
Abstract
Reports on intervertebral disc disease in cats are rare in the veterinary literature. It has been postulated that intervertebral disc protrusion is a frequent finding during necropsy in cats, without having any clinical relevance (King and Smith 1958, King & Smith 1960a, King & Smith 1960b). However, a total of six cases with disc protrusions and clinically significant neurological deficits have been reported over the past decade. (Heavner 1971, Seim & Nafe 1981, Gilmore 1983, Littlewood et al 1984, Sparkes & Skerry 1990, Bagley et al 1995). As in dogs, there are also two types of intervertebral disc disease in cats: Hansen's type I (extrusion), and type II (herniation). Cervical spinal cord involvement was more commonly recognised in cats than the lumbar or the thoraco lumbar area. Cats over 15 years were mainly affected (King & Smith 1958, King & Smith 1960a, King & Smith 1960b). We describe two cats with lumbar intervertebral disc protrusions. Emphasis is placed on differential diagnoses, treatment and follow-up.
Cat 1
A six-year-old, castrated, male, oriental shorthaired cat was referred by a local veterinarian to the Clinic of Small Animals in Bern because of an abnormal hindleg gait and a flaccid tail. The clinical signs presented acutely over the 5 days prior to presentation. Meanwhile, the cat was treated with dexamethasone (Dexa-Tad; Tad) at a single dose of 2.5 mg/kg bodyweight (BW) iv, but no improvement of neurological signs was observed.
The general physical examination revealed no abnormalities. On neurological examination a plantigrade stance of the left hind limb, as well as a paresis of the tail were observed. Gait abnormalities included paraparesis, more pronounced on the left, and ataxia of both hind legs. All postural reactions, such as correction of knuckling of the paw and the extensor postural thrust reaction, were decreased in both hind limbs. The patellar reflex was increased on the left side and normal on the right. The tibialis cranialis and the flexor reflexes were decreased bilaterally, as were the perineal reflexes. No deficits in perception of noxious stimuli were found. Muscle atrophy of both hind limbs was recognised. The presumptive anatomical localisation was either a lesion in the caudal lumbar intumescence (L6–S1) or the cauda equina. Differential diagnoses for the former localisation included a space-occupying lesion such as neoplasia or a protruded disc, as well as fracture, luxation, fibrocartilaginous embolism and infectious/inflammatory diseases.
