
Abstract
The purpose of this retrospective study was to demonstrate the surgical outcomes of anterior spinal fusion (ASF) and posterior subtraction osteotomy (PSO) for osteoporotic vertebral collapse (OVC). Forty patients who underwent surgery for OVC at the thoracolumbar junction with neurological deficits were included in this study. ASF was primarily chosen for patients without vertebral compression fracture at other levels, and PSO was chosen for patients with more severe kyphosis or with multiple vertebral fractures. ASF was performed in 26 patients and PSO was performed in 14 patients. We evaluated the pre- and postoperative clinical status consisting of pain, gait, paralysis, and bladder function analysis. Additionally, pre- and postoperative kyphosis, correction angle, correction loss, and upright balance were investigated radiologically. Improvements in pain level, gait, paralysis, and bladder function were obtained in both groups. Average correction angles in the ASF and PSO groups were 16 and 37, respectively. Average correction losses at the final follow-up in the ASF and PSO groups were 7 and 13, respectively. Newly developed postsurgical vertebral compression fracture adjacent to the level of instrumentation was observed in four patients (15%) in the ASF group and in 11 patients (79%) from the PSO group. ASF provided satisfactory outcomes for patients with thoracolumbar OVC, who have no vertebral compression fracture at other levels. Although PSO has benefits for the correction of kyphosis, several problems persist with this procedure, especially for patients with severe osteoporosis.
Keywords
Osteoporotic vertebral fracture is a significant injury producing a functional loss in activities of daily living for an increasing elderly population. Osteoporotic vertebral compression fracture is conventionally treated conservatively with rest, immobilization, analgesics, brace therapy, and physical therapy. However, these compression fractures sometimes fail to heal, resulting in progressive collapse and/or pseudarthrosis. This situation has been defined as osteoporotic vertebral collapse (OVC). 1 , 2 Furthermore, OVC at the thoracolumbar junction often causes neurological deficits. Development of neurological deficits is typically associated with several factors, including direct neural compression from retropulsed bony fragments in the spinal canal, abnormal neural alignment subsequent to progressive kyphosis, and dynamic neural damage due to abnormal mobility at the fracture site.
Decompression of the neural elements and restoration of spinal stability are essential in the surgical management for OVC. However, not only local factors but also general problems have to be considered when treating OVC. Patients with OVC have relatively severe osteoporosis and often possess multiple preexisting vertebral compression fractures, leading to technical difficulty in achieving spinal reconstruction. General spinal deformity is also a significant problem for these elderly patients such that local restoration of spinal alignment sometimes leads to adjacent spinal problems. 3 , 4 Surgical treatment for OVC is tailored for the individual patient presentation due to the multiple comorbidities in the osteoporetic population.
We have selected two common surgical interventions for OVC at the thoracolumbar junction that have been in use since 1998: anterior spinal fusion (ASF) and pedicle subtraction osteotomy (PSO). The purpose of this retrospective study was to demonstrate surgical outcomes of these two separate procedures.
Materials and Methods
Patient Population
Forty-one patients underwent surgery for thoracolumbar junction OVC between 1998 and 2008 at Osaka Rosai Hospital. Forty of them could be followed for at least 1 year (follow-up rate, 97%) and were included in this study. There were 15 men and 25 women. The average age at the time of surgery was 74 years (range, 60 to 80 years) and the average follow-up period was 50 months (range, 12 to 100 months). Surgery was indicated due to neurological deficits for all patients. Back pain alone without neurological deficits was not a surgical indication in this series. Although there was no clear criterion for the selection of either of these two surgical methods, ASF was mainly selected for patients without vertebral compression fracture at other levels, and PSO was selected for patients with the following characteristics: severe kyphosis, severe osteoporosis with multiple vertebral fractures, secondary osteoporosis (rheumatoid arthritis or steroid-induced), or association with spinal cord compression by posterior elements. ASF was performed in 26 patients and PSO was performed in 14 patients. Seven patients in the PSO group had rheumatoid arthritis or a history of steroid use. The average age (range) and male-to-female ratio in the ASF group were 74 years (60 to 80 years) and 13:13, respectively, and those in the PSO group were 73 years (62 to 80 years) and 2:12, respectively. The collapsed vertebral levels in the ASF group were T12 in 17 patients, L1 in seven, and L2 in two. The collapsed vertebral levels in the PSO group were T11 in one patient, T12 in seven, and L1 in six (Table 1).
