
Abstract
Study Design
Prospective cohort study.
Objectives
To analyze the effectiveness and practicality of using cancellous bone substitute with platelet-rich plasma (PRP) in posterolateral arthrodesis.
Methods
Twenty consecutive patients underwent posterolateral arthrodesis with implantation of cancellous bone substitute soaked with PRP obtained directly in the operating theater on the right hemifield and cancellous bone substitute soaked with saline solution on the right.
Results
Computed tomography scans at 6 and 12 months after surgery were performed in all patients. Bone density was investigated by comparative analysis of region of interest. The data were analyzed with repeated-measures variance analyses with value of density after 6 months and value of density after 12 months, using age, levels of arthrodesis, and platelet count as covariates. The data demonstrated increased bone density using PRP and heterologous cancellous block resulting in an enhanced fusion rate during the first 6 months after surgery.
Conclusions
PRP used with cancellous bone substitute increases the rate of fusion and bone density joining osteoinductive and osteoconductive effect.
Introduction
Arthrodesis is the conclusive target of vertebral fixation. Posterolateral fusion is commonly used in lumbar spine surgery. It consists of fusion between two adjacent vertebrae across the lamina and transverse processes. 1 Fusion depends on host and surgical factors including the selection of an appropriate graft. Iliac crest autograft has long been considered the gold standard for bone graft procedures. However, its use is associated with significant disadvantages including insufficient availability, donor site pain, increased operative time, increased estimated blood loss, and longer hospital stay. 2 Many autologous or heterologous bone substitutes are used to reach fusion. Currently, there are over 200 different commercial types of bone graft extenders, enhancers, and substitutes available from which to choose. 3 The objective is to find an osteoinductive and osteoconductive substrate that is also safe and easy to apply. The efficacy of platelet-rich plasma (PRP) as an osteoinductive material has been studied by several authors. 4 , 5 , 6 Preliminary results about using PRP in posterolateral fusion have been encouraging. 7 In this article, we analyze the effectiveness and practicality of using an heterologous cancellous bone substitute with autologous PRP obtained directly in the operating theater.
Materials and Methods
We evaluated 20 consecutive patients who underwent posterior decompression, vertebral fixation with pedicle screws, and posterolateral fusion from January 2012 to January 2013 at the department of Neurological and Neurosurgical Sciences of “Sapienza” University of Rome. Written consent was obtained from all participating patients. The inclusion criteria were degenerative or traumatic lumbosacral spine disease and normal platelet count (150 to 450 × 106/mL). The exclusion criteria were previous lumbosacral surgery, fixation involving dorsal vertebrae, neoplastic disease, blood dyscrasias, and abnormal platelet count. The following method was used: cancellous bone substitute (25 × 50 × 30 mm) soaked with autologous PRP was implanted on the right hemifield and cancellous bone substitute (25 × 50 × 30 mm) soaked with saline solution on the left hemifield. Tecnoss (Torino, Italy) SP-Block Soft BS7E (25 × 50 × 30 mm) was used as a bone substitute. It consists of a rigid heterologous cancellous collagenated bone block of equine origin. If hydrated with saline solution for 5 to 10 minutes, it becomes flexible and malleable. Each block was enough to cover two levels of arthrodesis unilaterally. Autologous PRP was obtained in the operating theater by taking peripheral venous blood from the patient. The Regen system (RegenLab, Lausanne, Switzerland) was used, consisting of an 8-mL patented test tube Regen THT-SP and a Regen centrifuge (H19-F Regen Centrigel) placed directly in the operating theater. The test tube containing 3 ± 0.1 g of polyester gel and 1 ± 0.05 mL of sodium citrate solution was centrifuged for 8 minutes at 3,100 rpm (1,500 g). This removes 95 to 100% of total red blood cells, with 80% of white blood cells and a platelet concentration between 2.5 and 4.5 × 106/μL remaining. After centrifugation, the content was divided into red blood cells below the filter at the base of the tube and PRP with buffy-coat superiorly. Platelets were suspended in plasma while shaking the tubes. The product was then ready for use. Each tube contained ∼4.5 mL of PRP, immediately available for application and enough to cover about two levels of arthrodesis unilaterally. The contact of the PRP with the porosity of the cancellous bone substitute and the addition of 2 mL of calcium gluconate favored the activation of the coagulation cascade and platelet activation (Fig. 1). Investigations into bone density were obtained by comparative analysis of region of interest (ROI) on computed tomography (CT) scan images. A square area 0.4 cm in size (ROI) is traced over the axial CT scan across the lamina and transverse processes. The electronic calculation of the mean pixel content (bidimensional unit of measurement) can be done in Hounsfield units (HUs). The numerical value obtained is the average of the densitometric values of the pixels contained in the area; HU = 0 corresponds to water, −1,000 to air, and +1,000 to cortical bone.