The blood cell count and serum biochemistry profile analysis revealed no abnormalities, and FeLV and FIV tests were negative.
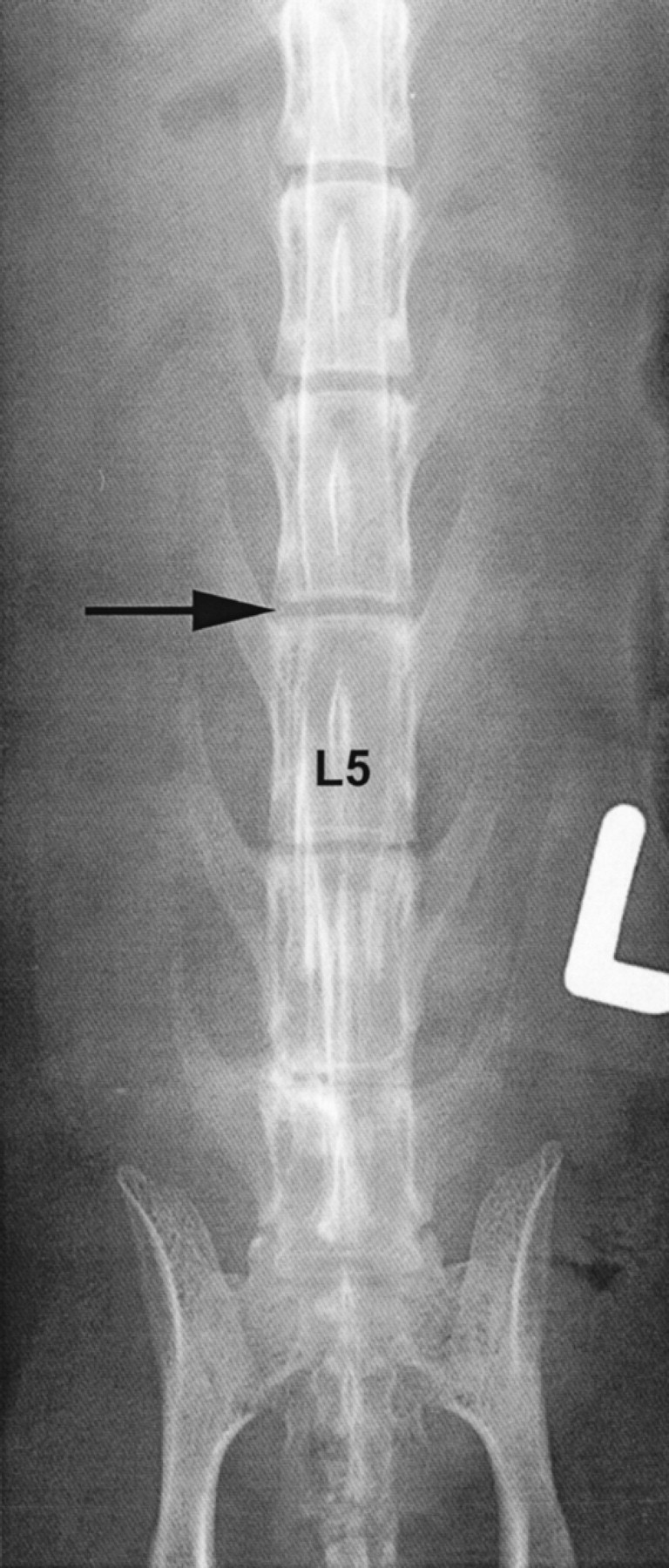
Thoracic plain radiographs were normal. Anaesthesia was induced with diazepam (Valium 10; Roche) at a dose of 0.25 mg/kg BW, iv and propofol (Disoprivan; ICI Pharm) at a dose of 5 mg/kg BW, iv and maintained with isoflurane (1–1.2%; Forene; Abott). Radiographs of the lumbosacral area showed a narrowed intervertebral disc space at the level of L6/L7. At the same location, calcification of the foramen intervertebrale was seen (Fig 1a). The subchondral boneplate of the caudal end of the vertebral body L6 and the cranial end of the vertebral body L7 showed a minimal thickening. The intervertebral disc space L5/6 was mineralised (Fig 1a). The CSF examination after cisterna magna puncture revealed no abnormalities (Pandy's test negative, 0/3 cells). On cisterna magna myelography the contrast lines stopped completely at the caudal quarter of the vertebral body L6. On the ventrodorsal oblique view the contrast lines showed a slight deviation to the right (Fig 1b). The radiographical findings were suggestive of an extradural compression of the spinal cord from the ventral aspect and from the left side, at the level of L6/7. A protruded disc was the most likely diagnosis. Due to the history and clinical signs, surgical decompression was the treatment of choice. A single dose of dexamethasone (2 mg/kg BW, iv; Dexa-Tad; Tad) was given preoperatively. A standard hemilaminectomy from the left side at the level of L6-L7 was performed. A substantial amount of disc material was removed from the vertebral canal. Intra-operative haemorrhage from the venous plexus was stopped by cold lavage with Ringers solution (Ringer-Lactat; Fresenius). Anaesthetic recovery was uneventful.

Lateral survey radiographs of the lumbar vertebral column showing a calcified intervertebral disc space at L5/6 and calcification within the foramen intervertebrale at the level of L6/7 (arrow).

Myelography, oblique view: stop and deviation of the contrast-line to the right; note the calcified disc at the level of L6/7 (arrow).
