
Abstract
A growing body of literature indicates an association between antiepileptic drugs (AEDs) and bone disease, including histologic, radiographic, and biochemical evidence. The AEDs most commonly reported to cause decreased bone mineral density and disorders of bone metabolism are inducers of the cytochrome P450 enzyme system (phenobarbital, phenytoin, carbamazepine, primidone). More recent studies also suggest that valproate, an enzyme inhibitor, causes abnormalities in bone health. Multiple mechanisms have been postulated to support the association; however, no single mechanism explains all the findings. Identifying bone disease in persons with epilepsy receiving AEDs is important, as multiple treatment options are available.
Introduction
Background and Evidence
Numerous techniques have been used to detect histologic and radiographic evidence of bone abnormalities in patients receiving AEDs, ranging from bone biopsies to the present gold standard in detection of decreased BMD, dual energy X-ray absorptiometry (DXA). Bone biopsies conducted in persons taking AEDs show osteomalacia, which literally means softening of bone, histologically characterized by an increase in osteoid or unmineralized bone (1). DXA assesses predominantly trabecular bone, such as the spine and the ribs, and measures the total mineral content. It is the most sensitive technique available for assessing BMD, detecting a 5% decrement or less of bone mass (18). Several studies have measured BMD in adult patients receiving AEDs by using DXA, finding significantly reduced BMD at the ribs and spine (7,11), femoral neck (6,11,12), and total hip (11). A prospective study quantified ongoing bone loss in young men receiving AEDs, with the highest rate of bone loss in the young male skeleton (12). In children, reduced BMD also is associated with AEDs, with reports describing reduced axial, appendicular (6,13), and whole-body bone mass (19).
Multiple biochemical abnormalities of bone metabolism are present in patients taking AEDs (see Table 1). These abnormalities include hypocalcemia, hypophosphatemia, reduced serum levels of biologically active vitamin D metabolites, and hyperparathyroidism. In addition, elevated levels of markers of bone turnover are found, such as markers of bone formation and bone resorption.
Biochemical Abnormalities of Bone Metabolism Associated with AEDs
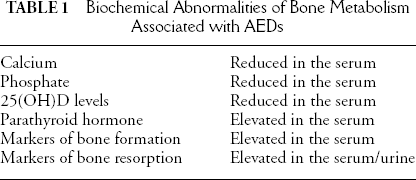
Calcium homeostasis and the concentration of phosphate in the body are essential components of bone metabolism, and both are affected by AEDs. Hypocalcemia has a reported incidence varying between 3% and 30% (2,20–23). Reduced serum phosphate also has been described in patients prescribed AEDs (4,24,25).
Vitamin D is essential for the proper development and maintenance of bone. Serum 25(OH)D concentration is the most commonly used index of vitamin D status, and reduced levels are seen in both adults and children taking AEDs (4, 11, 20, 23, 26–31). The most active metabolite of vitamin D is 1,25[OH]2D and, in adults taking AEDs, has been found to be decreased (10).
Parathyroid hormone (PTH) is secreted by the parathyroid gland and is directly involved in the regulation of calcium. When serum calcium is decreased, PTH acts to increase bone breakdown or resorption. An increase in circulating PTH associated with AED therapy is reported (21, 32).
Markers of bone formation have been assessed in patients receiving AEDs, which include alkaline phosphatase, osteocalcin, and the C-terminal extension peptide of type I procollagen. Alkaline phosphatase is the most commonly used marker of bone formation, and increases have been seen in both children and adults receiving AEDs (9,23–25). Because serum total alkaline phosphatase is derived from bone, liver, and other sources, it lacks sensitivity and specificity in evaluating bone disease. In reports that measured the isoenzymes, the increase in total alkaline phosphatase was owing mainly to the bone fraction (26,27). Osteocalcin, or bone-gla protein, is a small noncollagenous protein that is specific for bone tissue and dentin and is synthesized predominantly by osteoblasts. High serum levels of osteocalcin with AED treatment are described (9,33,34,). Procollagen type I molecules are secreted by osteoblastic cells. Subsequent cleavage of the amino terminal and carboxy terminal creates extension peptides. The C-terminal extension peptide of type I procollagen (PICP) is a putative serum marker of bone formation, and significant elevations have been seen in patients taking AEDs (9,34).
