
Abstract
Low-lying cord is an uncommon entity, and cord compression due lumbar disc disease is rarely encountered. We discuss our experience with a case of lumbar cord compression secondary to a large disc protrusion, which caused myelopathy in a low-lying/tethered cord. A 77-year-old woman with known spina bifida occulta presented with 6-week history of severe low back pain and progressive paraparesis. Magnetic resonance imaging showed a low-lying tethered cord and a large disc prolapse at L2/3 causing cord compression with associated syringomyelia. Medical comorbidities precluded her from anterior decompression, and therefore a posterior decompression was performed. She recovered full motor power in her lower limbs and could eventually walk unaided. She had a deep wound infection, which was successfully treated with debridement, negative pressure therapy (vacuum-assisted closure pump), and antibiotics. Six months after surgery, her Oswestry Disability Index improved from 55% preoperatively to 20%. Posterior spinal cord decompression for this condition has been successful in our case, and we believe that the lumbar lordosis may have helped indirectly decompress the spinal cord by posterior decompression alone.
Spinal cord normally ends above or at the level of inferior aspect of L2 vertebral body in 95% of cases. Low-lying cord is usually associated with various forms of spinal dysraphism. It presents in childhood due to longitudinal traction that results in tethering of the cord. 1 Rarely, patients progress to adulthood with no neurological symptoms. In most of these cases, spinal degenerative conditions or precipitating factors such as trauma exacerbate neurological symptoms, and patients can then present with various forms of neurological deficit. 2
Tethered cord syndrome (TCS) is considered a clinical entity in patients in the presence of a low-lying cord, thickened filum terminale, or on occasion a lipomatous lesion seen on radiological imaging. TCS in adults is commonly associated with spina bifida occulta and can cause significant morbidity if not diagnosed and treated early. 3
We present the case of an elderly woman with known spina bifida occulta, who presented with progressive back pain and paraparesis of relatively short duration.
She had radiological evidence of lumbar disc herniation causing cord compression and a tethered cord. We discuss the possible pathophysiology of disc disease causing cord compression in the presence of a tethered cord/low-lying cord and the role of decompressive surgery to possibly resolve these symptoms.
Case Report
A 77-year-old woman with known spina bifida occulta presented to the emergency department with a 6-week history of severe low back pain and progressive paraparesis. She was able to walk only two to three steps and only with two helpers. She denied any bowel or bladder dysfunction.
She was previously asymptomatic and was aware of a hairy patch in the lower back since birth. Her medical comorbidities included diabetes mellitus (type II), hypertension, increased body mass index, and mitral regurgitation.
Neurological examination of the lower limbs revealed proximal lower limb weakness of MRC (Medical Research Council) grade 3 in L2, L3 myotomes and grade 4 in L4, L5, and S1 myotomes. Sensory examination was normal. Reflexes were brisk with upgoing plantars and three beats of clonus in the right foot.
Subsequent investigation with magnetic resonance imaging of the whole spine showed a low-lying tethered cord and a large disc prolapse at L2/3 causing cord compression with associated syringomyelia (Figs. 1, 2, and 3).
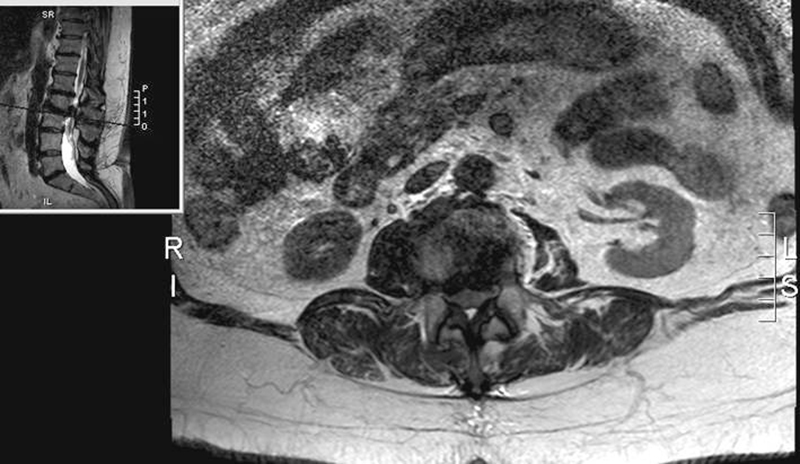
Axial view L2–L3 level.

Sagittal view T1-weighted image.

Sagittal view T2-weighted image.
The initial operative plan was to perform an anterior decompression, which may have entailed a corpectomy with bone graft and fusion. However, her extensive medical comorbidities increased the risk of perioperative morbidity. Consideration was given for posterior approach with the possibility of increased risk of wound infection due to the large lumbar pit and hairy patch, overlying the planned surgical wound. As posterior approach presented a significantly lower risk to the patient overall, a posterior decompression with a standard midline incision and laminectomy was performed at L2/3 under general anesthesia.
Following posterior decompression, the patient recovered full motor power in her lower limbs, and she could eventually walk unaided. In the early postoperative period, she had a deep wound infection, which was successfully treated with debridement, negative pressure therapy (vacuum-assisted closure pump), and antibiotics.
Follow-up in outpatient clinic 6 months after surgery, she was walking unaided and the wound had healed satisfactorily. Oswestry Disability Index showed an improvement from 55% preoperatively to 20%. Her upper motor neuron signs seen preoperatively had also resolved.
Discussion
TCS was described in last 3 decades and was previously associated only with the pediatric population. 4 Now, however, there is good evidence that it can occur even in adults and is much more common than previously thought. 1
Adults with TCS are considered to belong to two groups: those who were healthy in childhood but symptoms developed in adulthood or those who had static neurological deficits or skeletal deformities that were diagnosed in childhood but remained well until the onset of new and progressive neurological deficits in adulthood. 3 ,5 Other classifications included grouping them on basis of extent of spinal dysraphism6 or surgical outcome following detethering of the cord. 7
It has been shown that adults commonly present with varying neurological symptoms usually following a precipitating factor such as coughing, bending, or strenuous physical activity. It is thought that the mechanical longitudinal traction as a result of tethered cord causes these symptoms.
Many clinical series have found that these patients can present with a gradual, insidious onset of back pain, nondermatomal leg pain, burning pain in the buttocks and perineal region, and bowel and/or bladder dysfunction. 1 , 2 , 4 , 7 They can mimic symptoms of lumbar disc disease or spinal stenosis. There are some reports of symptoms being aggravated due to disc disease. 8
The recommended treatment is to detether the cord and excise any lesion. 1 , 2 , 3 Though the role of surgery is controversial, it has been shown that surgical detethering in the presence of neurological deterioration has been of some benefit. Motor weakness and pain seem to resolve though the return of sensory deficit, and return of bladder function varies. 4 Some surgeons have even questioned the role of detethering in the absence of symptoms and whether it would alter the natural history of TCS. 9
Our hypothesis is that the neurological deficit in this patient was likely secondary to the prolapsed disc. Owing to the natural lordosis of lumbar spine, posterior decompressive surgery may have allowed the spinal cord and neural elements to fall back and therefore relieved anterior cord compression. Upper motor neuron signs and myelopathy are not usually seen with lumbar disc prolapse when the cord is in the normal position. However, in the presence of low-lying cord, this could result in signs of cord compression with resulting myelopathy or upper motor neuron signs. This is the first case we know of that describes the management of lumbar cord compression with progressive neurological deficit. Posterior decompression appears to have provided a satisfactory outcome in this case.
Disclosures
Shreya Srinivas, None
Rohit Shetty, None
Iona Collins, None