
Abstract
A cross-sectional survey of a convenience sample of cats was carried out to determine the prevalence of and risk factors for respiratory tract disease, feline calicivirus (FCV) infection and feline herpesvirus (FHV) infection. Seven hundred and forty cats were studied; samples for isolation of FCV and FHV were obtained from 622 (84%). Data on individual cat and household variables were obtained by questionnaire for each cat and analysed using univariable and logistic regression analysis. Thirty-eight percent (282/740) of cats surveyed had respiratory tract disease. Eighteen of 24 predictor variables were found to be significantly (
Infectious respiratory disease in cats is a common clinical problem. The major recognised causes of feline upper respiratory tract disease (RTD) are feline herpesvirus-1 (FHV) and feline calicivirus (FCV) (Gaskell & Dawson 1994). Other agents, including
Despite the fact that vaccination has been practised routinely against FHV and FCV for about 20 years, the viruses are still prevalent in the feline population both in healthy cats and in cats with RTD. Several surveys have evaluated predisposing factors for the presence of respiratory virus infection and some have demonstrated gender, age and breed predilections. In particular, higher prevalences of FCV and FHV appear to be associated with cats of less than 12 months, and for FCV, households with greater numbers of cats (Wardley et al 1974, Coutts et al 1994). Few studies have attempted to identify and measure the risk factors for feline upper respiratory tract disease, however. It has been suggested that factors such as the age of the cat at the time of first exposure to an infectious agent, the virulence of the infecting strain, the degree of challenge, the presence of intercurrent illness, the immune and nutritional status of the cat, the population density, and the level of stress in the group may be involved in the development of respiratory disease (August 1990, Pedersen 1988, Gaskell & Dawson 1994).
The aims of this study were to identify the risk factors associated with the presence of respiratory tract disease, infection with FCV and infection with FHV. The inferences drawn may be useful in devising control schemes for intensively housed cats such as those that form the majority of the study sample. The study also examined the role of
Materials and Methods
Sampling of cats and viral isolation
A convenience sample of 740 cats were recruited into the study during the period May 1994 to November 1995, as previously described (Binns et al 1999). Questionnaires designed to measure possible risk factors for respiratory tract infection were completed for each animal. Some samples were obtained from cats with missing data on the questionnaire; all observations are therefore taken as a proportion of the cases with the appropriate information available.
Oropharyngeal swabs were taken by veterinary surgeons from 622 cats in their normal cattery environment or when cats were brought into veterinary surgeries. A plain sterile swab was used and placed immediately into virus transport medium for isolation of FCV and FHV as previously described (Coutts et al 1994).
Viral isolation was carried out on duplicate confluent monolayers of feline embryo or Crandell feline kidney cells, as described previously (Coutts et al 1994). Briefly, 100 μl of the swab transport medium was inoculated onto the cells for 1 h at 37°C, after which the cells were refed with maintenance medium (Eagle's MEM with 1% fetal calf serum [FCS], 50 iu/ml penicillin, 50 μg/ml streptomycin, buffered with sodium bicarbonate) and incubated in a 37°C, 5% carbon dioxide atmosphere. Cell cultures were examined daily for the characteristic cytopathic effects of FCV and FHV. All samples were passaged at least once before being reported as negative.
Predictor variables
Three outcome variables were used: the presence of RTD in the cat; isolation of FCV from an oropharyngeal and/or nasal swab sample from a cat; and isolation of FHV from a cat. Twenty-nine predictor variables (Binns 1997) were used with each outcome variable. Predictor variables relating to an individual cat included age (categorised into five groups), gender, antibiotic therapy within 2 weeks prior to sampling, vaccination history and pedigree status (Binns et al 1999).
Household-related predictor variables included the number of cats, the presence of other animals, and the type of colony (category 0=rescue cattery; category 1=breeding colony; category 3=others, eg pet cat household). A multi-cat household was defined as a household or cattery containing more than one cat (the number of cats was categorised into five groups; 0–1 cats, 4–10 cats, 11–20 cats, 21–50 cats and >50 cats). The presence of RTD, or history of such disease, in any cat in the household was also recorded.
