
Abstract
Study Design
Prospective observational cohort.
Objective
To document the accuracy of uncovertebral anatomic targeting in positioning cervical disc arthroplasty.
Summary of Background Data
Disc arthroplasty implants depend on midline placement for optimum mechanical function. Fluoroscopy is used to delineate the midline. Anatomic targeting from the uncovertebral joints in the neck may be adequate. We have investigated the efficacy of uncovertebral anatomic targeting for cervical disc arthroplasty.
Methods
Anatomic uncovertebral midline targeting for disc arthroplasty insertion was performed in 18 male (mean age 51 years, range 27 to 67) and 22 female (mean age 50, range 35 to 70) patients receiving a total of 59 implants over a 5-year period. Device insertion was under only lateral imaging control. Postinsertion operative fluoroscopy with optimized centering was used to record implant position in the anteroposterior plane, and centerline analysis was performed using cursor measurement technology from the GE PACS™ imaging system (GE Medical Systems, Mt. Prospect, IL).
Results
Analysis found a mean deviation from the ideal midline placement of only 0.7 mm (range, 0 to 2.9 mm). Only three devices were more than 2 mm off the anatomic midline.
Conclusion
This anatomic technique is effective, safely minimizing imaging resource needs and X-ray exposure to the patient and operating team.
Spinal disc arthroplasty implants are designed with a view to reconstructing normal motion segment kinetics and for optimal function must be perfectly positioned on the midline and maximally posterior within the disc space.
Anatomic positioning of the patient for surgery can easily leave minor tilt or rotation in the neck, but despite this, confirmation of anteroposterior (AP) implant positioning is easily accomplished with lateral fluoroscopic control by aligning the right and left lateral pillars of the spine on one another.
However, anatomic midline determination and implantation in the AP plane can be a challenge as a function of either minor rotations of the neck or asymmetry of prevertebral osteophytes compromising the surgeon's perception of the orthogonal plane. Marking the bone at surgery under AP fluoroscopy is traditionally proposed, 1 , 2 , 3 but even after such preliminary midline determination, minor deviations to one side or the other by the working tools used to fashion the disc space to accept an arthroplasty implant can easily lead to a misplaced device. Performing every step of the procedure under direct fluoroscopic control would help address this but requires either (1) a second operative fluoroscopy unit and very awkward positioning of the surgeon attempting to work within the confines of this AP-directed imager or (2) repeated transition of a single imager from the AP to the lateral plane with increased risk of surgical site contamination through that maneuvering. This would also lead to increased X-ray exposure to both the patient and the surgical team, and in a comparative study was not shown to be of benefit. 2 Surgical stereotaxy systems might potentially be used but to date are not reported in this application at the cervical level. So, surgical instrumentation systems taking advantage of local bony anatomic landmarks such as the uncovertebral joints might be of great practicality. 3
All the instruments used to fashion the disc space to accept the device (sizers, rasps, drill guides, and rail cutters) have a uniquely wedge-shaped design in the AP plane that allows for their self-centering through interference on the uncovertebral joints as they are worked into the index disc space.
We have undertaken an imaging review of our preliminary experience with this implant to determine the consistency of midline positioning of the implant using only these instruments as alignment guides in the mediolateral plane.
Neurological outcome in anterior cervical discectomy and fusion (ACDF) will depend as much on the indications for surgery as the technique and thoroughness of decompression, 5 , 6 and this analysis makes no attempt to address those issues in detail.
Methods
From January 2006 through August 2010, the author has used this one implant system consistently in anterior cervical discectomy reconstruction with lateral fluoroscopic control being used only during disc space preparation and device insertion. After implantation, centered AP fluoroscopic images are taken to confirm appropriate device placement and archived into our hospital's GE PACS™ digital imaging system.
These archived intraoperative images were later reviewed, measured, and implant distance off midline was calculated independently by the author, two colleague spine surgeons, and four senior orthopedic residents. Pooled results were then analyzed for consistency by a McMaster University statistics expert.