Demographic data
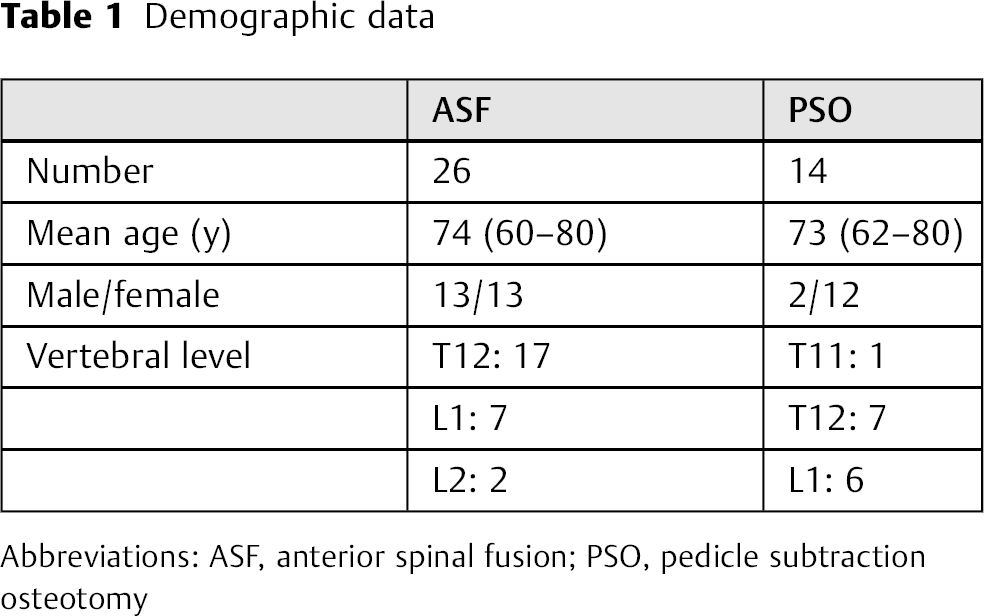
Abbreviations: ASF, anterior spinal fusion; PSO, pedicle subtraction osteotomy
Surgical Methods
ASF Procedure
The collapsed vertebral body was exposed via an extra- or transpleural and retroperitoneal approach. 5 After subtotal resection of the collapsed vertebral body and adjacent intervertebral disks, iliac or fibular strut bone was inserted as an anterior support. Anterior instrumentation was used, and the area of instrumentation was located at one segment above and one segment below the collapsed vertebra.
PSO Procedure
Laminectomy with bilateral total facetectomy was performed first, and then bilateral pedicles and intervertebral disk and necrotic vertebral tissue were excised through a posterior approach. Spinal shortening was performed with a pedicle screw system after insertion of the trimmed bone (made by the excised posterior elements) into the interbody free space. Finally, posterior pedicle screw fixation was performed including two or three segments above and below the collapsed vertebra. 6 Instrumentation removal was originally planned to restore mobility at the unfused segments after bony union was achieved at the shortened segment in the first eight patient cases. In the last six patients, instrumentation removal was not considered to be a standard protocol because new compression fractures at the fusion area were frequently observed after instrumentation removal in the earlier cases. Posterior and/or posterolateral bone graft was added to the whole segments of instrumentation for these six patients.
