
Abstract
Adult isthmic spondylolisthesis most commonly occurs at the L5–S1 level of the lumbar spine. Slip progression is relatively rare in adults with this condition and slippage is typically associated with advanced degeneration of the disk below the pars defect. When symptomatic, radiculopathy is the typical complaint in adults with isthmic spondylolisthesis. When considering options for surgical treatment of adult isthmic spondylolisthesis, the surgeon must consider several different options, such as decompression, fusion, instrumentation, reduction, and type of bone graft to be used. All of these decisions must be individualized as deemed appropriate for each particular patient. This report presents a case of intraoperative slip progression of a L5–S1 adult isthmic spondylolisthesis to a high-grade slip, which was treated with complete surgical reduction and posterior instrumented fusion. This case demonstrates the potential instability of this condition in adults and has not been previously reported. The case details and images are reviewed and the intraoperative decisions, treatment options, and patient outcome are discussed.
Keywords
Adult isthmic spondylolisthesis most commonly occurs at the L5–S1 level of the lumbar spine. Its incidence has been reported to be 4% by the age of 6 years and 6% by adulthood. 1 Multiple classification systems have been established to help describe the amount of slippage present and attempt to determine etiology. It is generally accepted that isthmic spondylolisthesis is caused by insult to the pars interarticularis, whether it is due to stress or fatigue fractures, progressive elongation without separation, lytic destruction, or congenital defects. 2 , 3 , 4 ,5 One of the most common classification systems used to quantify the slip is that described by Meyerding. 2 According to this system, grade I defines a slip from 0 to 25%, grade II from 26 to 50%, grade III from 51 to 75%, and grade IV from 76 to 100%. Regardless of the classification system used, a high-grade slip is generally considered to be one in which the cephalad vertebra has translated greater than 50% the width of the caudad vertebra (greater than grade II). Although progression of isthmic spondylolisthesis has been documented in adolescents, its occurrence in adults is unknown.
One study 6 examined 21 adults with isthmic spondylolisthesis and reported that slip progression ranged from 8 to 30% during a period of 3 to 20 years after the fourth decade of life. The slippage was typically associated with advanced degeneration of the disk below the pars defect. This report presents a case of intraoperative slip progression of an L5–S1 adult isthmic spondylolisthesis to a high-grade slip, which was treated with surgical reduction and posterior instrumented fusion. This case demonstrates the potential instability of this condition in adults and has not been previously reported. The case details and images are reviewed, and the intraoperative decisions, treatment options, and patient outcome are discussed.
Case Report
The patient is a 58-year-old woman who presented with a 5-year history of bilateral lower extremity radicular symptoms, right greater than left. The distribution of the radicular symptoms was most consistent with the L5 nerve dermatome. She had no evidence of subjective or objective weakness on history and exam. She underwent a series of three diagnostic and therapeutic transforaminal epidural steroid injections at the L5–S1 level bilaterally, which gave her short-term complete relief of her lower extremity symptoms. In the last year, physical therapy and nonsteroidal anti-inflammatory medications had provided her with little relief, and her symptoms had progressed to the point that it was affecting the quality of her daily living.
Radiographs of the lumbar spine (Fig. 1) revealed evidence of grade 2 spondylolisthesis at L5–S1 with end-stage degenerative disk disease at that level. Magnetic resonance imaging was obtained, which showed bilateral foraminal narrowing of the L5–S1 foramen bilaterally due to both end-stage degenerative disk disease and a grade 2 spondylolisthesis. Of note, there was no evidence of central stenosis on magnetic resonance imaging (Figs. 2A, B). The patient felt that she had exhausted reasonable conservative treatment options and wanted to pursue surgical intervention at this time.

Preoperative standing lateral radiograph demonstrating grade II spondylolisthesis with advanced degenerative disk disease at the L5–S1 level.
