cervicosternal angle, there was no difference between the young and middle-aged groups. This means that with age, decreased ROM is limited in C2–C7 region.
Matsunaga et al measured the Oc–C2 angle between the McGregor line and the inferior aspect of the axis in the neutral radiographs of 240 asymptomatic individuals (120 men and 120 women) who were divided into six groups of 40 members each, ranging in age from the third to the eighth decade, and showed that the Oc–C2 angles gradually decreased with age after 40 years old. 11 The other studies by neutral cervical radiographs of the asymptomatic volunteers showed that the Oc–C2 angle (McGregor line) decreased and the C2–C7 angle increased with aging and the Oc–C2 angle had strong correlation with the C2–C7 angle. 9 , 10 In another radiologic study of 1,230 asymptomatic volunteers who underwent cervical radiographs with neutral position, the C2–C7 lordotic angle was 8.0 ± 11.8 degrees in the third decade and increased to 19.7 ± 11.3 degrees in the eighth decade. 7 These results are discordant with the current study. It might be explained by the fact that their studies included participants of different ages than the current study. They included people between 12 and 80 years of age in their studies, 7 , 9 , 11 and we randomly selected people in their 20s and 50s. In addition, radiographs were taken differently in their studies. The individuals underwent cervical lateral radiograph while sitting on a stool with film-tube distance of 1.5 m 9 , 10 or standing with film-tube distance of 1.5 m, 7 and the subjects underwent cervical lateral radiograph while standing and film-tube distance was set at 1.8 m in the current study. In another study of 100 healthy unoperated adults who were free of spinal problems and underwent whole-spine standing radiographs, the subjects consisted of two groups divided by age: those in their 20s and those above 60. 15 The Oc–C2 angle was maintained but the C2–C7 angle increased in the old group compared with the young group. 15 The maintained Oc–C2 angle is concordant with the current study. There are controversies regarding the changes of Oc–C2 angle and C2–C7 angle with aging. It might be explained by the fact that the radiographs were taken differently than those in the current study. In that study, all individuals underwent cervical lateral radiograph while sitting on a stool with film-tube distance set at 1.5 m, 9 , 10 cervical lateral radiograph while standing with film-tube distance set at 1.5 m, 7 or whole-spine standing radiographs, 15 but in the current study, the subjects underwent cervical lateral radiograph while standing and film-tube distance was set at 1.8 m.
Similarly, in the current study, radiologic study of cervical dynamic radiographs of 1,230 asymptomatic volunteers showed that the C2–C7 ROM was 63.9 ± 15.6 degrees in men in their 20s (20 to 29 years) and decreased to 48.7 ± 12.0 degrees in men in their 50s (50 to 59 years). 7 In the women, the C2–C7 ROM was 71.6 ± 17.5 degrees in the subjects in their 20s and decreased to 55.1 ± 12.8 degrees in the subjects in their 50s. 7 However, there has been no report regarding aging changes in the upper cervical and cervicosternal ROM, though upper cervical angle in the neutral radiograph has been evaluated with respect to aging. 9 , 10 , 11 , 15 The upper cervical ROM by Oc–C2 angle and the ROM by cervicosternal angle during flexion and extension were maintained in the middle-aged group of the current study. Perhaps because the Oc–C2 region has no disk that can degenerate, it appears to be relatively well preserved in middle age. The cervicothoracic spinal junction, for unclear reasons, also appears to maintain its ROM and alignment in middle age.
The cervical plumb lines from the odontoid to C2 for all 100 volunteers were distributed in a narrow range (16.1 ± 11.6 mm) anterior to the center of C7. 12 C2 and C7 sagittal plumb line was maintained with a narrow range of variation of 40 mm. 13 In the current study, there was no significant difference between young and middle-aged groups for the C2–C7 plumb line distance in the neutral position. However, during the flexion of neck, the range of variation of the distance between C2–C7 plumb line decreased in the middle-aged group but was not different between two groups during extension.
As with other studies, the present investigation has several limitations. It is a retrospective study. Our study could be improved with a prospective study of volunteers who take cervical dynamic radiographs. Second, the grade of degeneration should be compared and the difference in ROM between the young and middle-aged groups explained. Unfortunately, it was difficult to compare the degeneration in the upper cervical spine (Oc–C2) with that in the lower cervical spine (C2–C7) because there is no intervertebral disk in the upper cervical spine. Third, it is a selection bias to place subjects into two dichotomous age categories. It would be a better study if we included subjects of all ages, including patients older than 70 years old. If we include subjects of all ages to the study population, we may get results similar to the previous studies about the sagittal cervical alignments by Oc–C2 angle and C2–C7 angle. 7 , 9 , 10 , 11 However, as far as we know, this represents the first and the largest set of normative data on asymptomatic subjects in both young and middle-aged groups for the cervical ROM, especially by the upper cervical angle and cervicosternal angle.
We found that only the ROM of the midcervical spine decreased significantly with aging, consistent with findings that these levels are most likely to develop both symptomatic and asymptomatic degenerative changes. Older people with the lower cervical spines fused congenitally or patients with those fused surgically can flex or extend their necks by the preserved motion of upper cervical spine and cervicosternal junction. It is imperative that surgeons be aware of this during surgical fusion extended to the upper cervical spine and cervicothoracic junction in older people. Our study could provide the information that the cervical ROMs by upper cervical angle and cervicosternal angle are important to the life of older people. Surgeons do not need to adhere to arthroplasty of the midcervical spine instead of cervical fusion in middle-aged patients, considering the decreased midcervical ROM in the middle-aged people.
Disclosures
No funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this article.