Clinical Assessment
Complete hospital and attending records on all patients were available for review. These records were assessed to determine demographic data including the primary diagnosis, operating time, intraoperative blood loss, and operative complications. In this study, we used two methods for evaluation of pre- and postoperative clinical status; one is the Frankel classification and the other is our original scoring system. This original scoring system consists of pain, gait, paralysis, and bladder function. A full score is 3 points in each category (Table 2). The pain scale was scored as follows: pain that is not controlled with medication, 0 points; pain that can be controlled with medication, 1 point; pain that is controlled without medication, 2 points; painless or negligible pain, 3 points. The gait scale was scored as follows: unable to maintain a standing position, 0 points; able to maintain a standing position but unable to walk, 1 point; able to walk with support, 2 points; able to walk without support, 3 points. The lower-extremity paralysis scale was scored as follows: manual muscle test (MMT) 0, 0 points; MMT 1 to 2, 1 point; MMT 3 to 4, 2 points; MMT 5, 3 points. In the present series, the tibialis anterior muscle showed prominent weakness at the preoperative paralysis; therefore, this muscle was used for the MMT evaluation. The bladder function scale was scored as follows: urinary retention, 0 points; urinary residence, 1 point; urinary retardation, 2 points; normal, 3 points. Postoperative complications were also investigated. Clinical assessment was performed for all patients before surgery; at 1, 3, 6, and 12 months after surgery; and at the final follow-up.
Original scoring system consisting of pain, gait, paralysis, and bladder function
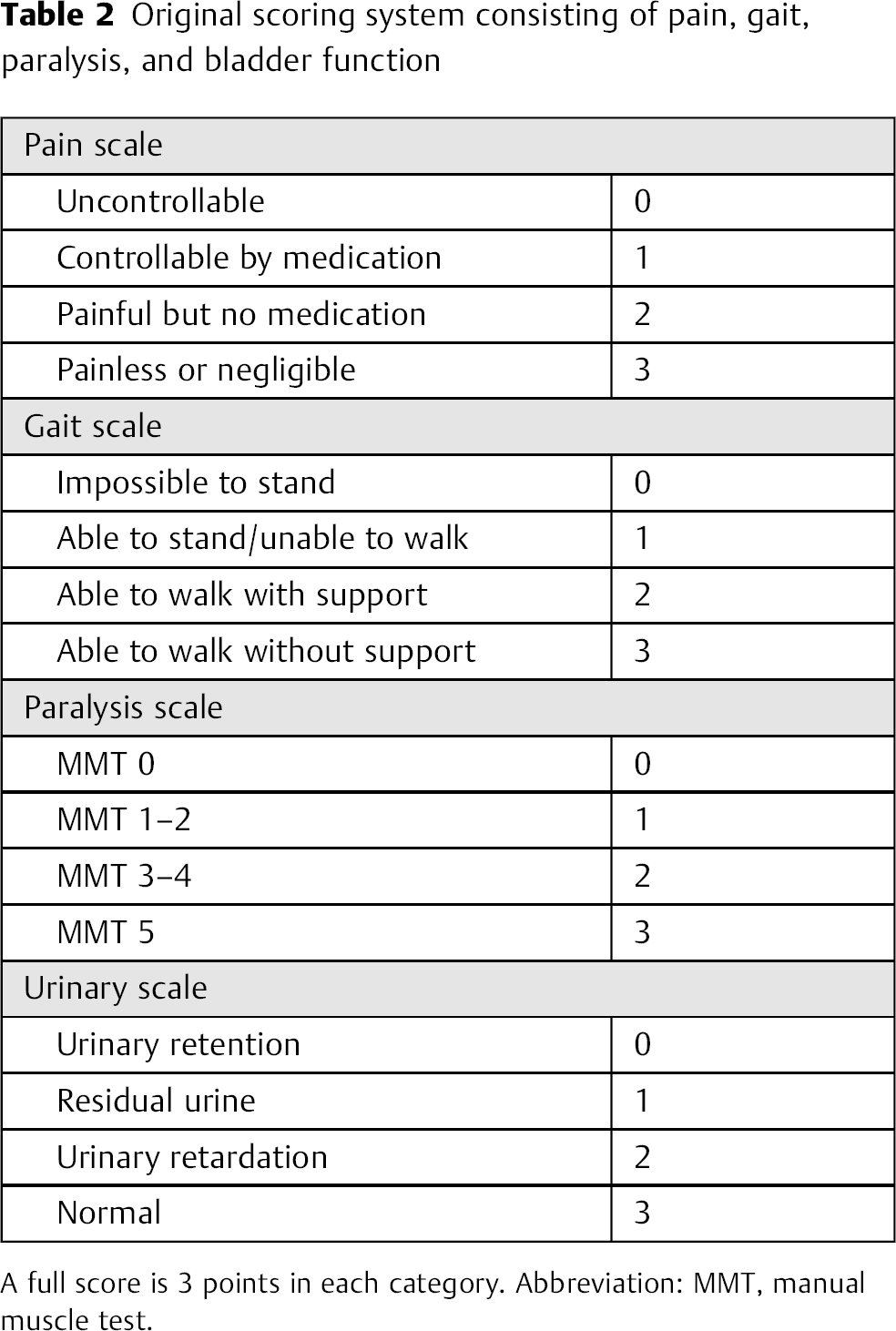
A full score is 3 points in each category. Abbreviation: MMT, manual muscle test.