Assignment of clinical scores
Clinical signs of respiratory or ocular disease were recorded and assigned scores as previously described (Binns et al 1999). Clinical scores were allocated according to the clinical signs described in the literature (Gaskell & Dawson 1998). Sneezing, coughing and dyspnoea were each assigned a score of three; ocular discharge, conjunctivitis and oral ulceration were assigned a score of two; and anorexia, pyrexia and hypersalivation were assigned a score of one. A cat was defined as having respiratory disease if the sum of its scores was three or above.
Statistical analysis
Univariable analysis was carried out using Epi Info v. 6.02 (Dean et al 1994). Data were entered into a computer database and 2×2 contingency tables and Yates' corrected chi-squared tests were used. Fisher's exact test was used if the expected value in a cell in the contingency table was lower than five. The unadjusted odds ratio, with Cornfield 95% confidence intervals (95% CIs), was calculated for each combination of predictor and outcome variable. Continuous variables for age and number of cats in household were categorised and analysed in 2×
Due to the number of potential confounding variables, logistic regression analysis was carried out to investigate the relationships between the predictor and outcome variables. Logistic regression analysis was also carried out (EGRET 1990). Variables were selected for inclusion in the logistic regression analysis if the
Regression diagnostics were carried out for each model by calculation of the delta-beta values: the change in the calculated regression coefficient for each variable and each case in the model (Hosmer & Lemeshow 1989). Cases with high values of delta-beta for any variable (those cases with significant leverage on the value of the coefficient) were excluded from the model and the model refitted to check its stability.
Results
Characteristics of study sample
The details of the sample population have been previously described (Binns et al 1999). A total of 740 cats were included in the survey, of which 622 (84%) were sampled for respiratory virus isolation. A total of 282/740 (38%) cats surveyed were classified as having current upper RTD, as defined by the clinical score. The clinical signs reported in these 282 cats included sneezing (79.9%), ocular discharge (53.7%), nasal discharge (51.4%), conjunctivitis (30.6%), coughing (27.6%) and dyspnoea (20.4%). Pyrexia, inappetence, oral ulceration and hypersalivation each occurred at a frequency of less than 20%.
Isolation of FHV and FCV
Overall, FCV was isolated from 162/622 (26%) of cats, and FHV from 30/622 (5%) (Table 1). Three cats were positive for both viruses, giving a total of 189/622 (30%) cats positive for one or both viruses. The isolation rates for FCV and FHV in cats with RTD were 81/244 (33%) and 27/244 (11%), respectively; in cats with no current RTD the isolation rates were 45/201 (21%) and 2/201 (1%), respectively. One hundred and thirty-one of 506 fully vaccinated cats (26%) were shedding FCV, whereas only 14 (3%) were shedding FHV. Twenty-four of 81 (30%) non-vaccinated cats were shedding FCV and 13/81 (16%) were shedding FHV (data not shown).
