
Abstract
Background
Osteochondroma is the most common primary bone tumor, composing 35% of benign bone tumors and 9% of all bone tumors; 1.3 to 4.1% of all osteochondromas originate from the spine. A rare differential diagnosis for globus symptoms is an osteochondroma originating from the anterior surface of the axis. We describe a rare case of osteochondroma of the dens resulting in “globus symptoms” (the subjective sensation of a mass in the throat) treated with excision via the high cervical extrapharyngeal approach.
Purpose
To discuss the surgical management of this problem, with an emphasis on surgical approach used. The clinical history, examination, and investigations are presented and illustrated, along with clinical patient outcome.
Study Design/Setting
This article is a case report of a patient treated at the Department of Trauma and Orthopaedics in an active university teaching hospital.
Methods
Case presentation. For the discussion, we used handpicked articles, as well as MEDLINE and PubMed database searches with the keywords “C2,” “dens,” “osteochondroma,” “globus,” “extrapharyngeal approach.”
Results
Uncomplicated procedure. Histological analysis confirmed a benign osteochondroma with no evidence of malignancy. The patient underwent an uncomplicated postoperative recovery and was discharged 24 hours after surgery, fully ambulatory and eating and drinking well.
Conclusions
The high cervical retropharyngeal approach is safe and reproducible for the excision of osteochondromas or osteophytes of the upper cervical spine.
We describe a rare case of osteochondroma of the dens resulting in “globus symptoms” (the subjective sensation of a mass in the throat) treated with excision via the high cervical extrapharyngeal approach.
Case Report
A 65-year-old man presented with a 2-month history of “something stuck” in his throat. In the subsequent 2 years, these evolved to mainly respiratory symptoms, nasal congestion, intermittent breathing difficulty, snoring, dysphagia with a subjective sensation of food lodging in the larynx, and regurgitation of food contents 1 hour following ingestion. There were no other symptoms on systems review. He had a past medical history of benign prostatic hypertrophy, stable angina, and gastroesophageal reflux disease. There was no significant family history of disease. Clinically, no masses or lymphadenopathy could be palpated in the neck. No focal neurological deficit was found on testing cranial or peripheral nerves. Laboratory values full blood count, urea and electrolytes, liver function tests, and inflammatory markers were all within normal limits.
Further evaluation by ear, nose, and throat surgeons and flexible nasoendoscopy showed a bony hard, smooth, and immobile visible mass lesion at the oropharynx (Fig. 1).
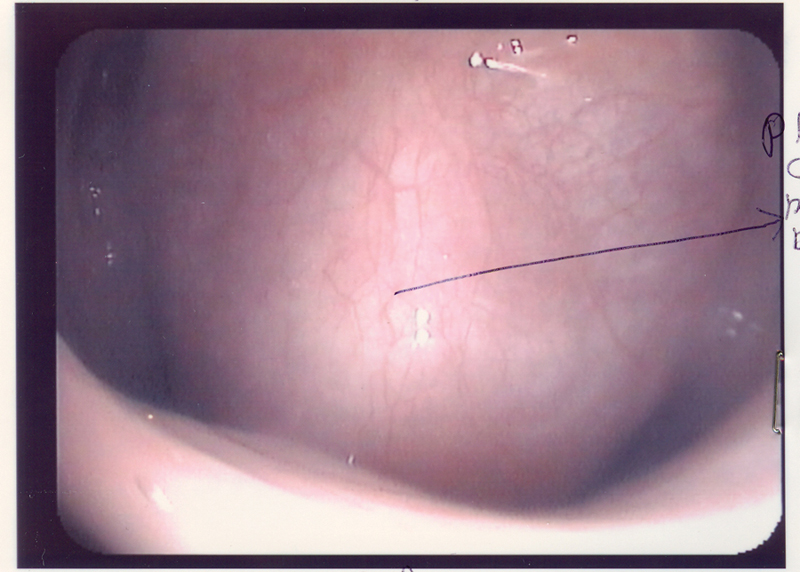
Flexible nasoendoscopic view showing a bony hard, smooth, and immobile visible mass lesion at the oropharynx.
X-ray showed a radiopaque round mass lesion arising from the body of the axis (Fig. 2). Computed tomography (Fig. 3) and magnetic resonance imaging (Fig. 4) showed an osseous outgrowth that was continuous with the anterior cortex of the body of C2. The appearances were characteristic of benign osteochondroma that projected forward and caused pressure on the esophagus.

X-ray appearance.