Radiological Assessment
Fusion status, pre- and postoperative kyphosis, correction angle, correction loss, and upright balance were investigated. Fusion status was evaluated with dynamic lateral radiographs. Fusion status was evaluated at the site of the shortened segment within the PSO group. The kyphotic angle was measured in the instrumentation area with a lateral radiograph. The distance between the C7 plumb line and the midline of the sacrum on a standing anteroposterior radiograph was measured as the index of coronal balance. The distance between the C7 plumb line and the sacral promontory on a standing lateral radiograph was measured as the index of sagittal balance. New (postoperative) development of vertebral compression fracture and instrumentation failure was also investigated as a late complication. Radiological assessment was performed for all patients before surgery; at 1, 3, 6, and 12 months after surgery; and at the final follow-up.
Statistical Analysis
Findings from these measurements were analyzed statistically using simple regression analysis, Student t test, and C2 analysis.
Results
Clinical Results
The mean operating time was 354 minutes (range, 210 to 585 minutes) in the ASF group, and 436 minutes (range, 195 to 700 minutes) in the PSO group. Intraoperative blood loss averaged 1472 mL (range, 230 to 7420 mL) in the ASF group, and 1581 mL (range, 400 to 5650 mL) in the PSO group.
Frankel classification showed 32 patients with grade C and 8 patients with grade D preoperatively improved to 1 patient with grade C, 32 patients with grade D, and 7 patients with grade E at the final follow-up. Thirty-three patients showed at least one grade improvement. As for original scoring system, the average pre- and postoperative pain scores in the ASF group were 0.5 and 2.3 points, respectively, and those in the PSO group were 0.5 and 1.8 points, respectively. The average pre- and postoperative gait scores were 1.2 and 2.4 points, respectively, in the ASF group, and 0.6 and 2.0 points, respectively, in the PSO group. The average pre- and postoperative paralysis scores were 1.2 and 2.6 points, respectively, in the ASF group, and 1.4 and 2.4 points, respectively, in the PSO group. Foot drop was observed in 14 patients before surgery; however, it improved in all but one patient postoperatively. The average pre- and postoperative bladder function scores in the ASF group were 1.5 and 2.3 points, respectively, and those in the PSO group were 1.4 and 2.6 points, respectively. The average pre- and postoperative total scores in the ASF group were 4.5 and 9.6 points, respectively, and those in the PSO group were 3.9 and 8.9 points, respectively (Fig. 1). In both groups, improvements were obtained in all categories.

Pre- and postoperative clinical status consisted of pain, gait, paralysis, and bladder function scores. A full score is 3 points for each category. Abbreviations: ASF, anterior spinal fusion; op, operation; PSO, posterior subtraction osteotomy.
Radiological Results
Bony union was achieved in 24 patients (92%) in the ASF group. Bony union at the shortened segment was obtained for all patients (100%) in the PSO group. Average kyphotic angles in the area of instrumentation before surgery, immediately after surgery, and at the final follow-up in the ASF group were 34, 18, and 25 degrees, respectively, and those in the PSO group were 41, 4, and 17 degrees, respectively (Fig. 2). Average correction angles in the ASF and PSO groups were 16 and 37 degrees, respectively. Average correction losses at the final follow-up in the ASF and PSO groups were 7 and 13 degrees, respectively. The main cause of correction loss was subsidence of the graft bone in the ASF group, and in the PSO group the main cause was newly developed vertebral compression fracture after removal of instrumentation. Average correction loss was 17 degrees in eight patients after removal of instrumentation and 2 degrees in six patients without removal of instrumentation. The average distances between the C7 plumb line and midline of the sacrum before surgery, immediately after surgery, and at the final follow-up in the ASF group were 6 mm, 10 mm, and 12 mm, respectively, and those in the PSO group were 14 mm, 12 mm, and 13 mm, respectively. The average distances between the C7 plumb line and the sacral promontory before surgery, immediately after surgery, and at the final follow-up in the ASF group were 34 mm, 23 mm, and 47 mm, respectively, and those in the PSO group were 44 mm, 30 mm, and 68 mm, respectively (Fig. 3).