In certain bone diseases such as osteoporosis, bone resorption exceeds formation. Specific markers of bone resorption can be measured in the urine and serum. Cross-linked carboxy-terminal telopeptide of human type I collagen is a serum marker of bone degradation, and hydroxyproline is a marker in the urine. These markers are elevated in patients with epilepsy receiving long-term AEDs (9) and after recent initiation of therapy (34).
Antiepileptic Drugs Associated with Bone Disease
The AEDs most commonly associated with altered bone metabolism and decreased bone density are inducers of the cytochrome P450 enzyme system, including phenytoin (PHT), carbamazepine (CBZ), primidone (PRM), and phenobarbital (PB) (6,7,9,23,24,34). The majority of the published studies and evidence is from patients receiving these medications.
The effect of valproate (VPA) on bone metabolism and bone density has received limited study. Early reports evaluating indices of bone metabolism in patients taking VPA found no significant abnormalities (23,29). In contrast, a recent study of 40 adults taking long-term VPA found increased serum concentrations of calcium, low serum 1,25[OH]2D concentration, and increased markers of bone resorption and formation (10). The increased serum calcium was postulated to reflect increased bone resorption. A few small pediatric studies evaluated bone mass in patients taking VPA, finding reduced bone mineral density (35) and normal bone mineral density (6,36). In adults, one study (10) using computer-linked DXA measured BMD at the second metacarpal of the right hand in subjects taking VPA monotherapy. A BMD reduction of 14% in adults taking VPA monotherapy was found, compared with healthy control subjects.
In the past 10 years, multiple new AEDs have been approved. Few studies have evaluated the effect of these medications on bone mineral metabolism and BMD. One study (5) in adults looked at the effect of some of the new drugs [lamotrigine (LTG), topiramate, vigabatrin, gabapentin) on bone mineral metabolism and BMD, and found no significant abnormalities. In children, short stature, low bone mass, and reduced bone formation was described in boys and girls treated with LTG either alone or in combination with VPA (19). As no reference standards exist for BMD in children, the reported findings have no clear clinical significance.
Polytherapy has been shown to be associated with a higher risk of bone metabolism abnormalities than is monotherapy (11,21,37). Polypharmacy also has been identified as a risk factor for low bone mass in adult patients (11). No single combination has emerged as more likely to cause bone disease.
Possible Mechanisms of Antiepileptic Drug–associated Bone Disease
Several theories have been proposed to explain the link between AEDs and bone disease. Hepatic induction of the cytochrome P450 enzyme system leading to increased catabolism of vitamin D is the principal mechanism reported (9,38). However, it does not explain the findings described in patients receiving other medications, such as VPA, an inhibitor of the cytochrome P450 enzyme system. In addition, the finding of vitamin D deficiency has not been demonstrated in all studies, and evidence of bone turnover is found independent of vitamin D deficiency (9,32,34). Other possible mechanisms include a direct effect on bone cells, including impaired absorption of calcium and inhibition of response to PTH, hyperparathyroidism, and calcitonin deficiency (38).
AEDs that induce hepatic cytochrome P450 enzymes may cause increased conversion of vitamin D to polar inactive metabolites in the liver microsomes, reducing bioavailable vitamin D (23,39). Decreased biologically active vitamin D leads to decreased absorption of calcium in the gut, resulting in hypocalcemia and an increase in circulating PTH. PTH then increases the mobilization of bone calcium stores and subsequent bone turnover.
AEDs may interfere with intestinal absorption of calcium. Impaired absorption would lead to hypocalcemia and feedback hypersecretion of PTH. Markedly decreased calcium absorption was found in rats treated with PHT but not with PB (40). These results suggest that in patients treated with PHT, impaired calcium absorption may play a role.
Evidence also exists for inhibition of the cellular response to PTH. Fetal rats treated with PHT or PB demonstrated an impaired response to PTH (41). Inhibition of the bone resorptive response to PTH could lead to hypocalcemia, a frequent finding in patients taking AEDs.
