
Abstract
The objective of this article is to report a case of a patient with ankylosing spondylitis who sustained a fracture through a prior solid arthrodesis without loosening or changing posterior instrumentation. There have been few cases reported of a patient with ankylosing spondylitis suffering a fracture through a prior instrumented arthrodesis. None have noted the instrumentation remaining intact with the fracture through the middle of the construct. The surgeon must be aware of this possibility to avoid spinal instability that may lead to a neurological deficit. We retrospectively reviewed the case. A review of the literature was performed through a PubMed search. A patient was found to have a fracture within a prior construct despite the presence of a posterior instrumentation. The mechanism of failure was a three-column spine fracture with “bending” of the rods. This patient was treated with a revision posterior/anterior instrumentation and fusion with placement of larger-diameter rods for added stiffness. Fractures through a prior instrumented arthrodesis are rare but still can occur in the ankylosing spondylitis patient. Given the higher risk of epidural hematoma and neurological compromise in this patient population, the surgeon must keep this on the differential diagnosis when treating patients with a prior instrumented arthrodesis.
Ankylosing spondylitis is a seronegative inflammatory disease that affects the axial skeleton. It results in fusion of the intervertebral disc as well as the facet joints. This fusion of the spine results in the spine acting like a long bone that is prone to fractures when subjected to a bending or torsional moment.
Materials and Methods
A retrospective review of the medical records and radiographic imaging was performed. Permission to review and present this information was obtained from the patient.
Case Report
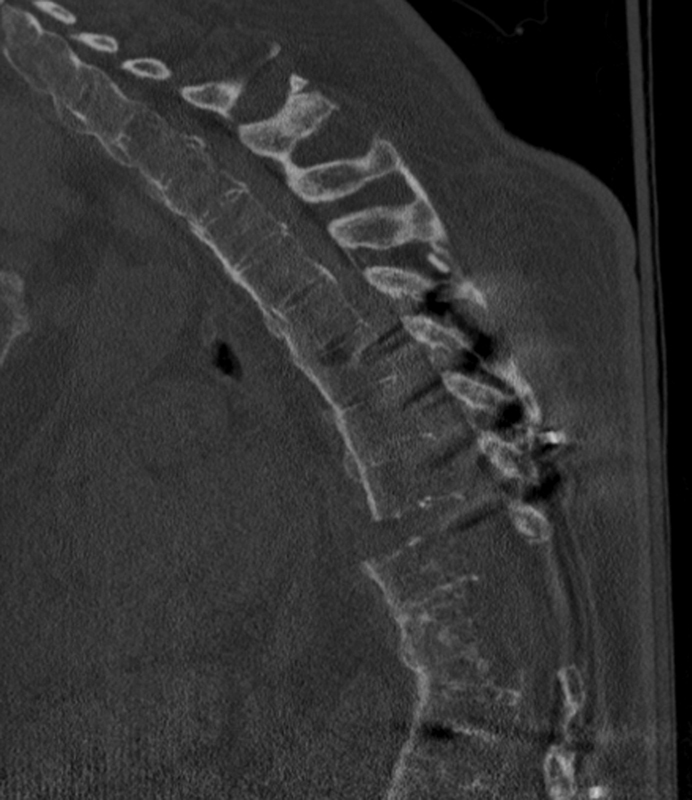
In 2004, a 65-year-old man sustained a fall from standing height in which he suffered a T10 compression fracture with significant local kyphosis (Figs. 1 and 2). Computed tomography (CT) myelogram showed marked canal stenosis at the level of the fracture. The patient underwent a partial posterolateral vertebral column resection and T9–11 laminectomy with instrumented fusion from T6 to L3 (Fig. 3). The patient did well postoperatively and was followed as an outpatient until a solid arthrodesis was obtained.