Patient Positioning and Imager Alignment
Patients were positioned on a radiolucent operating table under general anesthetic after oral intubation and induction of pharmacological neuromuscular paralysis. Gardner Wells tongs were applied and in-line traction with 5-pound weights applied to hold the head steady, and the shoulders were taped down distally to optimize fluoroscopic visualization of the more distal cervical segments. An inflatable positioning bag was placed behind the nape of the neck and inflated so as to optimize lordotic alignment of the neck during surgery.
Surgical Technique
All surgeries were done through a standard anterolateral approach from the right side and self-retaining handheld retractors were used.
After lateral fluoroscopic confirmation that the index disc had been accessed, the table or patient were slightly rotated when necessary so as to perfectly align the posterior cortex of the lateral masses with one another at the surgical level and so bring the fluoroscopy image to a “perfect lateral” orientation. Complete discectomy was performed, extending laterally as far as the visible base of the uncovertebral joints and posteriorly down to and through the posterior longitudinal ligament so as to allow complete visualization of the dura across the full width of the spinal canal. Foramen enlargement by resection of posterior uncovertebral osteophytes was performed as required, with care being taken to limit such resection to no more than the posterior third of the uncovertebral joint. Disc space preparation and device insertion were then done under lateral fluoroscopic control. After device insertion, the imager was rotated to the AP position, tilted sagittally so as to align with the index disc space, and rotated as needed so as to center the spinous process of the uninstrumented vertebra immediately caudal to the implant between its corresponding pedicles or uncovertebral joints. AP images were then taken and saved for later analysis.
Midline Determination and Implant Position Measurement
On the archived images, a digital cursor was used to draw a line bisecting the spinous processes immediately cephalad and caudal to the implant (Fig. 1). This established the midline. The implant's known lower baseplate width was then measured with the cursor (Fig. 2), and a correction factor to account for radiographic magnification was calculated (according to the formula known width in millimeters/cursor-measured width). Right- and left-sided baseplate widths from the midline were then measured. The difference between the right and left baseplate half-widths was then calculated, halved, and converted to give the true deviation from midline.
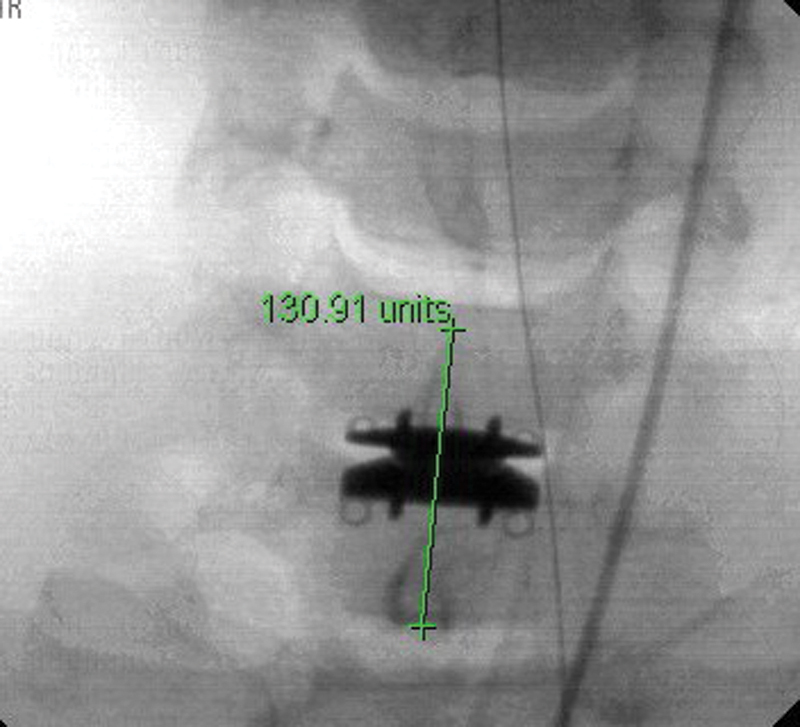
Midline determination.
