
Abstract
A two-and-a-half year-old male, domestic shorthaired cat was presented with a history of chronic expiratory dyspnoea, dysphagia and progressive weight loss. Thoracic radiography revealed a caudal mediastinal mass. Surgical exploration confirmed the presence of an abscess in the caudal mediastinum. Despite the good prognosis, euthanasia was performed at the owner's request and post-mortem examination revealed an abscess that had been caused by a grass awn located within.
The purulent to pyogranulomatous inflammation or abscessation in various body sites due to the migration of grass awns, also referred to as ‘grass awn disease’ (Brennan & Ihrke 1983, Lotti & Niebauer 1992, Frendin et al 1994, Frendin 1997, Frendin et al 1999), is a rather common occurrence in Greece, especially in hunting-breed dogs. In a large study originated in the USA, it has been found that 61% of all foreign bodies recovered from dogs and cats were of plant origin (Brennan & Ihrke 1983). The characteristic barbed shape of Hordeum spp may explain their invasive nature, although migration inside the body is passively facilitated by the animal's motion (Brennan & Ihrke 1983). Most commonly affected sites include the external ear canal, interdigital skin, perineal area, nasal cavity, third eyelid and the paralumbar area, though other locations such as the diaphragm have also been reported (Johnston & Summer 1971, Nicolson & Horne 1973, Hur 1974, Brennan & Ihrke 1983). In Greece, low humidity and long periods of draught during the summer are held responsible for the appearance of various conditions associated with foreign bodies of plant origin, mainly occurring in longhaired dogs. Grass awn disease is a rare clinical entity in cats, mainly because of their fastidious nature, grooming habits and limited exposure to awns (Brennan & Ihrke 1983) where the third eyelid, abdominal cavity and urinary bladder have been the only reported sites (Hur 1974, Brennan & Ihrke 1983). Free roaming cats are more often affected simply because they have access to the fields where Hordeum spp is abundant. In contrast, mediastinal masses are a common occurrence in the cat, especially in the cranial mediastinum (Walter 1987, Thrall 1994). Caudal space occupying lesions in the feline mediastinum may include neoplasms, foreign bodies or dilatation of the oesophagus, diaphragmatic or hiatal hernia, gastroesophageal intussusception, abscesses, granulomas or neoplasms (Biller 2000).
There is no other reference in the literature, at least to the authors' knowledge, describing a caudal mediastinal abscess in the cat associated with migrating grass awns, hence the ensuing report.
Case report
A two-and-a-half year-old, intact male, domestic short-haired cat, weighing 5 kg, was referred to the Department of Clinical Sciences of the Veterinary Faculty, Aristotle University of Thessaloniki, Greece because of dyspnoea, weight loss and dysphagia, the latter being of temporary character. The cat had an indoor-outdoor lifestyle, was current with vaccinations and prevention for endoparasites and ectoparasites and had been recently tested positive for FIV but negative for FeLV using a commercial ELISA test kit (IDEXX®, France). One month before admission, the cat was presented to a local practitioner with a history of fever, inappetence and depression of four-day duration. Clinical examination had detected pain elicited on deep palpation of the cranial abdomen. Enrofloxacin (Baytril; Bayer), prescribed at a dose of 10 mg/kg, SID, per os, for two days, resulted in no improvement, so exploratory laparotomy was performed on suspicion of a foreign body. However, no gross abnormality or foreign body was revealed. Enrofloxacin was administered for a further week, this time together with prednisolone (Prezolon; Minerva) at a dose of 1 mg/kg, SID, per os, resulted in the resolution of fever.
On admission, the only abnormality detected was an expiratory dyspnoea of moderate degree. Complete blood count and serum biochemistry results were within normal limits. Lateral radiographs of the thorax revealed, a large, well-demarcated and spherical soft tissue density (6×6×7.5 cm), with a gas shadow superimposed on it, in the caudodorsal mediastinum. The caudal vena cava was displaced ventrally and the cupula and right diaphragmatic interface were obscured, accordingly (Fig 1). The ventrodorsal radiograph (Fig 2) showed the density to have an adjacent to the midline position. There was also lateral displacement of the artery, bronchus and vein of the right caudal lung lobe, which appeared consolidated. A tentative diagnosis of localised caudal mediastinal mass lesion was made as no other abnormalities were detected in the abdominal radiographs.