The cat showed a less plantigrade gait on the left rear limb and had spontaneous urination 24 h postoperatively. The patient was treated with cephalexin (Cefaseptin; Chassot) at a dose of 30 mg/kg BW, PO, BID for 10 days and prednisolone (Prednisolon; Chassot) at a dose of 1 mg/kg BW, PO, SID for 2 days and then 0.5 mg/kg BW, PO, SID for 3 days. The cat had daily manual physiotherapy such as massage and passive motion of the hind legs and was kept in a large box to permit the maximum of exercise. The cat improved constantly and was discharged 1 week after surgery. Two years later the cat was seen at our clinic for another unrelated problem. Only slight muscle atrophy of the hind limbs without gait or postural reaction abnormalities was observed at that time.
Cat 2
The second cat was a 12-year-old, spayed, female Persian that was referred without any treatment to our clinic with the major complaint of para-paresis and ataxia of the hind limbs. The clinical signs had a peracute onset and were non-progressive.
General physical examination revealed no abnormalities. Neurological evaluation confirmed a paraparesis and ataxia of the hind limbs. The spinal reflexes, such as the extensor and flexor reflexes, as well as the perineal reflexes were decreased. The decreased postural reactions and the decreased reflexes in the rear limbs were consistent with a lesion at the spinal cord segments between L3 and S3. Differential diagnoses included a space occupying lesion such as neoplasia (eg lymphoma) or inter-vertebral disc disease, as well as an infectious/inflammatory condition and trauma (fracture, luxation, subluxation).
The results of complete blood cell count and serum biochemistry profile, as well as thoracic plain radiographs were normal. The cat was FeLV and FIV sero-negative. Anaesthesia was induced with diazepam (Valium 10; Roche) at a dose of 0.5 mg/kg BW, iv, propofol (Disoprivan; ICI Pharm.) at a dose of 6 mg/kg BW, iv and methadon (Methadon; Streuli) at a dose of 0.2 mg/kg BW, iv and maintained with halo-thane (0.8–1%; Halothan; Halocarbon). The plain radiographs of the lumbosacral area were normal. CSF analysis revealed no abnormalities. On cisterna magna myelography the lateral view showed a thinning and splitting of the contrast line over the vertebral bodies L4 and L5 with a dorsal deviation (Fig 2a). The ventro–dorsal view showed that the contrast stopped over the vertebral body L4, with a slight deviation of the right contrast column to the left (Fig 2b). In addition, a linear tomogram suggested an additional intradural component with a triangle-shaped enlargement of the ventral contrast line at the level of L5. Extradural compression of the spinal cord with a possible intradural component at the level of L4/5 was the radiologic diagnosis. Differential diagnoses included space-occupying lesions such as neoplasia, disc protrusion and haematoma. Due to the history and clinical signs, surgical decompression and biopsy was planned. A single dose of dexamethasone (Dexa-Tad; Tad) at a dose of 2 mg/kg BW iv was given preoperatively. A routine hemilaminectomy at L4/5 from the right side was performed and a mass was removed. The spinal cord had a normal colour and the dura mater was intact. After cold lavage with Ringers solution (Ringer–Lactat; Fresenius), closure of the wound was routine. The removed extradural mass was examined histopathologically and showed blood, hyaline cartilage and pieces of dura mater. The diagnosis of disc extrusion was confirmed.

Lateral view: thinning and splitting of the contrast-line over L4/5 with dorsal deviation, indicating a ventral extradural compression at L4/5 (arrows).
Ventro-dorsal view: slight deviation of the right contrast column to the left at L4/5 (arrow).
The cat improved over the next 6 days with daily manual physiotherapy, such as massage and passive motion of the hind legs. On the seventh post-operative day the cat was discharged with slight residual paraparesis. Complete recovery was noted after two months.