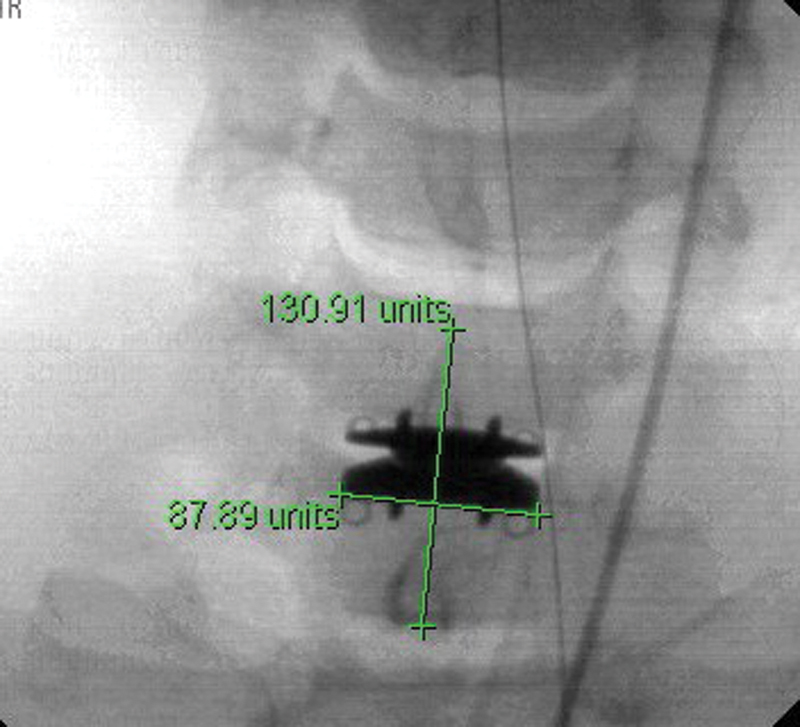
Cursor measure of known baseplate width.
Results
Some 63 implantations were performed in 43 patients during the study period.
Relatively advanced age was not considered a contraindication when preoperative magnetic resonance imaging confirmed the uncovertebral and facet joints to be healthy and not deteriorated. Multilevel spondylosis of the anterior column was considered a relative indication.
Postinsertion intraoperative images were available for 59 devices in 40 patients as four sets of images were inadvertently not saved. There were 18 male (mean age 51 years, range 27 to 67) and 22 female (mean age 50, range 35 to 70) patients reviewed.
All patients were largely relieved of their neurological symptoms, and also all cases where pain was a significant presenting symptom experienced significant relief of that symptom. There were no revisions and no implant migration noted in these patients.
Analysis found a mean deviation from ideal midline placement averaging only 0.7 mm (mean; range, 0 to 2.9 mm).
The intraclass correlation coefficient for all observers using a two-way mixed-effects model for average measures was 0.713, showing good consistency in our method of determining anatomic midline placement of our implants (Table 1).