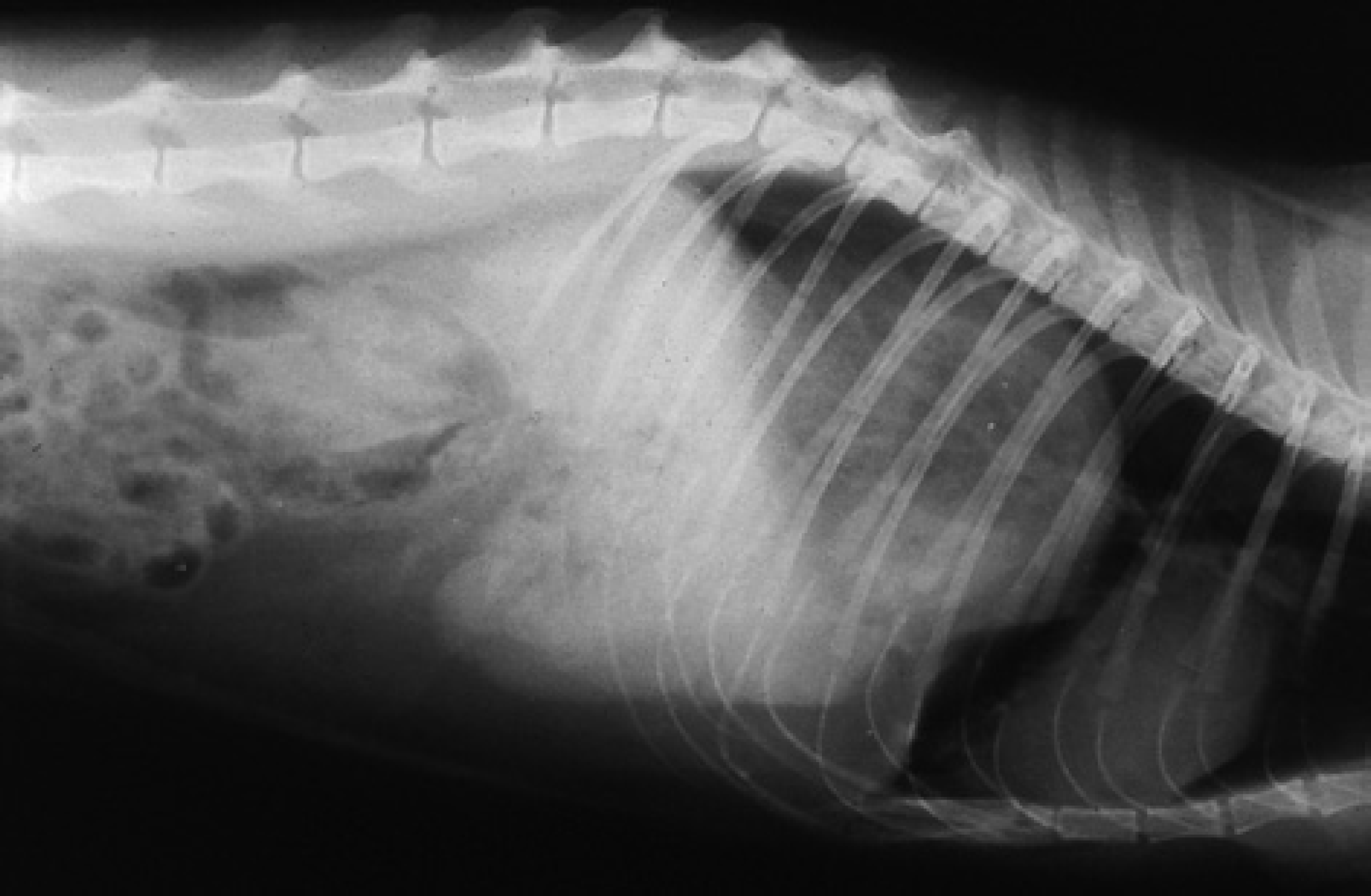
Lateral radiograph of the thorax showing a well-demarcated and voluminous soft tissue density in the caudodorsal mediastinum.