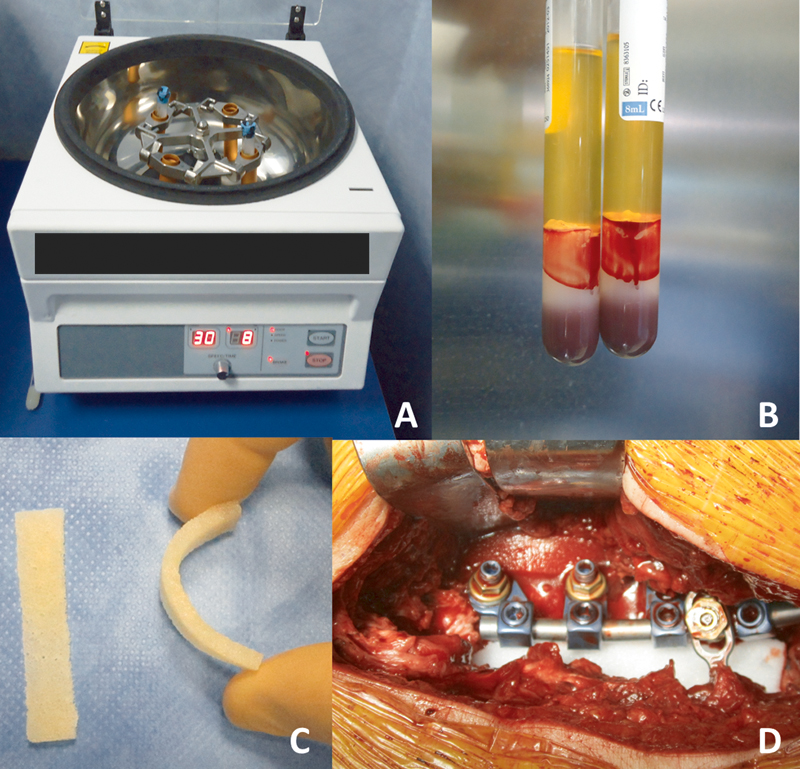
(A) Centrifuge placed in the operating room. (B) After centrifugation, red blood cells trapped below the filter of gel content at the base of the tube. The upper portion is divided in the platelet-rich plasma and in the upper buffy-coat; (C) bone block; (D) intraoperative picture.