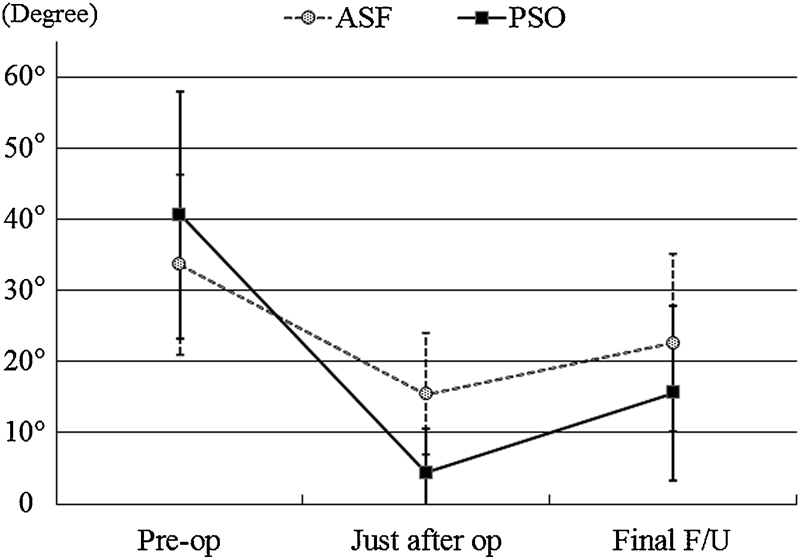
Average kyphotic angles in the instrumentation area before surgery, immediately after surgery, and at the final F/U. Abbreviations: ASF, anterior spinal fusion; F/U, follow-up; op, operation; PSO, posterior subtraction osteotomy.
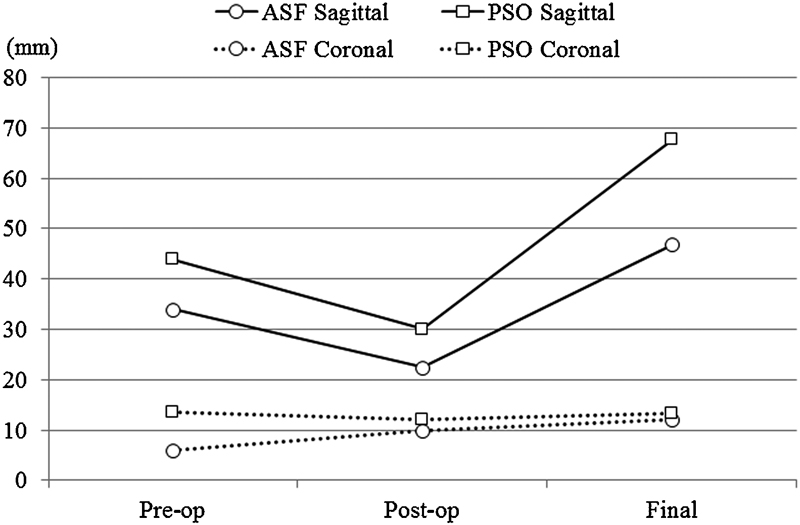
Sagittal and coronal balance in the instrumentation area before surgery, immediately after surgery, and at the final follow-up. Abbreviations: ASF, anterior spinal fusion; op, operation; PSO, posterior subtraction osteotomy.