Prevalence of infectious agents in cats with and without respiratory tract disease

Overall 82 of 740 (11%) cats were positive for
Univariable analysis of predictor variables
Univariate relationships between predictor variables and feline respiratory tract disease
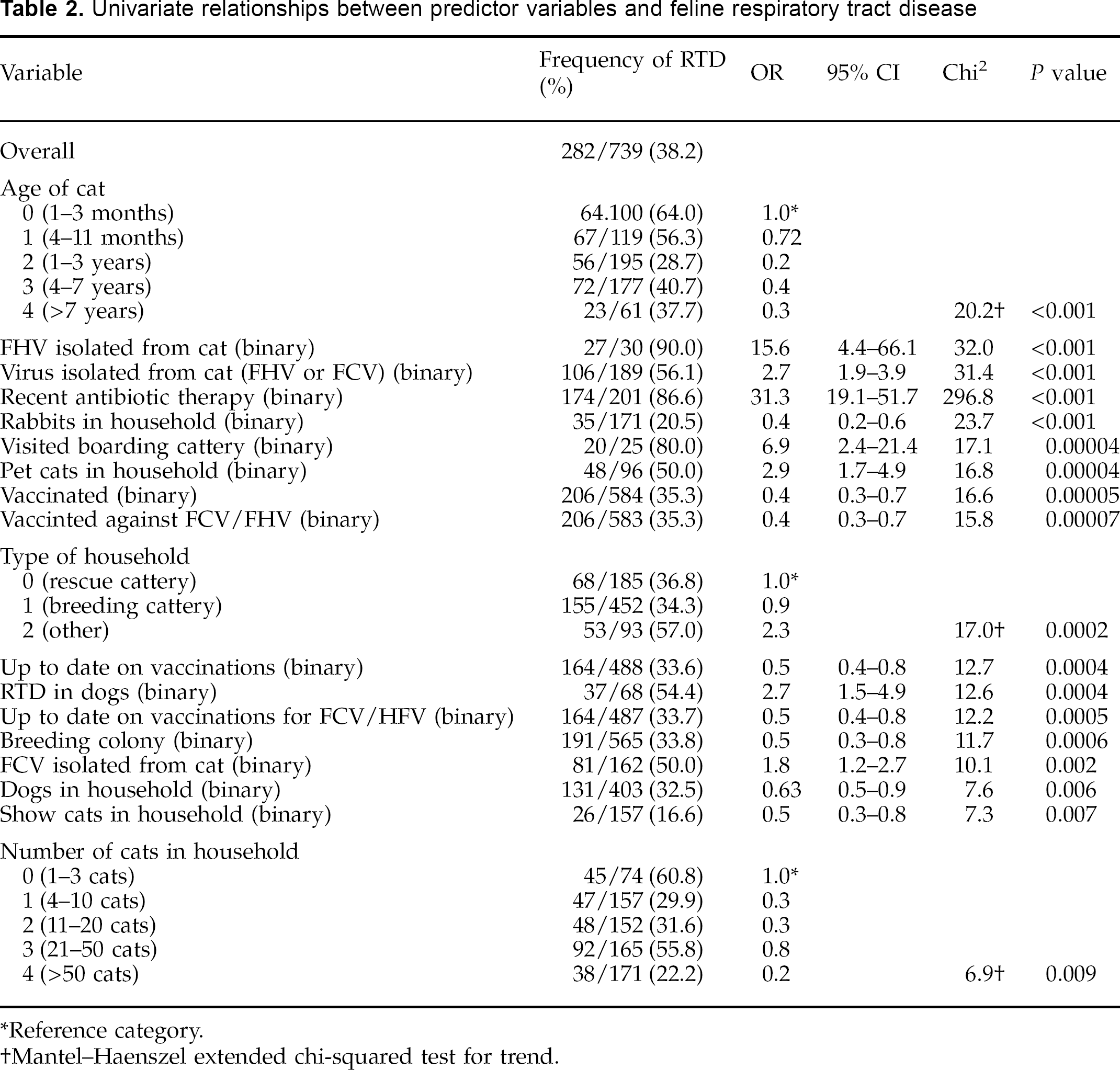
Reference category.
Mantel–Haenszel extended chi-squared test for trend.