Results
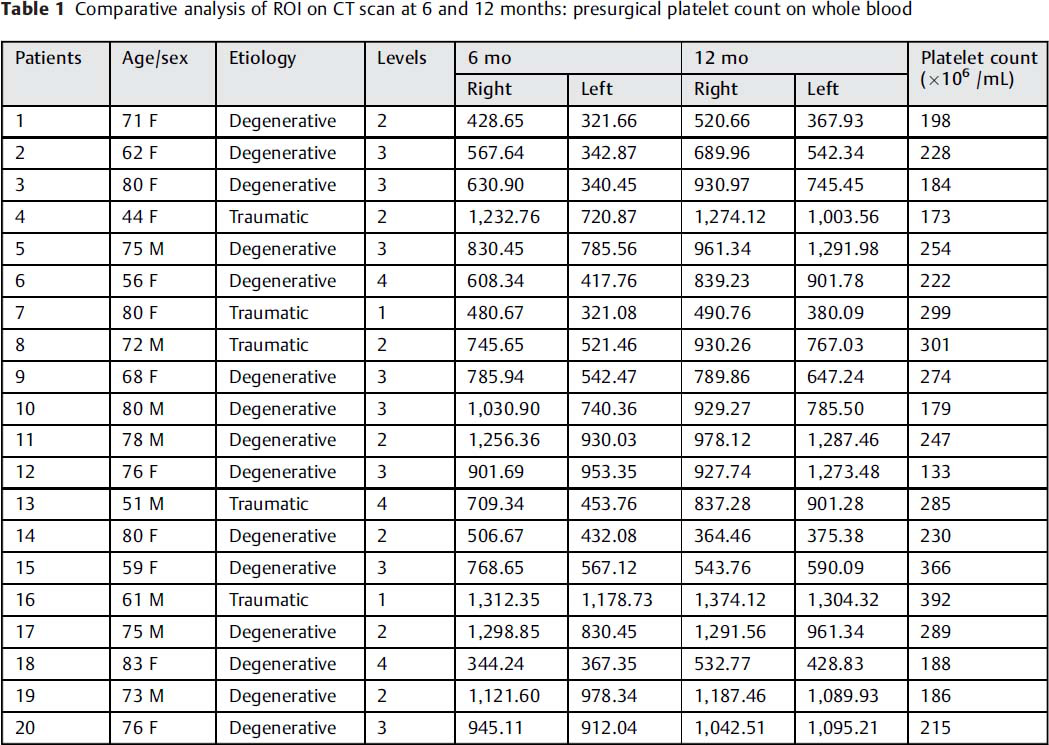
The 20 patients included 8 males and 12 females with mean age = 70 (standard deviation [SD] = 10.9). They were operated on for 15 lumbar stenosis and 5 lumbar body fractures. The platelet count in the whole blood varied between 173 and 390 × 106/mL. A CT scan 6 and 12 months after surgery was performed in all patients (Figs. 2 and 3). Investigations into bone density were obtained by comparative analysis of ROI (Table 1). The data were analyzed with two repeated-measures variance analyses with value of density after 6 months and value of density after 12 months as factors (density on the right hemifield versus density on the left hemifield) using age, levels of arthrodesis, and platelet count (in the whole blood) as covariates.
Comparative analysis of ROI on CT scan at 6 and 12 months: presurgical platelet count on whole blood
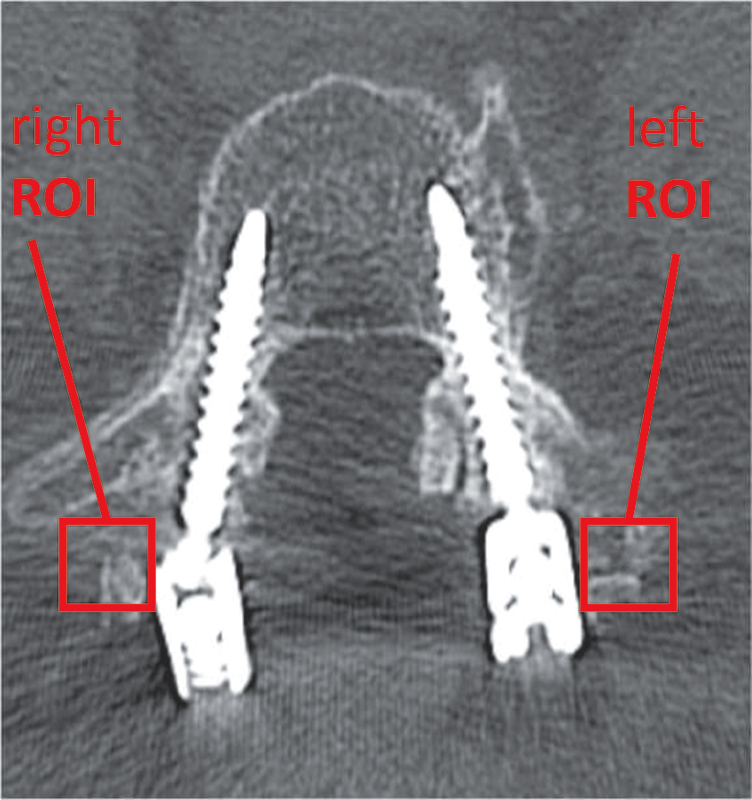
Region of interest (ROI) analysis on computed tomography scan 6 months after surgery.