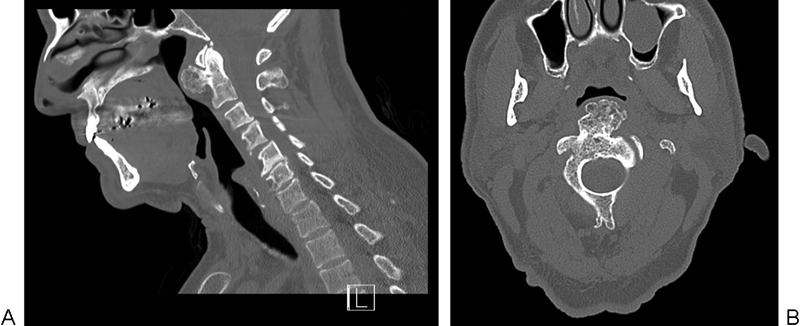
Computed tomography scan appearance (sagittal and axial views).
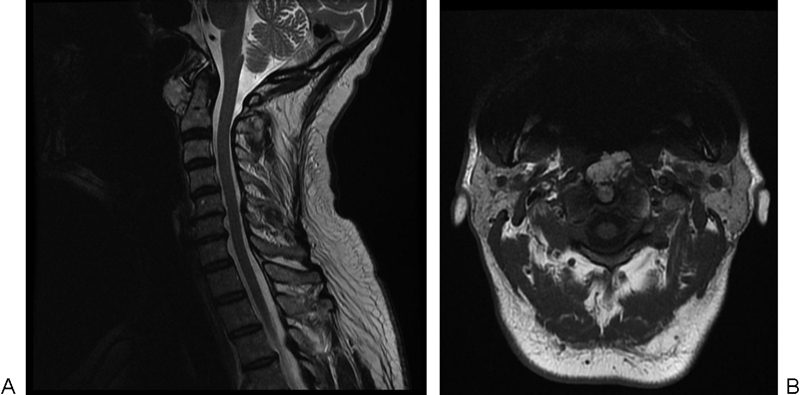
Magnetic resonance image appearance (sagittal and axial views).
Surgical Excision and Postoperative Recovery
The patient was positioned supine with the head tilted toward the right. The left extrapharyngeal approach was used by the spinal surgeon in conjunction with a plastic surgeon, starting with a curvilinear incision 1 inch below the palpable border of the mandible.
Careful dissection continued to isolate carotid sheath and neurovascular bundle. A plane was developed behind the jugular vein and down to prevertebral fascia. The carotid vessels were retracted medially and the posterior belly of digastric muscle retracted superiorly. The hypoglossal and superior laryngeal nerves were visualized and protected. The level of the osteochondroma was confirmed using image intensifier. The 6.5 × 5 × 5-cm osteochondroma was removed with osteotomes and bone wax applied to bleeding surfaces (Figs. 5, 6, 7).

Skin markings for incision below the border of mandible.
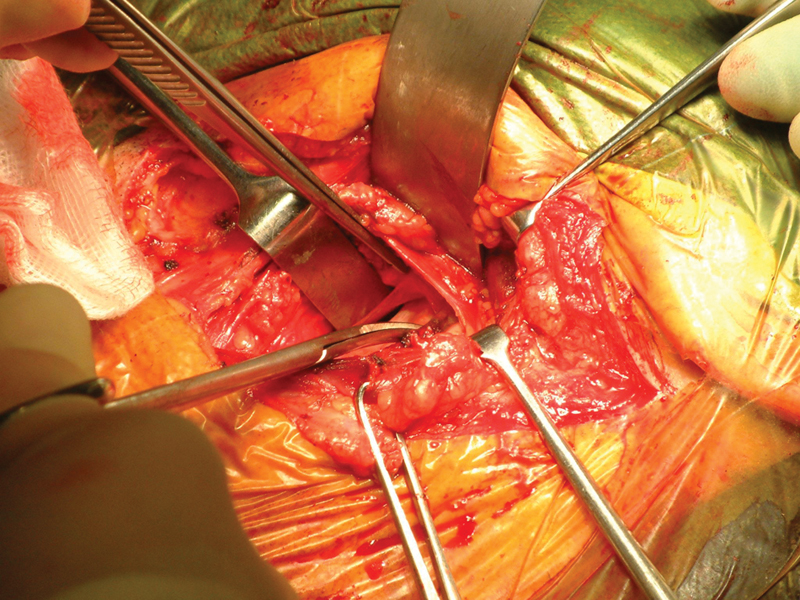
Dissection while protecting vital structures like hypoglossal nerve.