A number of household or environment-related factors were found to be associated with respiratory tract disease; there was a positive association with cats kept in research colonies and pet households (category ‘other’), compared with breeding colonies and rescue catteries (Table 2). Households containing smaller numbers of cats (χ2 for trend=6.9;
The presence of healthy and/or diseased dogs in the household was negatively associated with current respiratory disease in the cats (χ2=7.6;
Univariate relationships between predictor variables and FCV isolation

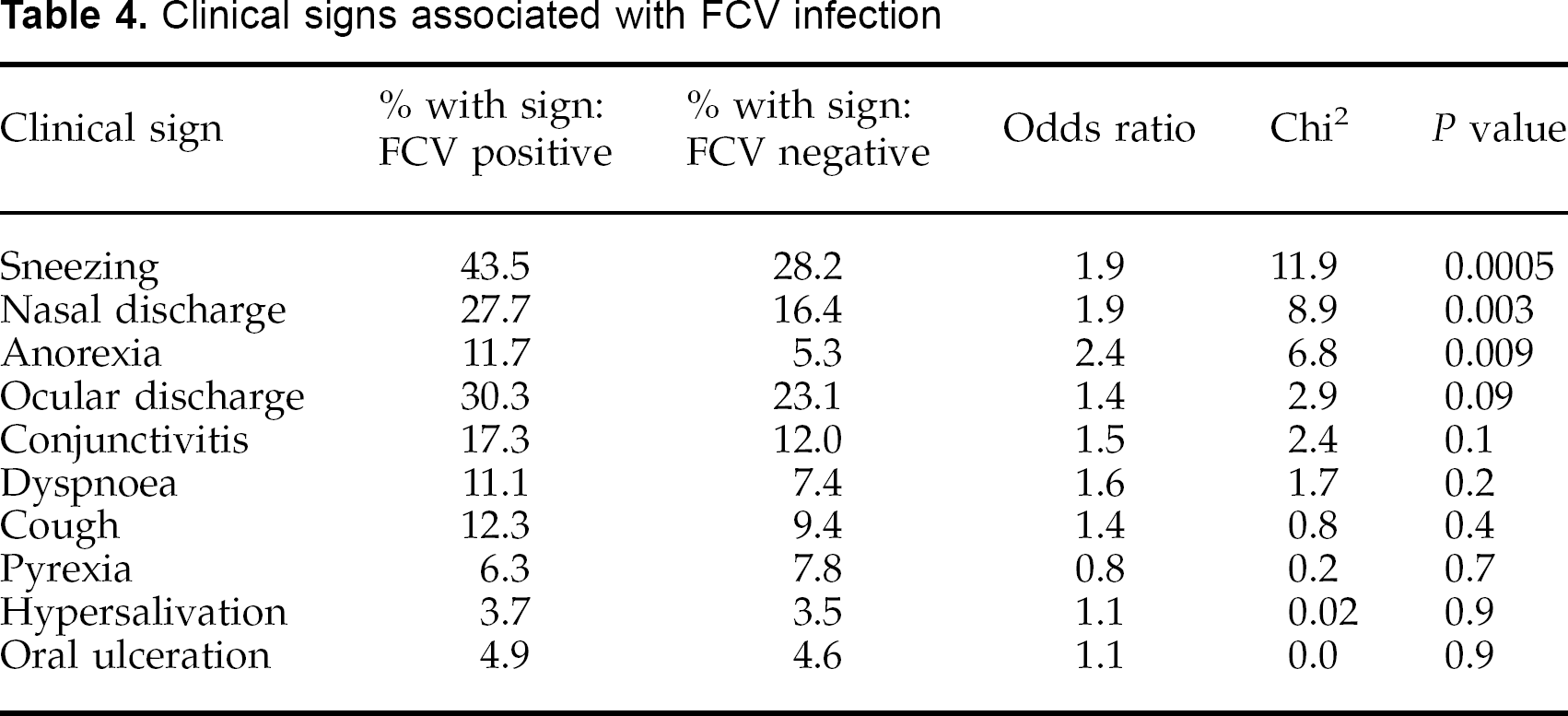
Clinical signs associated with FCV infection
Univariate relationships between predictor variables and FHV isolation

Reference category.
Mantel-Haenszel extended chi-squared for trend.
Fisher Exact test.