Coronal computed tomography scan 6 months after surgery.
The main effect of value of density after 6 months was significant (F(1,19) = 5.522, p < 0.05): the value of density on the right hemifield after 6 months was significantly different from the value of the density on the left hemifield (mean = 830.353 [SD 61.8] for the right hemifield versus mean = 632.890 [SD 59.5] for the left hemifield). The post hoc mean comparison showed that the value of density on the right hemifield was significantly greater than the value of density on the left hemifield after 6 months (Δ = 197.463; F(1,19) = 43, p < 0.001). The interaction with age was marginally significant (F(1,19) = 3.700, p = 0.72); the interaction between the levels (F(1,19) = 2.070, p = 0.169) and the platelet count (F(1,19)= 0.64, p = 0.804) was not significant, which suggests no effects of these variables on results.
These data demonstrate increased bone density using PRP and heterologous cancellous block in the first 6 months after surgery (Fig. 4).
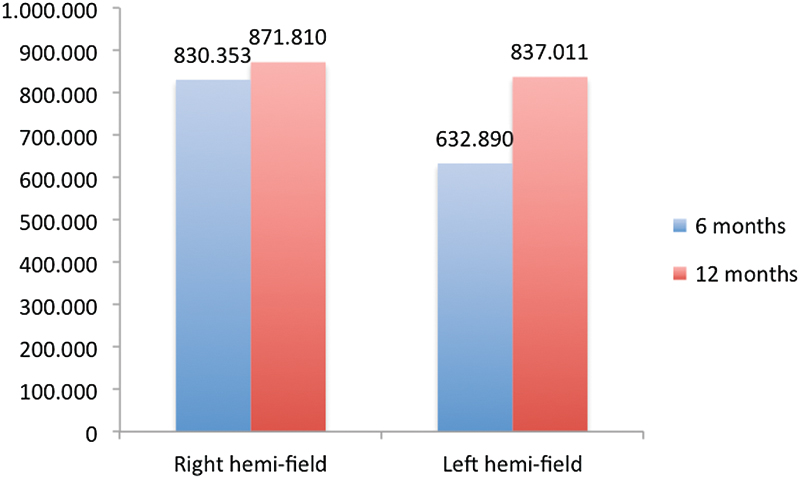
Bone density between the left and the right hemifields at 6 and 12 months.
The analysis of variance on the value of the density after 12 months showed that at this time no significant difference was observed in the two hemifields (F(1,19)= 1.100, p = 0.310). In fact, the mean of the value of the density on the right hemifield was 871.810 versus 837.011 of the left hemifield after 12 months (Δ = 34.79; F(1,19) = 0.665, p = 0.426). Also in this case, no interaction between the covariates of age (F(1,19) = 0.573, p = 0.460.), levels (F(1,19) = 1.407, p = 0.253), and platelet count (F(1,19) = 0.117, p = 0.737) was observed. No correlation between bone density and preoperative platelet count was observed.