Postoperative Complications
Deep surgical site infection developed in one patient (4%) in the ASF group. Anterior instrumentation was removed 3 months after surgery, and additional surgeries were required to control infection in this patient. Pseudarthrosis was the ultimate outcome for this patient. Pseudarthrosis was observed in one other patient; however, additional treatment has not yet been performed due to asymptomatic nonunion. Bone graft subsidence was observed in nine patients (35%), one of whom (4%) required additional posterior fixation due to upper screw cutout and progressive kyphotic deterioration with severe back pain. Newly developed vertebral compression fractures adjacent to the level of instrumentation were observed in four patients (15%). These fractures were treated conservatively, and the symptoms associated with these fractures resolved. As for indication of revision surgery, symptomatic progressive kyphosis more than 10 degrees due to graft bone subsidence or newly developed vertebral compression fractures adjacent to the level of instrumentation was considered for additional posterior reinforcement. There were no major perioperative complications including surgical site infection in the PSO group. Newly developed vertebral compression fracture was detected in 11 patients (79%), three of whom (21%) underwent additional revision surgery as a result of their symptom deterioration. Newly developed vertebral compression fracture in the instrumentation area developed after instrumentation removal, and symptom deterioration was observed due to the recurrence of kyphosis in two patients. In another patient, pedicle screws at the caudal end of the instrumentation pulled out due to newly developed vertebral fracture, resulting in severe pain. These three patients underwent revision surgery to extend the fusion area. Pedicle screw loosening was detected in two patients, but no backing out of the screws was observed in the six patients who did not undergo implant removal (Table 3).
Postoperative complications
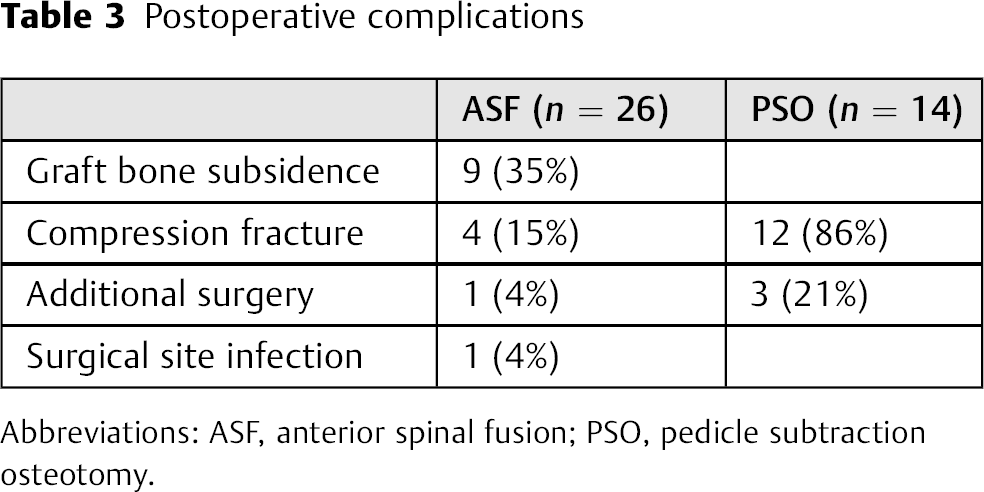
Abbreviations: ASF, anterior spinal fusion; PSO, pedicle subtraction osteotomy.
Discussion
OVC is often associated with progressive kyphotic deformity and neural tissue compression and is only amenable to major surgical intervention. 1 , 2 However, there is controversy regarding which is the most appropriate spinal reconstruction method. Commonly reported techniques include ASF, 1 , 5 , 7 , 8 , 9 posterior fusion alone, 2 , 10 PSO, 4 , 6 , 11 , 12 , 13 , 14 , 15 , 16 , 17 and combined anterior and posterior surgery. 17
The advantages of ASF include direct decompression of the retropulsed bony fragments, reconstruction of the stable anterior spinal column, and preservation of the intact posterior elements. 5 , 8 However, some reports have indicated that additional posterior reinforcement is required due to insufficient fixation with anterior instrumentation alone. In addition, postoperative development of adjacent vertebral collapse has been reported in patients with steroid-induced osteoporosis or low bone mineral density. 7 , 9 , 10 Kanayama et al reported that the rates for patients requiring posterior reinforcement were 15.4% in one-level corpectomy patients and 40% in two-level corpectomy patients. 7 However, in this series additional posterior reinforcement was required in only one patient with the exception of the case with deep surgical site infection. ASF demonstrated favorable surgical outcomes in the present study. We consider ASF to be the treatment of choice for patients with thoracolumbar junction OVC, who have no vertebral compression fracture at other levels. However, the maintenance of local sagittal alignment after kyphosis correction remains a persistent problem, especially in elderly patients or patients with poor bone quality. In addition, salvage surgery for deep surgical site infection is quite distressful to both surgeon and patient. Reapproach to the anterior spinal elements is difficult in the situation of severe adhesion to the surrounding tissue, which is associated with relatively high risk for the damage of important organs, major vessels and the urinary tract.