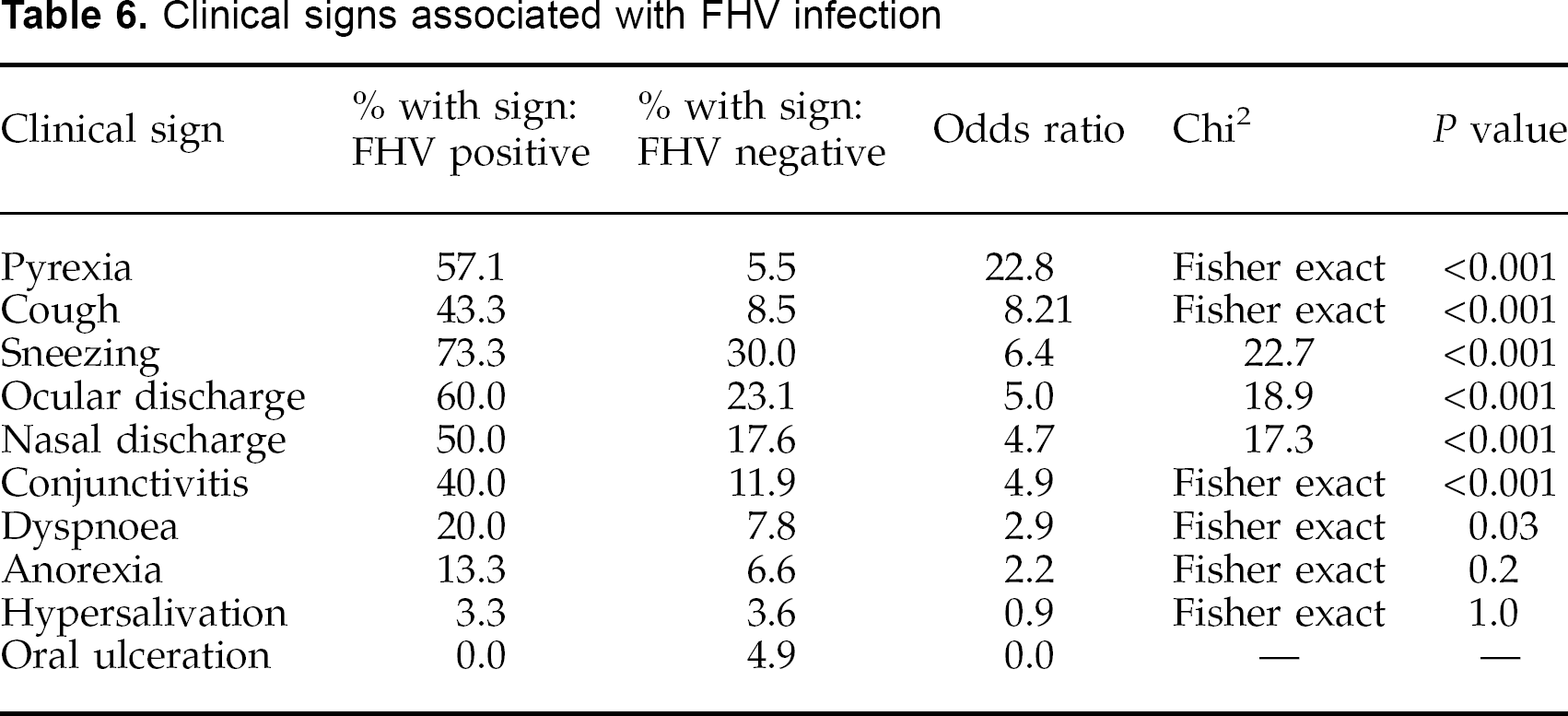
Clinical signs associated with FHV infection
Although most of the predictor variables found to be associated with FHV in univariable analysis related to the individual cat rather than the household, the presence of either rabbits (OR=0) or dogs (OR=0.35) in the household was negatively associated with herpesvirus isolation from a cat. As with FCV, there was no association between the number of cats in the household (χ2 for trend=0.92,
Logistic regression analysis
Respiratory tract disease
Logistic regression. After adjusting for confounding seven predictor variables were found to be significantly associated with feline respiratory tract disease in this model (Table 7); isolation of FHV and FCV were independently associated with RTD, kittens (4–11 months) and catteries (21–50 cats) were also positively associated with RTD.