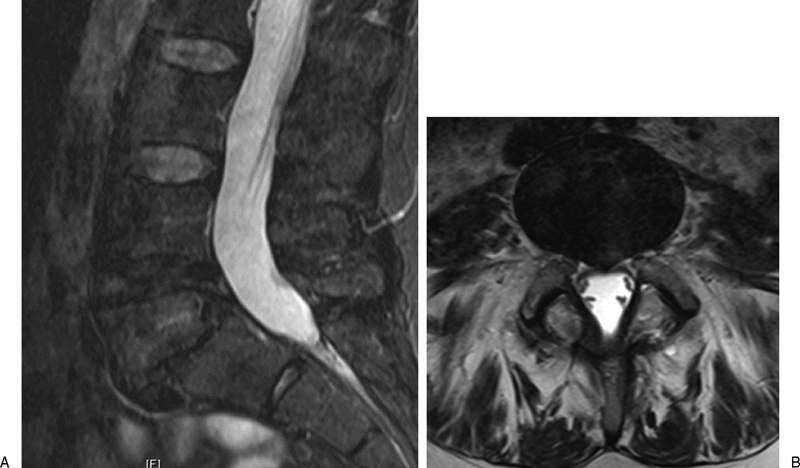
Preoperative sagittal (A) and axial (B) magnetic resonance images demonstrating grade II spondylolisthesis with advanced degenerative disk disease at the L5–S1 level. Note that there is no evidence of central stenosis despite the slip, but the symptoms are due to significant bilateral foraminal stenosis.
The patient was brought to the operating room for a planned posterior decompression of the L5–S1 level and posterior instrumented fusion without reduction. She was placed in the prone position on a Jackson spine table frame (Mizuho Ikakogyo Co., Ltd., Tokyo, Japan). Intraoperative neuromonitoring with somatosensory and motor evoked potentials were used during the procedure, and anesthesia was performed using total intravenous anesthesia. A preoperative fluoroscopic image of the lumbar spine at that time revealed that the spondylolisthesis remained a grade II at that time. The posterior elements of L5 and S1 were then surgically exposed. Prior to starting the decompression, a localization image was taken with intraoperative fluoroscopy revealing that the preoperative grade II spondylolisthesis had now slipped to a grade IV during the exposure (Figs. 3A, B).
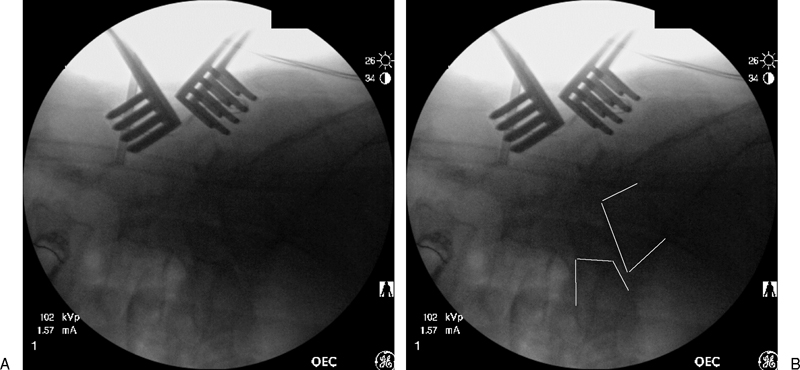
(A) Intraoperative lateral fluoroscopic image demonstrating slip progression of the spondylolisthesis to grade IV while on the operating room table. (B) Lines have been placed to outline the posterior margins of the vertebral bodies of L5 and S1 to help clarify the slip.
The wound was then packed and the skin closed with staples followed by placement of a sterile sealed dressing. The patient was then carefully flipped and transferred back onto a hospital bed. The operating room table was then switched to a flat-top operating table with an adjustable bolster frame. The patient was then rolled into the prone position onto the bolster frame, which was then elevated to maximum height, creating flexion at the lumbosacral level. Another fluoroscopic image was taken, revealing that the slip had reduced back to a grade II (Figs. 4A, B). A partial reduction was obtained by repositioning the patient in a more flexed position.
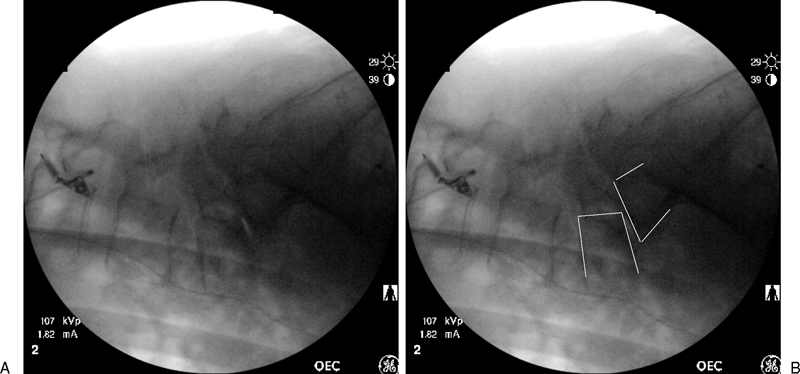
(A) Intraoperative lateral fluoroscopic image demonstrating reduction of the slip to a grade II spondylolisthesis following the repositioning of the patient in a more flexed position utilizing a bolster frame. Note the vacuum disk phenomenon seen at the L5–S1 disk following the reduction. (B) Lines have been placed to outline the posterior margins of the vertebral bodies of L5 and S1 to help clarify the slip.