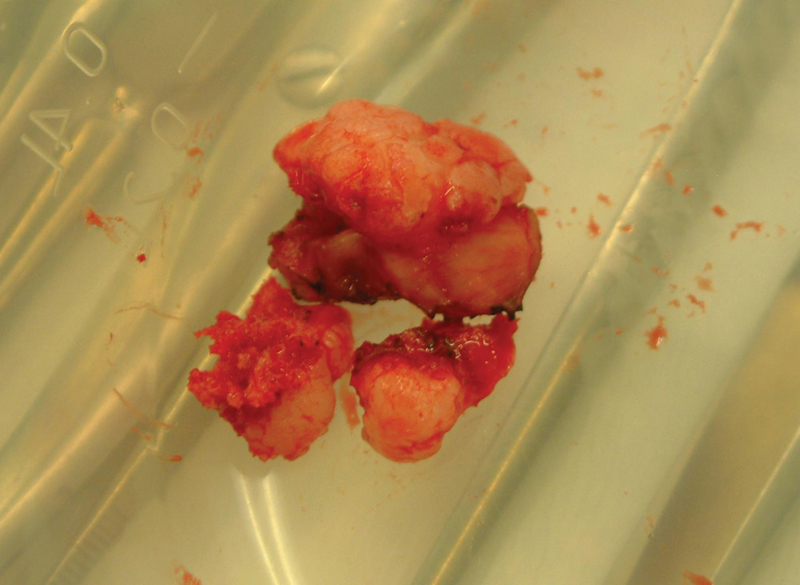
Excised osteochondroma.
Histological analysis confirmed this to be a benign osteochondroma with no evidence of malignancy. The patient underwent an uncomplicated postoperative recovery and was discharged 24 hours after surgery, fully ambulatory and eating and drinking well.
Discussion
Ear, nose, and throat surgeons use the term globus symptoms to describe the subjective sensation of a mass felt in the throat. A rare differential diagnosis for globus symptoms is an osteochondroma originating from the anterior surface of the axis. The globus sensation itself comes with a high lifetime incidence (46%), 1 although the proportion of people to which the symptom can be attributed to bony tumors or osteophytes is not yet known.
Osteochondroma is the most common primary bone tumor, composing 35% of benign bone tumors and 9% of all bone tumors 2 ; 1.3 to 4.1% of all osteochondromas originate from the spine. 3 In a literature review by Lotfinia et al, 4 24.24% of cervical spine osteochondromas arise from C2, 18.83% from C1, and 15.15% at the C7.
The potential for sarcomatous change of osteochondromas has been found to be four cases in 150 cases of solitary osteochondroma in the spine (i.e., 2.7%). 5 Given this rarity, its prophylactic excision in asymptomatic individuals may not be fully justified in a high-risk region such as the cervical spine. An excision becomes eminent when symptoms are severe and progressive.
Various options with regards to an approach to the dens include the following (Table 1): a transoral approach, a transnasal endoscopic approach, or high cervical extrapharyngeal or retropharyngeal approach
Benefits and drawbacks of various surgical approaches to the dens
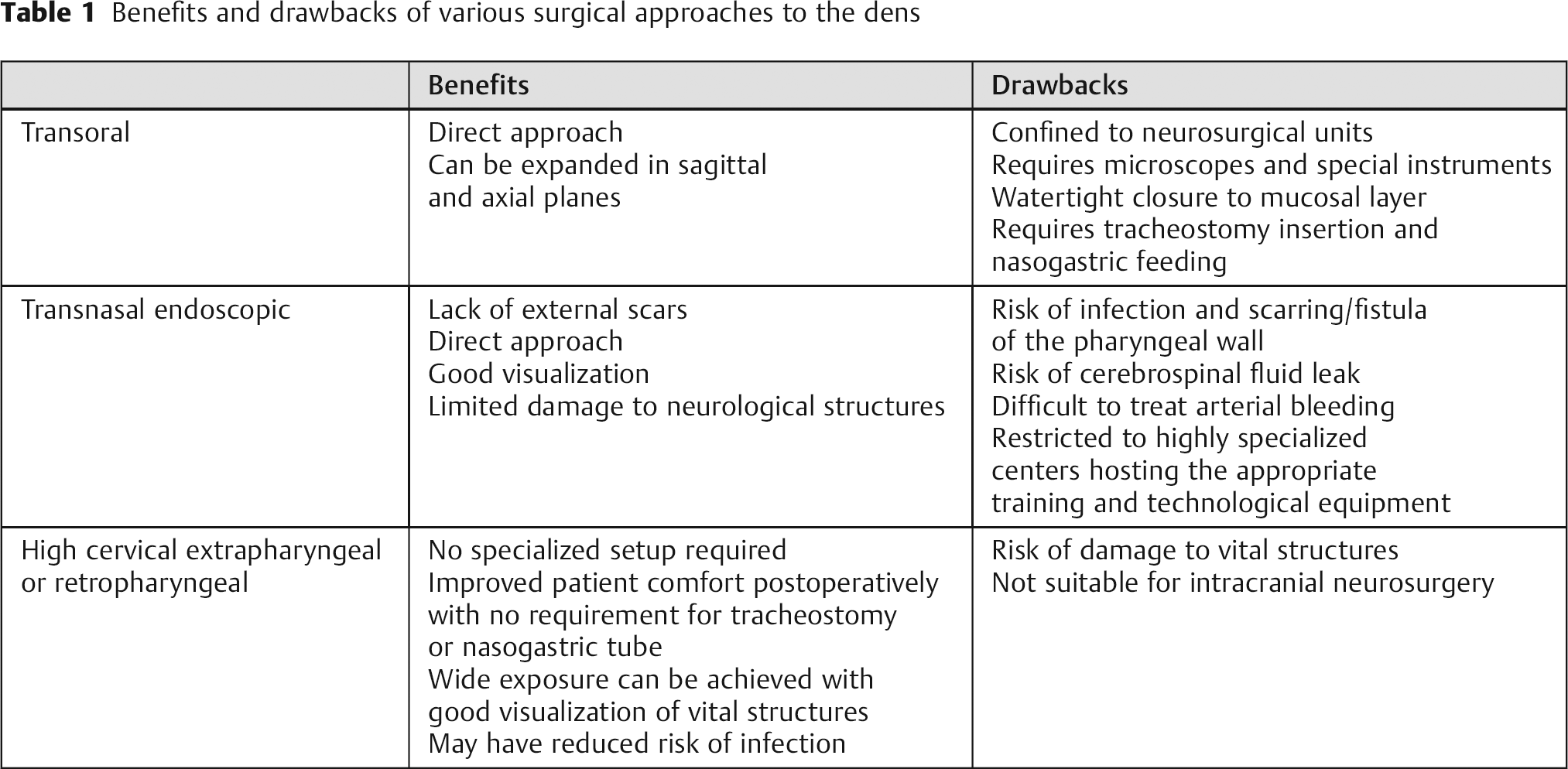
The transoral approach is confined to neurosurgical units. It does require expertise of access surgeons, microscopes, and special instruments. Attention must be made to ensure a watertight closure to the final mucosal layer. 6 It also necessitates tracheostomy insertion and a period of nasogastric feeding to allow the pharyngeal wall to heal.