Multivariate relationships between predictor variables and respiratory disease using ordinary logistic regression (n=426)

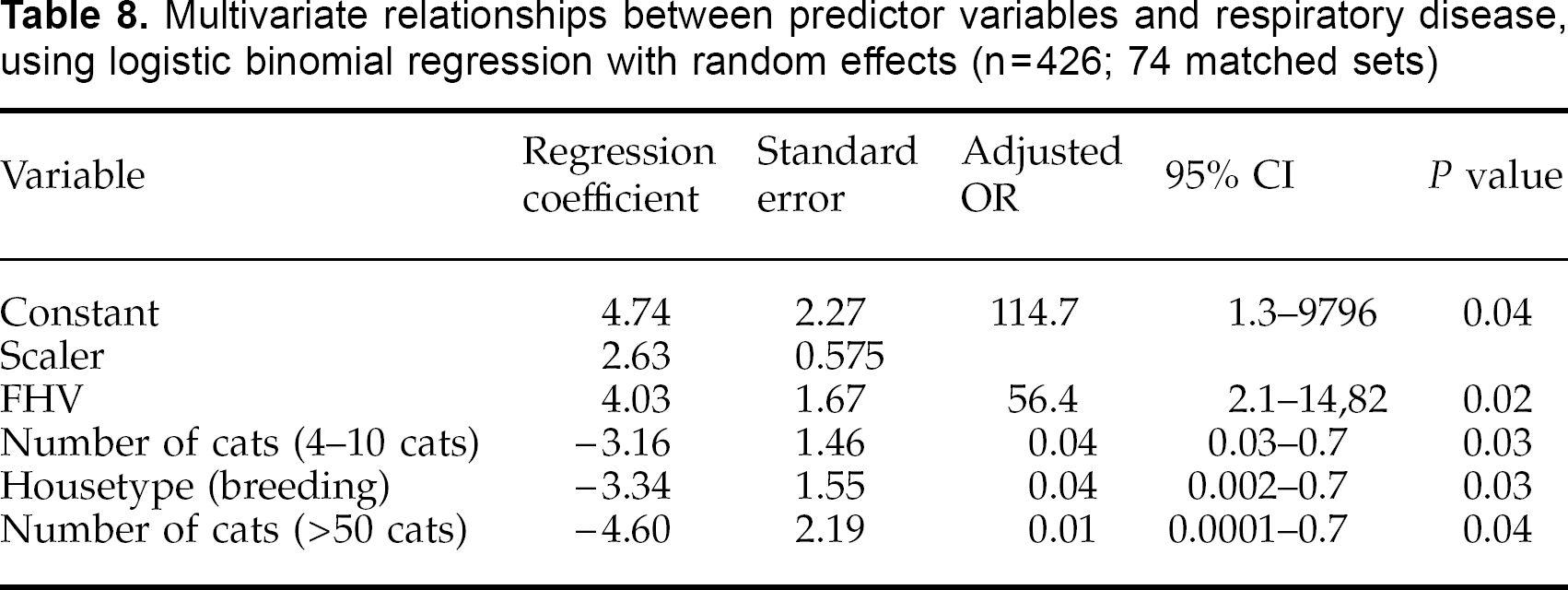
Logistic binomial regression with a random effect for household. Terms remaining significant were FHV isolation (positive) and breeding colonies (negative) (Table 8). The number of cats in the household remained significant, but in this case households of 4–10 cats and >50 cats had significant negative associations with respiratory tract disease.
Multivariate relationships between predictor variables and respiratory disease, using logistic binomial regression with random effects (n=426; 74 matched sets)
FCV isolation
Logistic regression. After adjusting for confounding, dogs and cats with respiratory disease, and the presence of dogs in the household, all showed a positive association with FCV infection (Table 9).
Multivariate relationships between predictor variables and FCV isolation, using ordinary logistic regression (n=426)

Logistic binomial regression with random effects for household. Presence of dogs with respiratory tract disease remained significantly associated with FCV isolation.
FHV isolation
The small number of FHV-positive cats led to difficulties in carrying out multivariable analysis for this outcome variable. It was possible to build a limited model, however, using a subset of predictor variables. Respiratory tract disease had a strongly positive association with FHV isolation and vaccination was negatively associated (Table 10). The only other significant factor was the presence of more than 50 cats in the household.