Intraclass Correlation Coefficient
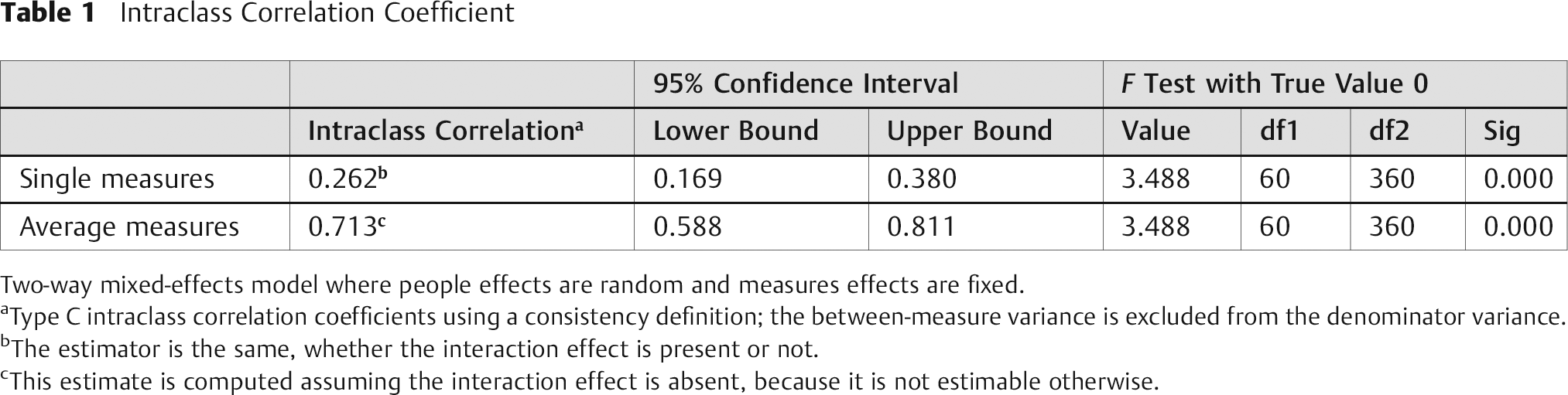
Two-way mixed-effects model where people effects are random and measures effects are fixed.
Type C intraclass correlation coefficients using a consistency definition; the between-measure variance is excluded from the denominator variance.
The estimator is the same, whether the interaction effect is present or not.
This estimate is computed assuming the interaction effect is absent, because it is not estimable otherwise.
The coefficient calculated separately for the group of three surgeon observers was 0.621 and for the group of four resident observers it was 0.635, suggesting that surgeon and resident observers were equally consistent with this technique of measurement and positioning calculation.
Discussion
Although the use of intraoperative AP fluoroscopy is not impossible during disc arthroplasty procedures, the requirement on the surgeon to work within the physical confines of the AP-directed imager gantry is awkward and does not lend itself to surgical exactitude. This would also require either that two imagers (AP and lateral) be available or that the imager be regularly rotated between the AP and lateral planes, with implications not just to radiation exposure but also to possible surgical site contamination. The results of this series suggest that AP imaging may not be required for accurate midline placement of the Prestige LP™ disc arthroplasty implant, and possibly for other systems in which the instrumentation is designed to align against the uncovertebral joints.
This cohort report does not allow for any comment on possibly decreased procedural time with single-plane imaging nor comparative accuracy against AP imaging-assisted procedures as it is not a controlled series.
Acute-phase neurological outcome in ACDF will depend as much on the indications for surgery as the technique and thoroughness of decompression, 5 , 6 and this analysis makes no attempt to address those issues in detail.
Longer-term reconstructive outcomes from disc arthroplasty reconstruction after decompression may be a function of implant positioning, which is the sole issue addressed in this technique article.
We propose here only to validate the accuracy of midline positioning of disc arthroplasty devices with our fluoroscopy-minimized technique using only lateral imaging during the procedure and have demonstrated that this technique achieves device placement with a mean deviation from midline of less than 1 mm.
Conclusion
Our results confirm that uncovertebral joint-based anatomic midline positioning using wedge-shaped tools to prepare the end plates for device insertion is highly accurate and that both surgeon and resident observers are equally consistent in measuring implant deviations from ideal position when using a standard measurement protocol.
Disclosure
Drew A. Bednar, None
Footnotes
Acknowledgments
The author thanks surgeon observers Dr. Aziz Al Mutair and Dr. Brian Drew; residents Drs. Osama Al Shaya, Christina Goldstein, Ian Robles, and Haifeng Ren; and Dr. Forough Farroukhyar, Associate Clinical Professor and Director of the Surgical Research Methodology Program at McMaster University, for their assistance with this project.