
Abstract
Introduction
Interspinous motion preservation technique for various spondylotic conditions has been supposed to be useful as a time-sparing technique before rigid instrumentation with a potential secondary surgery for adjacent segment disruptions. But clinical results of various devices manufactured on the ideal concepts should not clearly make the idea successful or sometimes showed negative result.1.2 We review several reports on interspinous motion preservation devices (ISDs) and find a clue for the reasons of poorly functioned devices. We are tried to analyze the anatomical characteristics of lumbar spinous process based on lumbar CT's and suggest the neglected points in clinical application of the ISDs.
Materials and Methods
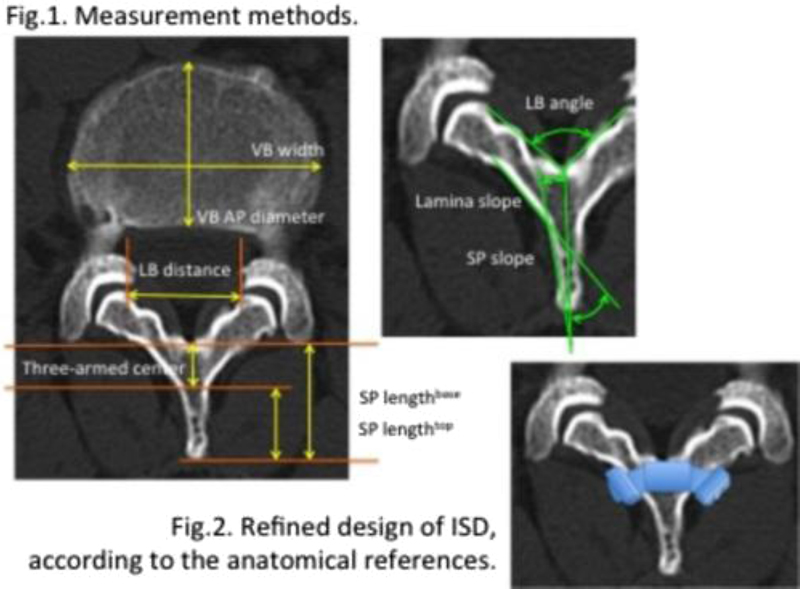
We analyzed the radiographic anatomical findings of lumbar spinous processes on CTs of the 120 vertebral bodies of 40 patients (male 20, female 20), aged 50∼65 years old. L2.34 spinous processes (SPs) and lamina were analyzed because ISDs can be mostly applied into the one or more of L 2-3, 3-4, 4-5 interspinous spaces. Lamina base (LB) distance (the shortest straight distance between medial facet ends in the spinal canal), LB angle (the angle between the lamina medial surfaces), lamina slope (the slope angle of a lamina to a center axis of spinous process), SP length top (the length of SP from a tip to the level of a junction of SP and lamina), SP length base (the length of SP from a tip to the level of a base surface of spinal canal), three-armed center area (the cross-meeting area of two laminas and a spinous process,= SP length base- SP length top), and SP slope (the slope angle of a SP surface to a center axis of spinous process) were measured on PACS system.
Results
LB distances were 16.8 ± 2.2 mm (L2), 21.0 ± 3.3 mm (L3), 21.4 ± 3.3 mm (L4) in female patients, and 19.3 ± 2.4 mm (L2), 19.6 ± 2.2 mm (L3), 22.2 ± 4.7 mm (L4) in male patients. LB angles were 83.8 ± 12.6° (L2), 88.1 ± 14.2° (L3), 83.4 ± 14.1° (L4) in female patients and 91.8 ± 11.0° (L2), 95.8 ± 15.0° (L3), 95.6 ± 17.3° (L4) in male patients. Lamina slopes were 34.2 ± 11.5° (L2), 36.5 ± 11.0° (L3), 41.1 ± 7.2° (L4) in female and 36.8 ± 6.3° (L2), 34.6 ± 7.1° (L3), 35.4 ± 5.2° (L4) in male patients. The differences according to sex at each level were not statistically significant (p = 0.287). SP length top were 17.6 ± 2.4 mm (L2), 17.8 ± 2.3 mm (L3), 17.4 ± 3.0 mm (L4) in female and 20.5 ± 3.3 (L2), 20.2 ± 3.3 mm (L3), 19.6 ± 3.3 mm (L4) in male patients. SP length base were 24.7 ± 3.0 mm (L2), 25.7 ± 2.3 mm (L3), 24.5 ± 5.0 mm (L4) in female patients and 28.3 ± 3.2(L2), 28.3 ± 3.4 mm (L3), 27.7 ± 3.4 mm (L4) in male patients. Three-armed center areas were 7.1 ± 1.9 mm (L2), 8.0 ± 1.4 mm (L3), 7.1 ± 1.9 mm (L4) in female patients and 7.8 ± 1.5 (L2), 8.1 ± 1.5 mm (L3), 8.1 ± 1.5 mm (L4) in male patients. The differences according to sex at each level were not statistically significant (p = 0.112). SP slopes were 3.8 ± 4.4° (L2), 4.9 ± 4.1° (L3), 5.4 ± 4.8° (L4) in female patients and 3.4 ± 3.7° (L2), 3.7 ± 4.1° (L3), 3.8 ± 5.1° (L4) in female patients.
Conclusion
ISDs were applied in interspinous space to support the SP itself to decrease the stress on the compromised vertebral disc and facet joints. But unfolding interspinous space at further posterior point, far more stress could generate anteriorly by a lever effect, resulting in vertebral body tilt anteriorly rather than straight lifting. Three-armed center area may be a center of a lever, lifting the body with less tilt of the vertebral body or segmental kyphosis. Under-support type devices(DIAM. Coflex) support the spinous portion directly and maintain their stability with unfolding SP. Wing-type devices(Wallis, X-stop, etc.) maintain them with holding SP over by side wings. If under-support type devices were not located just on the three-armed center area, its initial size would be bigger to support tightly interspinous space at further posterior site and make the segment kyphosis, which could give more stress on a compromised disc rather as the disc degeneration progressed (lever effect). When an anterior margin of a wing in classic designed devices touched the lamina, a posterior margin of the wing could not contact the SP surface because SP had the slope of 3∼5 degrees. While wings compressed, even if the wing-type devices were inserted the three-armed center area initially, the devices should be migrated posteriorly (7-8 mm) because of the heavy lamina angle of 34∼41 degrees (migration effect). Posterior migration of somewhat larger sized device while compressing wings could make higher stress on the mid-portion of SP, possible resulting in frequent SP fracture.2The refinement of design of ISDs according to the anatomical reference is supposed to be necessary. The core bar (7∼8 mm width) should be located at the three-armed center rather than further posterior interspinous space. If the wings, in wing-type devices, were to be connected to the core bar at the level of lamina, they should be tilted as the reference angle of lamina slope (34∼41°) rather than vertically in order not to be posteriorly migrated when they were compressed tightly.
None declared
Sénégas J, Vital JM, Pointillart V, Mangione P. Long-term actuarial survivorship analysis of an interspinous stabilization system. Eur Spine J 2007;16(8):1279–1287
Bowers C, Amini A, Dailey AT, Schmidt MH. Dynamic interspinous process stabilization: review of complications associated with the X-Stop device. Neurosurg Focus 2010;28(6):E8
Verhoof OJ, Bron JL, Wapstra FH, van Royen BJ. High failure rate of the interspinous distraction device (X-Stop) for the treatment of lumbar spinal stenosis caused by degenerative spondylolisthesis. Eur Spine J 2008;17(2):188–192