Discussion
Several conditions should be considered in a cat with progressive or acute paraparesis. Lymphosarcoma is the most common disease affecting the spinal cord in cats (Northington & Julianna 1978), followed by aortic thromboembolism and trauma (Oliver 1997). Other considerations include focal meningomyelitis associated with feline infectious peritonitis (FIP), toxoplasmosis or cryptococcosis (Legendre & Whiteneck 1975, de Lahunta 1983, Kornegay 1983). Less commonly occurring spinal cord lesions include discospondylitis (de Lahunta 1983) and ischaemic myelopathy resulting from fibrocartilagonous thromboembolism (Zaki & Prata 1976, Turner et al 1995, Scott & O'Leary 1996). Intervertebral disc disease is a rare condition but it has to be considered in any paraparetic cat (Seim & Nafe 1981, Gilmore 1983, Sparkes & Skerry 1990, Bagley et al 1995).
Based on history and neurological findings, as well as radiographic results including myelography, lumbar intervertebral disc extrusion was diagnosed in two cats. Diagnosis was confirmed on histopathological examination in one cat. Both patients were successfully treated by surgical decompression and disc removal with post-operative physiotherapy. Thus, the prognosis seems to be rather good if surgical treatment as well as carefully conducted physical therapy, such as muscle massage and passive motion of the legs to maintain muscle mass and ranges of joint motion, is performed. Little information about the treatment of intervertebral disc protrusion in cats is available (Seim & Nafe 1981, Gilmore 1983, Sparkes & Skerry 1990, Bagley et al 1995). The authors believe that the guidelines of medical and surgical treatment for dogs can probably be used for the cat.
King and Smith's studies on disc degeneration in clinically normal cats identified two main types of disc degeneration in this species (King & Smith 1958, King & Smith 1964). Their findings are compatible with existing data in dogs (Hoerlein 1978). Few cats develop chondroid degeneration (calcified nuclei), while most show a more fibroid pattern of degeneration. Cat 1 showed mineralisation of two intervertebral disc spaces and cat 2 showed fibroid disc degeneration, which was confirmed histopathologically. Thus, it also seems that in cats with clinically relevant disc protrusion at least the fibroid disc degeneration is represented. Furthermore, the two cats suffered from a Hansen's Type I disc extrusion in the lumbar spinal cord region. Distribution in the other six cases was: three affected in the thoracolumbar region (2×T12/13, T13/L1) with acute onset, two in the cervical region (2×C5/6) and one with cauda equina signs (L6/7) with a chronic progressive history (Heavner 1971, Seim & Nafe 1981, Gilmore 1983, Littlewood et al 1984, Sparkes & Skerry 1990, Bagley et al 1995). In the veterinary literature Hansen's type II protrusion seems to be more common in the cervical spinal cord region in cats without clinical relevance (King & Smith 1958). In contrast to the findings in the veterinary literature, our cats suffered from intervertebral disc extrusion in the lumbar spinal cord region (King & Smith 1960a, b, King & Smith 1958). We can conclude that the cervical, thoraco-lumbar and lumbar spinal cord can be affected in cats producing clinical signs of intervertebral disc disease. The probability of clinically significant disc extrusion seems to be higher in the thoracolumbar and lumbar area. This could be explained by the relatively wider vertebral canal in the cervical area (Bojrab 1993). Additionally, these dorsal protrusions are observed frequently in cats over 15 years of age, indicating that the condition affects mostly older cats (King & Smith 1960a, b). Our cats were young, similar to all other reported cases with clinically significant disc protrusion (Heavner 1971, Seim & Nafe 1981, Gilmore 1983, Littlewood et al 1984, Sparkes & Skerry 1990, Bagley et al 1995). Our study indicates that intervertebral disc protrusion should be a differential diagnosis in young to middle aged cats with acute paraparesis.
An interesting finding is that pure breed cats appear to be overrepresented, as 50% of previously reported cases (two Siamese, one Russian Blue), in addition to our cats (Persian and oriental shorthaired) were pure breed cats (Heavner 1971, Gilmore 1983, Sparkes & Skerry 1990). But the number of cases is very small and several other factors (eg the likelihood of referral for surgical treatment) could be influential.
The recommended treatment is surgical decompression, disc removal and post-operative physiotherapy. The physiotherapy programme involves massage and passive motion of the affected limbs, as well as keeping the cat in a large box to permit the maximum of exercise. The prognosis in surgically treated cats is fair to good.