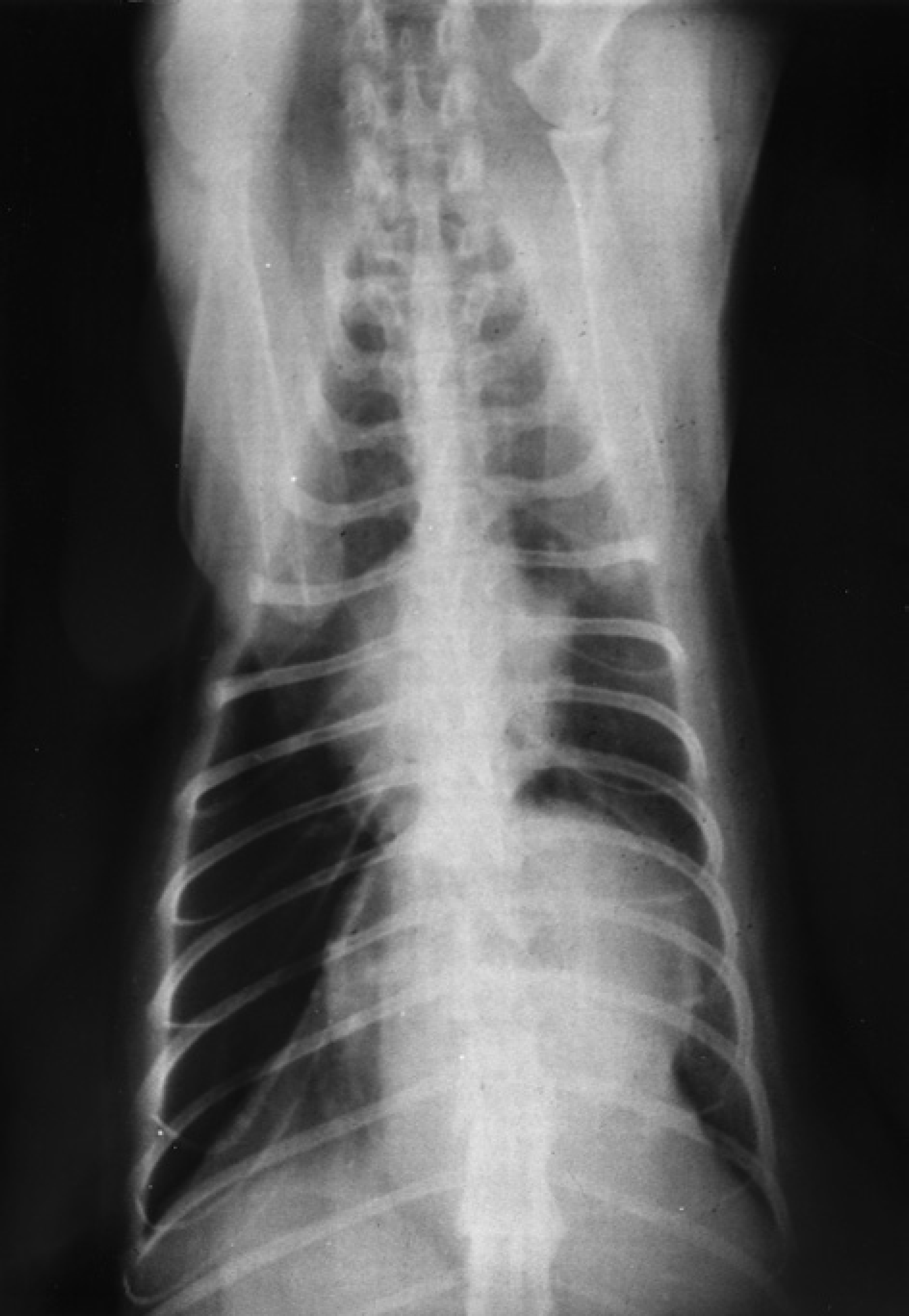
Ventrodorsal radiograph of the thorax depicting a soft tissue density in the caudal mediastinum.