Following repeat prepping and draping, the spine was again exposed and the decompression completed with laminectomy of L4 and L5 and bilateral foraminotomies at L5–S1. Pedicle screws were then placed within the pedicles of L4, L5, and S1 bilaterally. Titanium rods were then contoured to fit within the heads of the L4 and S1 screw and were locked into position. While locking the L5 pedicle screws to the traversing rods, the L5 vertebral body was slowly reduced to an almost anatomic position (Fig. 5). There were no changes in intraoperative neuromonitoring during the case. The spine was then decorticated, and both allograft and local autograft were placed.
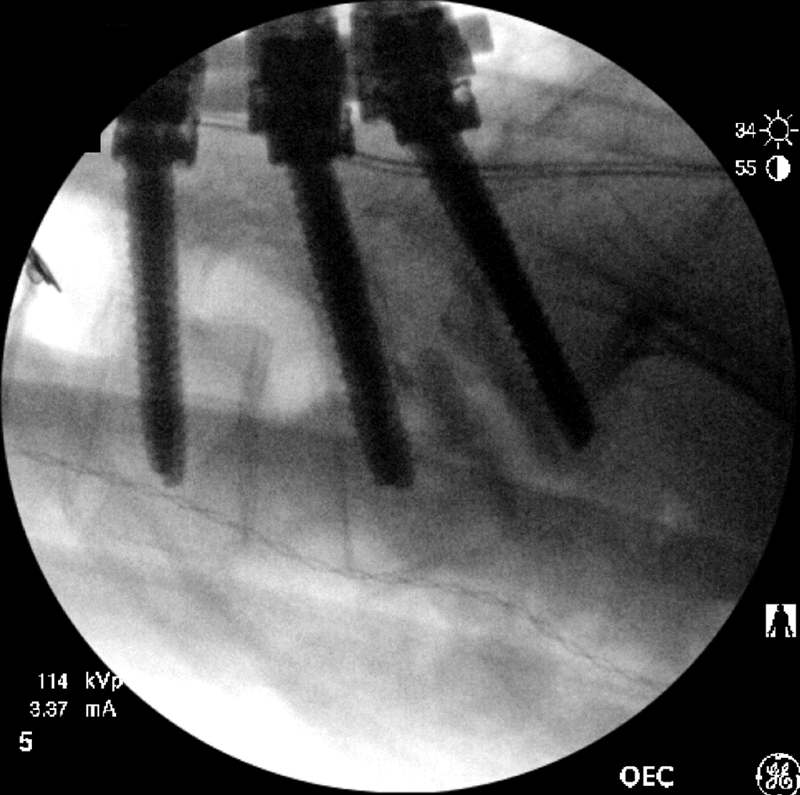
Intraoperative lateral fluoroscopic image demonstrating near anatomic reduction of the L5–S1 spondylolisthesis following instrumentation from L4–S1.
Immediately postoperatively, the patient was neurologically intact and reported improvement in her bilateral lower extremity radicular symptoms (Fig. 6). At 3 months postoperatively, the patient reported complete resolution of her radicular symptoms and remained without neurological deficit.
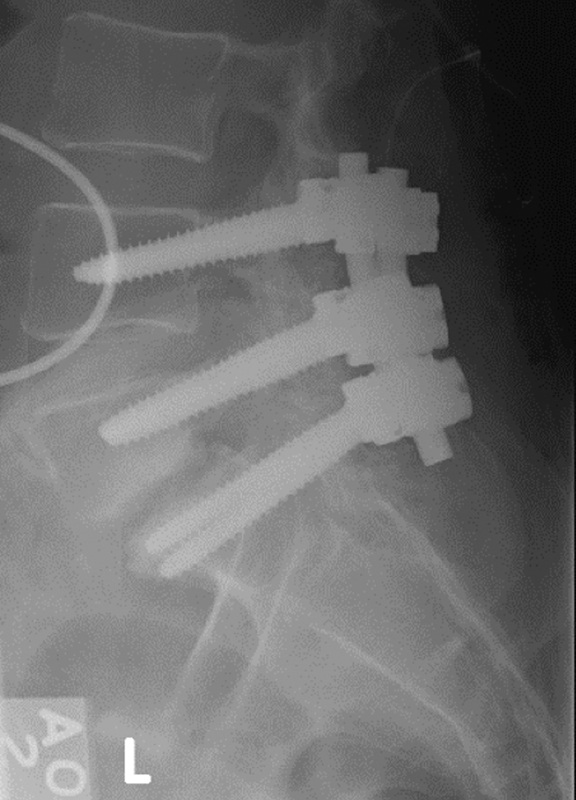
Upright lateral radiograph of the lumbar spine taken postoperatively demonstrating maintenance of the reduction achieved during instrumentation.