Several reports have described the surgical outcomes of PSO for OVC. 4 , 6 , 11 , 12 , 13 , 14 , 15 , 16 , 17 PSO enables both decompression of the neural elements and correction of kyphosis. PSO obtained better correction of kyphosis when compared with ASF; however, problems still remain in the maintenance of sagittal alignment after kyphosis correction with the PSO procedure as well as with the ASF. There were high rates of newly developed postoperative vertebral compression fracture (79%) and additional surgery (21%) within the PSO group in the present study. Although we do not have quantitative osteoporosis data such as bone mineral density, we speculate that there was an apparent bone quality deficit in the PSO group to a greater degree than that found in the ASF group. This may be due to the demographic makeup of the PSO group, in which half of the patients had a diagnosis of rheumatoid arthritis or a history of steroid use. In addition, the proportion of women in the PSO group was higher than that in the ASF group. Therefore, the reasons for the higher rates of newly developed compression fracture in the PSO group were considered to be due to poor bone quality rather than the surgical procedure itself. PSO had an advantage in kyphosis correction; however, kyphosis recurred due to the newly developed vertebral compression fractures. Our primary objective for the PSO procedure was to obtain stability in the shortened segments. For this purpose, we considered that a temporary fixation area, including two or three segments above and below the involved segment, was necessary. Therefore, instrumentation removal was originally planned after bony stability in the shortened segment was achieved. However, newly developed vertebral compression fractures in the fixation area frequently occurred after instrumentation removal, producing kyphotic deterioration. In addition, newly developed vertebral compression fractures developed at the end of the fixation area or at the level adjacent to the fixation in patients without instrumentation removal. However, prominent kyphotic deterioration was not detected in patients who did not have instrumentation removal. Therefore, we do not recommend instrumentation removal in patients with OVC. However, we simultaneously consider bony stability not only in the shortened segments but also in the segments adjacent to the fixation, to prevent instrumentation failure. In such situations, correction and maintenance of kyphosis by osteotomy with long fixation for severe osteoporotic patients may still have several problems.
Preoperative sagittal balance was poor in the PSO group when considering upright sagittal alignment. The sagittal balance improved immediately following surgery, but deteriorated due to correction loss over time. Similarly, deterioration of the sagittal balance was also observed in the ASF group. These results suggest that not only correction loss but also the aging process may affect progression of sagittal imbalance. Therefore, limitations do exist when attempting to correct the sagittal imbalance for elderly patients. A recent report recommended in situ fusion without correction of kyphosis. 18 , 19 , 20 , 21 Short segment fixation may be more important than correction of kyphosis for elderly patients with severe osteoporosis.
There were several limitations because this is a retrospective study of two separate procedures. First, preoperative evaluation of bone quality was not investigated. We did not describe any bone mineral density data or metabolic bone markers such as bone alkaline phosphatase and deoxypyridinoline. Second, it was difficult to compare the ASF and PSO groups because the preoperative condition and the indication of each group were quite different.
Conclusions
ASF has produced satisfactory outcomes for patients with thoracolumbar junction OVC, who have no vertebral compression fracture at other levels. PSO has benefits for the correction of kyphosis; however, several problems persist following this procedure, especially for patients with severe osteoporosis.
Disclosures
Shinya Okuda, None
Takenori Oda, None
Ryoji Yamasaki, None
Takamitsu Haku, None
Takafumi Maeno, None
Motoki Iwasaki, None