The transnasal endoscopic approach is being used in highly specialized centers hosting the appropriate training and technological equipment. The possibilities, safety, and limits of this approach are still under investigation. 7 Both of the above approaches are associated with risk of infection and scarring/fistula of pharyngeal wall.
The high cervical retropharyngeal approach does not require a specialized setup. The approach can safely be undertaken by experienced spine surgeons or with the help of either head and neck or plastic surgeons. One can achieve a wide exposure from the basiocciput of clivus and anterior rim of the foramen magnum to the rostral cervical spine up to C4, to deal with a variety of pathology and fixation. Although there is a risk of damage to vital structures like marginal branch of the facial nerve, superior laryngeal nerve, hypoglossal nerve, superior thyroid artery, lingual artery, facial artery, and external carotid artery, they can be visualized and carefully protected under direct vision. 8 , 9
Traditional description of the approach to cervical spine suggests retracting carotid sheath contents laterally. We suggest retracting the carotid sheath contents medially, which minimizes the risk of brisk bleeding from common facial vein and tributaries. Also, this avoids the need for extensive dissection and ligation of rather big veins.
Benefits compared with direct transoral/transmucosal approach include improving patient comfort postoperatively and obviating the need for tracheostomy or nasogastric feeding and for median labiomandibular glossotomy where greater access may be required. The risk of infection may also be reduced. 8
Summary
Osteochondromas are rare bone tumors that may occur in the cervical spine and their excision is recommended if the patient is symptomatic. The high cervical retropharyngeal approach is safe and reproducible for the excision of osteochondromas or osteophytes of the upper cervical spine.
Disclosures
Ken Wong, None
Shaishav Bhagat, None
Jonothan Clibbon, None
A. S. Rai, None