Multivariate relationships between predictor variables and FHV isolation, using ordinary logistic regression (n=426)

Discussion
Thirty-eight percent of the 740 cats in this survey had upper respiratory tract disease at the time of sampling. Clinical signs in affected cats were similar to those previously reported including sneezing (the most common clinical sign), ocular and nasal discharge, conjunctivitis, dyspnoea and coughing (Norsworthy 1993, Gaskell & Dawson 1994). Other signs including fever, in-appetance and oral ulceration occurred less frequently. The nature and severity of clinical signs was generally consistent with previous studies of both natural and experimental infection for both FCV and FHV (Gaskell & Dawson 1994). However, other pathogens may also have been involved. Cats shedding FHV showed a generally more severe clinical picture than those with FCV, as reported previously. Surprisingly, there was no association of FCV isolation with oral ulceration although this is generally considered a characteristic feature of FCV infection.
Coughing was recorded in 27% of the cats with URTD and was found to be significantly associated with FHV infection. Although coughing is known to occur in some cases of FHV infection (Gaskell & Dawson 1994), and it has recently also been reported in association with
Overall, FCV and FHV were isolated from 26% and 5%, respectively, of the 622 cats sampled for respiratory viruses. In the 378 healthy cats in the survey, the prevalence was 21% and 1% for FCV and FHV, respectively. These figures are similar to those found in other surveys of healthy cats and have remained at a comparable level despite the introduction of vaccination in the mid seventies. In a prevaccination survey of 1500 healthy cats, 8–41% were shedding FCV and 0.4–1.75% were shedding FHV depending on the type of household (Wardley et al 1974). Post-vaccination, a 9-year (1980–1989) retrospective survey of asymptomatic cats found 18.5% shedding FCV and 0.2% shedding FHV (Harbour et al 1991). A more recent survey isolated FCV from 25% and FHV from 0.58% of 500 healthy cats at cat shows (Coutts et al 1994).
The generally higher isolation rate of FCV compared to FHV in clinically healthy cats probably relates to the differences in the carrier states for the two viruses (Wardley 1976, Gaskell & Povey 1973, Gaskell & Dawson 1994). Feline calicivirus carriers shed virus more or less continuously from the oropharynx, whereas FHV carriers only shed intermittently, usually following stress, and most of the time the virus is latent in the trigeminal ganglia and therefore not detected on routine tests (Gaskell et al 1985). For this reason, surveys of healthy cats will tend to underestimate the prevalence of FHV in the population. It is also possible that false negatives for virus shedding may have occurred, particularly when cats were sampled late in the course of disease. In addition, the relatively delayed cytopathic effect of FHV may be masked by that of FCV when both viruses are present concurrently in cell culture. Polymerase chain reaction technology may be used to increase the sensitivity of detection of FHV (Sykes 1997, Weigler et al 1997), although the epidemiological significance of PCR positive virus isolation negative cats is not clear.
In this study the isolation rates from cats with current RTD were 33.2% for FCV and 11.1% for FHV. Although it is difficult to compare between studies, early surveys generally showed approximately equal frequencies of isolation of FCV and FHV from cats with RTD (Povey & Johnson 1971, Jensen et al 1977, MacLachlan & Burgess 1979, Bech-Nielsen et al 1980). More recent surveys have reported results similar to those found in the present survey where FCV tends to predominate (Knowles et al 1989, Harbour et al 1991). It is possible that vaccination has had more effect in reducing the prevalence of FHV-related disease than that caused by FCV, perhaps due to the strain variation amongst FCV isolates and the possibility that vaccine resistant strains may be evolving (Knowles et al 1989, Dawson et al 1993, Lauritzen 1997, Geissler et al 1997).
More than half of the cats with RTD were not shedding detectable levels of FHV or FCV. This may have been partly due to misclassification of disease in some cats, but may also have been due to sampling late in the course of disease, to low sensitivity of detection, or to the presence of other agents for which screening was not carried out. A separate analysis of the cats in this study found a prevalence of 13.8% for
An attempt was made to evaluate risk factors for feline RTD, FCV isolation, and FHV isolation using objective epidemiological techniques. Feline herpesvirus and FCV isolation and cats of 4–11 months old were positively associated with respiratory tract disease and breeding catteries and ‘other’ types of household were negatively associated in comparison with rescue catteries. The effect of household size was less clear, although multiple households in both models were associated with RTD. It is generally accepted that RTD tends to occur in young kittens as they lose their maternally-derived antibody and it has also been reported that respiratory disease is more common in intensively-reared and housed cats (Povey 1990). This study therefore supports the observation that age, intensive housing, stress and the mixing of cats from different sources may all predispose to respiratory disease (Pedersen 1988, Norsworthy 1993).