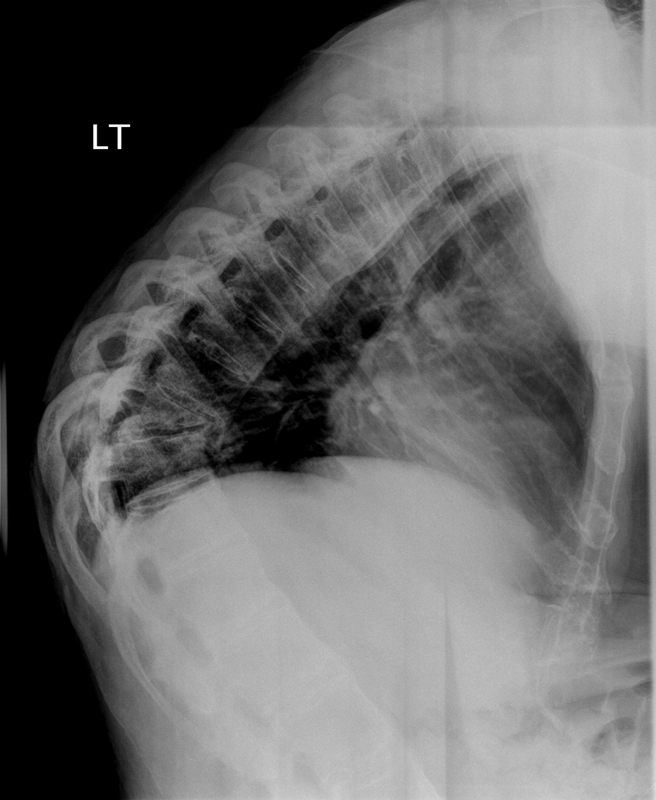
Lateral radiograph showing T10 fracture with significant local kyphosis.

Sagittal reformat of a computed tomography myelogram showing T10 fracture with spinal canal stenosis.

Postoperative lateral radiograph after T9–11 laminectomy and T6–L3 posterior fusion. Overall kyphosis at this time measured 61 degrees.
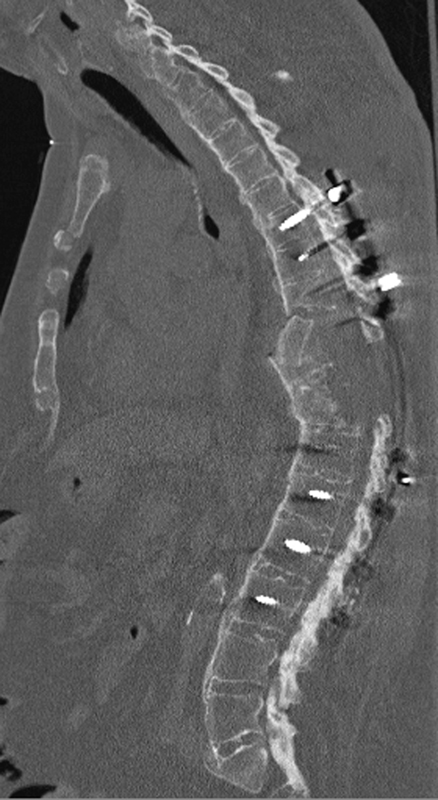
Five years after this surgery, the patient presented to the emergency department complaining of severe back pain following another fall. CT scan showed an extension-distraction injury at T10 (Fig. 4). Despite the presence of a fracture in the middle of the prior T6–L3 construct, none of the pedicle screws appeared to be loose. Close examination of the CT scan showed no lucencies around the pedicle screws suggesting loosening of the screws, nor was there any evidence of screw breakage. Measurement of the kyphosis over the entire T6–L3 construct was 51 degrees. The overall kyphosis from T6–L3 was found to be 68 degrees on postoperative imaging from his index procedure in 2004 (Fig. 5). This change in local kyphosis was interpreted that the mode of failure was a three-column bony injury with “bending” of the rods themselves or loosening of hardware not appreciated on imaging. A decrease in overall kyphosis can occur with bending of the rods resulting in extension of the entire spinal segment. In this sense, the pedicle screw instrumentation remained intact and solidly in place, but bending of the rods allowed for enough motion through the fusion mass and construct that a refracture of T10 occurred.
Sagittal reformat of computed tomography scan in 2009 after fall resulted in refracture through fusion mass and extension-bending of the rods. Overall kyphosis at this time measured 45 degrees. Sagittal plane bending of the rods in an extension direction will result in a decrease in overall kyphosis angle.
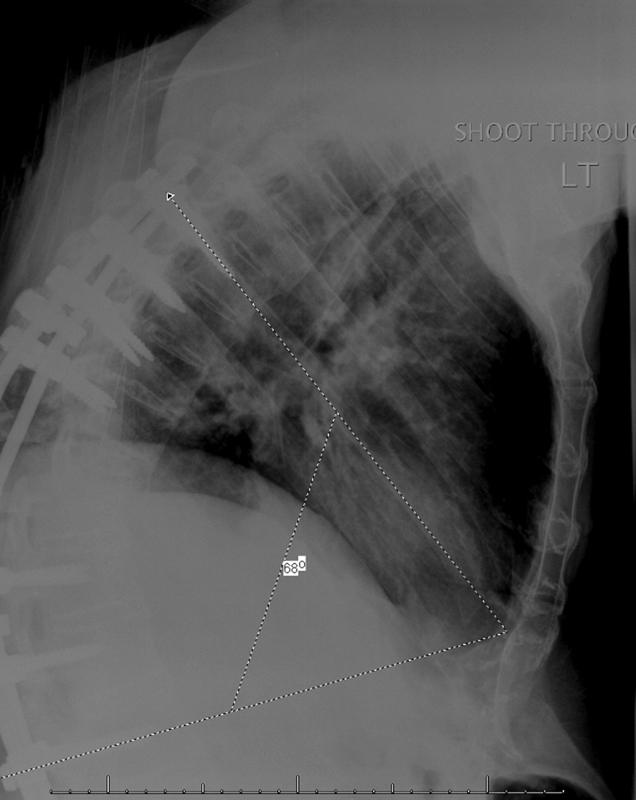
Postoperative lateral plain film from index surgery prior to reinjury showing overall kyphosis of 68 degrees.