Discussion
When considering options for surgical treatment of adult isthmic spondylolisthesis, the surgeon must consider several different options, such as decompression, fusion, instrumentation, reduction, and type of bone graft to be used. All of these decisions must be individualized as deemed appropriate for each particular patient. When symptomatic, radiculopathy is the typical complaint in adults with isthmic spondylolisthesis, as in this patient. At the L5–S1 level, the slippage causes encroachment on the foramen and compression of the exiting L5 nerve root. When the patient presents with radicular leg pain, decompression is a favored choice for surgical treatment. 7 , 8
In adult patients with symptomatic low-grade isthmic spondylolisthesis, decompression and in situ fusion have been effective, although the addition of posterior instrumentation has also been shown to be beneficial. 9 , 10 , 11 , 12 , 13 The pathology in high-grade spondylolisthesis involves focal kyphosis at L5–S1 with hyperlordosis just above L5. This scenario can cause pain, facet joint arthrosis, and foraminal stenosis. Advanced degenerative disk disease at L5–S1 may also cause further instability and pain. Although it is generally accepted that symptomatic high-grade slips in adults require surgical stabilization and may benefit from partial reduction, there are no clear guidelines regarding the best approach for obtaining these goals 14 , 15 (i.e., posterior alone versus anterior-posterior procedures).
We are unable to explain the occurrence of this slippage after boney exposure alone without decompression. A literature search did not yield any biomechanical or clinical studies to help explain this occurrence. We can only speculate that a combination of factors, such as general anesthesia, prone positioning with the abdomen hanging free, muscle relaxation, and soft tissue dissection, may have facilitated the slip.
Partial reduction of a high-grade slip can have some benefits; it facilitates direct foraminal decompression and improves sagittal alignment of L5 on S1. The patient discussed in this report demonstrated remarkable instability when placed on the operating room table. This may have been a combination of her lumbosacral kyphosis associated with advanced degeneration of the disk below her pars defects. A partial reduction was obtained by repositioning the patient in a more flexed position and a complete reduction was easily obtainable during instrumentation, which may suggest gross instability at that level. Despite reported risk of neurological injury following complete reduction, this patient had complete resolution of her radicular symptoms with no neurological deficits postoperatively.
Conclusions
Adult isthmic spondylolisthesis most commonly occurs at the L5–S1 level of the lumbar spine. Slip progression is relatively rare in adults with this condition, and slippage is typically associated with advanced degeneration of the disk below the pars defect. When symptomatic, radiculopathy is the typical complaint in adults with isthmic spondylolisthesis. This report presented a case of intraoperative slip progression of an L5–S1 adult isthmic spondylolisthesis to a high-grade slip, which was treated with surgical reduction and posterior instrumented fusion. A complete reduction was achieved. The patient had complete resolution of her symptoms postoperatively without neurological deficits. This case demonstrates the potential instability that may be encountered when operating on patients with this condition.
Disclosures
Mark M. Mikhael, None
Gary S. Shapiro, None
Jeffrey C. Wang, Royalties: Medtronics, Stryker, Seaspine, Osprey, Aesculap, Biomet, Amedica, Zimmer, Synthes; Stock Ownership: Fziomed; Private Investments: Promethean Spine, Paradigm Spine, Benevenue, NexGen, K2 Medical, Pioneer, Amedica, Vertiflex, Electrocore, Surgitech, Axiomed; Board of Directors: North American Spine Society, Cervical Spine Research Society, AO Spine/AO Foundation; Scientific Advisory Board: VG Innovations, Corespine, Expanding Orthopaedics, Syndicom, Osprey, Amedica, Bone Biologics, Curative Biosciences, PearlDiver, Inc., Pioneer, Seaspine