Discussion
Posterolateral arthrodesis is a fusion between two adjacent vertebrae across the lamina and transverse processes. 1 Many autologous or heterologous bone substitutes are generally used as an implantation to reach fusion. 3 The objective is to find an osteoconductive and osteoinductive substrate that is also safe and easy to apply. The bone substitute is a heterologous cancellous collagenated bone block of equine origin. Its acts as an osteoconductive scaffold. Collagen binding to fibronectin promotes the anchorage of mesenchymal stem progenitors, on which it exerts its chemotactic action and induces differentiation into osteoblasts. It has a rigid and malleable consistency and maintains the original graft volume from 6 to 18 months from application. This is particularly important to allow the rapid development of the bony bridge between the transverse processes. This also reduce the risk of pseudarthrosis and nonunion present in arthrodesis performed with other substitutes. 8 Moreover, cancellous bone substitute can be used also in association with autologous bone graft (laminectomy bone chips); future investigations to analyze this option are necessary.
In this study, we included both patients with degenerative conditions and patients who experienced trauma. Because posterior elements are intact in vertebral body fractures, the cohort of patients is homogeneous. We excluded patients with tumor because we do not routinely perform posterolateral arthrodesis. Fusion was assessed with computerized analysis of ROI, a square area 0.4 cm in size traced over the axial CT scan across the lamina and transverse processes. It is important to emphasize that the numerical value obtained from this measurement is the average of the densitometric values of the pixels contained in the area studied. We did not notice high-density areas that could be hypertrophic pseudarthrosis. PRP has an osteoinductive effect increasing the bone regeneration and production. 9 , 10 This is due to the action of growth factors released by platelets upon activation. Platelets are a potential source of multiple autologous growth factors, and proteins are involved in the physiologic processes of healing and tissue regeneration. The products rich in platelets have the goal to replace the blood clot with a preparation enriched in platelets that, once activated, secrete large amounts of proteins and growth factors (platelet-derived growth factor, epidermal growth factor, transforming growth factor-β, vascular endothelial growth factor, insulin-like growth factor 1). They exert mitogenic action on osteoblasts and induce the differentiation of mesenchymal stem progenitors into osteoblasts. 11 Autologous PRP can be obtained directly in the operating theater. This method is faster and immediately available to the surgeon.
PRP has to be prepared to effectively separate the platelets from red blood cells, taking care not to damage the platelets. This method is important because the growth factors contained within the platelet α-granules are activated at the same time that the granules themselves merge with membrane platelet. 12 , 13 , 14 The properties of the PRP in tissue repair have already been documented in numerous studies. Therefore, the molecular mechanisms through which the growth factors stimulate repair are complex and depend on the different types of tissues and types of cells that receive the messages. 15 PRP is obtained by platelet sequestration and concentration. The exact relationship between the platelet count and the concentration of growth factors remains unclear. No correlation between bone density and whole blood platelet count was found in our series. Several in vitro studies seem to point out that the content of platelet growth factors is quite variable among individuals and is not necessarily proportional to the platelet count. 16 PRP is an autologous product and is completely safe for the patient. Moreover, it promotes leukocyte chemotaxis and has antibacterial effect and also increases tissue repair and remodeling. 16 Several studies demonstrated that iliac crest autograph is the gold standard for bone graft procedures including posterolateral fusion. 2 , 3 As its use is associated with significant disadvantages (including insufficient availability, donor site pain, increased operative time, increased estimated blood loss, longer hospital stay), many surgeons prefer to use heterologous bone substitutes even if it is proved that their validity is lower. In this study, we are testing an alternative option that appears to be effective and safe. The validity of our method has not been compared with autograph, but the technique can be improved in the future.
Conclusions
PRP used with cancellous bone substitute increases the speed of bone production in posterolateral arthrodesis joining osteoinductive and osteoconductive effect. Autologous PRP can be produced directly in the operative theater. The preparation is very quick and can be made also during surgery. This method is a safe and effective alternative option to the common bone substitutes.
Disclosures
None