Few factors were found to be associated with FCV infection on univariable analysis. These included current RTD, recent antibiotic therapy and the presence of dogs in the household, which all had a positive association. Vaccination was shown not to have a significant effect on the isolation rate of FCV: 26% of vaccinated cats were shedding FCV compared to 30% of unvaccinated cats. A previous report also found that a high proportion (43%) of cats shedding FCV were vaccinated (Harbour et al 1991). Similarly in our study an even greater proportion of cats shedding FCV were vaccinated (61%; data not shown). Since 41% of the vaccinated FCV-infected cats in the current survey were also categorised as having current respiratory tract disease, they may represent vaccine reactions or breakdowns (Dawson et al 1993).
Multivariable analysis indicated that feline RTD was a significant predictor variable for FCV isolation as were the presence of dogs in the household and RTD in in-contact dogs. This apparent association of both diseased and healthy dogs with FCV infection has not previously been reported. Viruses antigenically related to feline calicivirus have been isolated sporadically from dogs (Evermann et al 1983, 1985); however, most cases of infection with canine caliciviruses have been associated with diarrhoea (Evermann et al 1985, Mochikuzi et al 1993), or genital disease (Crandell et al 1988); one dog infected with calicivirus had ulcerative glossitis (Evermann et al 1981). The possibility of transmission of caliciviruses between cats and dogs requires further study, however, some studies have shown some serological relationships, and recent work has shown that one canine isolate appears to be in a different genetic clade to FCV (Roerink et al 1999).
The univariable analysis of predictor variables for FHV isolation showed many potential risk factors including younger cats, entire males and current RTD. The survey carried out by Harbour et al also showed a significantly higher shedding rate for FHV in younger cats (Harbour et al 1991). Although the logistic regression analysis for the outcome of FHV isolation could include only limited numbers of covariates, RTD (positive association), larger households (positive association) and vaccination (negative association) were significantly associated with FHV. A positive association between FHV isolation and acute RTD, and cats that had had recent contact with cats outside the household was recently shown in a study by Sykes (1997). In the present work, there was a significant negative association of vaccination on the prevalence of FHV with 3% of vaccinated cats shedding virus in contrast to 16% of unvaccinated cats. Although vaccination appears to have a protective effect, 42% of the cats shedding FHV were fully vaccinated, which supports the findings of Harbour and colleagues where 62% of cats found to be shedding FHV were fully vaccinated (Harbour et al 1991). Both FCV and FHV vaccination protects against disease but not against infection or the development of the carrier state (Orr et al 1978, Gaskell et al 1982, Gaskell & Dawson 1998).
As this survey consisted of convenience based sampling there may have been bias, and many of the cats tested came from households with an ongoing or recent respiratory disease problem. Difficulty in obtaining random samples have been described in other epidemiological surveys of cat populations, and a review of survey reports showed that convenience samples were unlikely to be representative of the feline population (Sukura et al 1992). This, therefore, may restrict the generalisability of the study results.
This study demonstrates that, despite vaccination, respiratory pathogens in cats are still widespread. It therefore reinforces previous recommendations for disease control which have relied on a combination of both vaccination and management procedures (Pedersen 1988, Gaskell & Dawson 1994). It is hoped that the findings of this study may be helpful in further investigation and in controlling risk factors for respiratory disease in cats.
Footnotes
Acknowledgements
The authors would like to thank BSAVA Petsavers for funding this work. Additional support was from the Wellcome Trust and Pet Plan Charitable Trust. The authors would also like to thank Christine McCracken and Ruth Ryvar for technical assistance.