Upon the owner's request, surgical exploration was carried out. Midline laparotomy extended to median sternotomy revealed a relatively large encapsulated mass in the caudodorsal mediastinum adjacent to the diaphragm. Fine needle aspiration cytology showed a large population of degenerated neutrophils and macrophages, suggestive of abscessation. Despite the favourable prognosis of the case after the would-be removal or drainage of the abscess, the owner requested euthanasia of the cat. At post-mortem, a thin-walled mass lesion, in close contact with the diaphragm and filled with a yellow-coloured purulent material, was found in the caudal mediastinum. Further exploration revealed a grass awn within it (Fig 3). No abnormalities were seen in the lung, the esophagus or the other structures of the thoracic cavity. Bacterial aerobic culture of pus on blood agar gave negative results.

On post-mortem examination a grass awn (Hordeum spp) located into the cavity of the caudal mediastinal abscess was revealed.
Discussion
In the feline cases described in the literature, there has been no explanation regarding the route of grass awn migration (Hur 1974, Brennan & Ihrke 1983). Grass awn ingestion and perforation of the oesophageal wall has been proposed as an underlying mechanism of thoracic cavity inflammation (Hur 1974). In our case, there has been clinical evidence that the grass awn had been ingested before perforating the oesophageal wall and lodging in the caudal mediastinum. Dysphagia, exhibited by the cat some days before admission, may further support this option. This sign usually indicates oesophageal disease when addressing the problem of mediastinal masses (Walter 1987).
Grass awn inhalation and migration through the bronchi and pulmonary parenchyma and pleural penetration have been proposed to cause mediastinal abscessation and pleuritis (Nicholson & Horne 1973, Horne 1981, Brennan & Ihrke 1983, Lotti & Nieubauer 1992, Frendin et al 1994, Frendin 1997). From our experience, this kind of awn migration into the body is common in dogs belonging to hunting breeds. In cats, migration through the airways should be considered much less probable because they rarely undertake open-mouth breathing. Indeed, the lack of coughing and the absence of lung pathology at post-mortem may support the oesophageal route. Moreover, evidence of a fibrotic cord connecting the pleural or pulmonary surface with the abscess, which has been described in cases of aerogenous grass awn invasion (Frendin et al 1994), was not found in this case. On the other hand, airway migration cannot be ruled out since the absence of pulmonary and/or bronchial lesions has been considered inconclusive evidence (Frendin 1997). The expiratory dyspnoea the cat exhibited could be attributed to the large size of the abscess and the subsequent compression of the lung lobes.
Ante-mortem diagnosis, based mainly on radiology and cytology, did not pose any particular difficulty in the present case. Oesophagography was not performed simply because there was no evidence of dysphagia on admission to our clinic. The presence of a foreign body abscess was one of the top differentials, as such lesions are often located exactly in the caudal-dorsal mediastinum, at least in the dog (Walter 1987). Further evidence of a localised inflammatory condition in this cat was the fever and the painful reaction elicited on palpation of its cranial abdomen.
Streptococcus spp, Staphylococcus aureus, Pasteurella multocida, Actinomyces spp, Nocardia spp and Fusobacterium spp are common isolates in the infections associated with migrating grass awns (Brennan & Ihrke 1983, Lotti & Niebauer 1992). In our case, both cytology and culture did not reveal bacterial involvement because of the lack of cultures for specific pathogens or the concurrent use of enrofloxacin at the time of the second surgical exploration.
With the surgical removal of the mediastinal abscess the cat would have probably experienced an uneventful recovery if the owner, for unexplained reasons, had not decided to have euthanasia performed. Since this curable entity shares many clinical and radiological characteristics with mediastinal tumours, it should be always considered in the differential diagnosis of intrathoracic disease, especially in geographical areas like Greece.