This interpretation of the preoperative imaging studies was confirmed intraoperatively. After exposing and removing the rods and cross-connectors, all pedicle screws were found to be solidly in place. This posterior instrumentation was replaced with larger screws and a quarter-inch rod.
A postoperative CT scan after this posterior revision surgery showed a persistent distraction of the anterior and middle columns. Due to concerns for compromised axial load-bearing ability and subsequent possible further instability, this patient underwent an anterior partial corpectomy of T8 and T9 with placement of an iliac crest allograft (Fig. 6).
Postoperative computed tomography scan after revision posterior fusion and anterior corpectomy with placement of iliac crest allograft.
The patient was last seen at 3-month follow-up. All incisions are healed, the instrumentation is intact, and the patient has gone on to develop a solid arthrodesis. He is clinically doing well and was allowed to return to work and activity as tolerated.
Discussion
Ankylosing spondylitis is a seronegative inflammatory disease that affects the axial skeleton. 1 It can lead to fusion of the facet joints, as well as the intervertebral disc, into a fixed, hyperkyphotic posture. In addition to this sagittal plane imbalance, patients with ankylosing spondylitis often have generalized osteopenia, making them prone to spinal fractures after even minor trauma. 2 These spinal fractures are often missed on plain radiographs due to distortion of normal anatomy and occasional difficulty with patient positioning. For this reason, CT scans are often recommended to exclude a fracture in any patient with ankylosing spondylitis. 3
Spinal fracture in ankylosing spondylitis usually occur at the cervicothoracic junction, 4 but can also affect the thoracic and lumbar spine. 5 These fractures have a higher risk of neurological compromise due to the higher incidence of epidural hematoma as well as the possibility of translation at the newly mobile fracture site. 1 , 6 Operative fixation of spinal fracture in the ankylosing spondylitis patient often involves multiple points of fixation, usually at least three levels above and below the fracture site. The rate of pseudarthrosis is low as these patients have a predilection to spinal arthrodesis.
Fractures through a fusion mass have been reported in noninstrumented and instrumented fusions for idiopathic scoliosis. 7 , 8 Fractures of bones with prior instrumentation are most likely due to a nonunion of a fracture or pseudarthrosis of the attempted fusion. However, our patient represents a different mode of failure. Our patient did not develop a pseudarthrosis that led to hardware failure and failure of the entire surgical construct. He did not develop a nonunion of his thoracic fracture that led to hardware failure. On all preoperative imaging studies, the hardware appeared to be intact, unbroken, and solidly seated in bone. Intraoperatively, all pedicle screws were solidly seated into bone, and the fusion mass appeared to be intact. On further review of the CT scans from this recent injury as well as the imaging from after his prior surgery, we noted that there was a difference in overall kyphosis. With all the pedicle screw instrumentation solidly in place, the most likely explanation for the mode of failure is that this patient sustained an extension-distraction injury in the middle of his prior construct that resulted in a three-column bony injury with bending of the rods. Revision surgery involved replacement of pedicle screws and use of a quarter-inch rod for increased stiffness of the construct. 9 Although fractures caudal to an arthrodesis in an ankylosing spondylitis patient have been described,1011–12 fractures within an instrumented arthrodesis have not.
Conclusion
Patients with ankylosing spondylitis develop generalized osteopenia and a fixed sagittal plane imbalance that predisposes them to spinal fractures. Operative fixation should involve treating the spine like a long bone in which multiple points of fixation are obtained. Despite a solid arthrodesis and well-placed instrumentation, patients with ankylosing spondylitis can still sustain a spinal fracture after minor trauma. In this case report, we present a patient who sustained an extension-distraction fracture in the middle of a solid instrumented arthrodesis. Careful vigilance must be maintained in ruling out spinal fractures in all patients with ankylosing spondylitis, even those with a preexisting instrumented fusion.