Hyperparathyroidism also has been suggested as a possible mechanism. Both male patients with normal vitamin D status (9) and subjects who were vitamin D repleted had evidence of hyperparathyroidism (32). Hyperparathyroidism can primarily activate bone resorption and, through a coupling phenomenon, secondarily activate bone formation.
A final postulated mechanism is calcitonin deficiency. Calcitonin is a hormone produced by the thyroid gland that inhibits osteoclast-mediated bone resorption. Calcitonin deficiency may therefore accelerate bone turnover. This deficiency has been demonstrated both in vitro and in vivo (42,43).
Treatment
Although few studies have evaluated the effect of treatment in bone disease associated with AEDs, multiple therapies for bone disease are available, including calcium and vitamin D supplementation, bisphosphonates, hormone replacement, selective estrogen modulators (SERMs), and calcitonin.
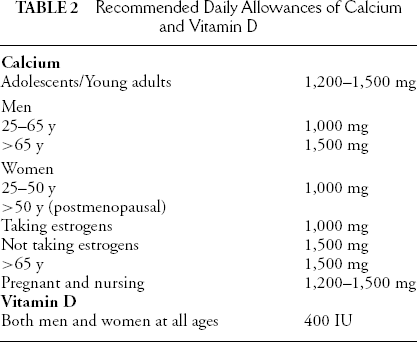
Calcium can slow the rate of bone loss in elderly women not taking AEDs with inadequate calcium intake (44). This is an important finding, as most people do not have adequate calcium intake in their diets, and supplementation is necessary. Vitamin D supplementation also may be necessary, especially for persons with inadequate exposure to sunlight (see Table 2 for recommended daily allowances of calcium and vitamin D). Vitamin D supplementation was evaluated in one study of (45) institutionalized and noninstitutionalized subjects receiving AEDs who had low 25-hydroxyvitamin D levels. Seventeen of the 18 noninstitutionalized patients achieved normal 25-hydroxyvitamin D levels over a period of 12 months; one patient had normal levels after 15 months. All institutionalized patients achieved normal levels over a period of 12 months. The doses of vitamin D required ranged from 400 to 4,000 IU/day.
Recommended Daily Allowances of Calcium and Vitamin D
The two approved formulations of bisphosphonates including alendronate and risedronate. Bisphosphonates are potent inhibitors of bone resorption and, given the findings of increased bone resorption associated with AEDs, may be an effective treatment for bone disease in patients receiving AEDs.
Data supports the efficacy of hormone replacement in stop-ping bone loss (44). However, multiple reported side effects include an increase risk of breast cancer, cardiovascular events, and venous thrombolism (46). In addition, women with epilepsy should be aware that hormone-replacement therapy (HRT) may increase seizure activity (47).
SERMs act as either estrogen agonists or antagonists (44). Raloxifene is a Food and Drug Administration (FDA)-approved formulation, and in bone, acts as a partial agonist. In postmenopausal women, raloxifene increases bone mass and reduces the risk of vertebral fracture by 40% to 50% (48,49). Side effects include an increased risk of deep venous thrombosis and an increase in hot flashes.
As studies have found decreased calcitonin associated with AED use, calcitonin may be an effective treatment in patients with bone disease receiving AEDs. In a study of postmenopausal women not on AEDs intranasal salmon calcitonin at a dose of 200 IU per day reduced the rate of vertebral but not peripheral fracture (50).
Conclusion
AEDs are associated with bone disease, as evidenced by biochemical abnormalities and decreased BMD. The AEDs most commonly reported to affect bone include inducers of the cytochrome P450 enzyme system (PHT, PB, PRM, CBZ). In addition, growing evidence suggests that VPA, an enzyme inhibitor, also affects bone. Limited data exist regarding the newer AEDs. Several theories have been proposed to explain the mechanism of AED-associated bone disease, but no single theory explains all the reported findings, and the mechanisms may be multiple. Finally, no definitive guidelines have been established for evaluation or treatment. However, persons taking long-term AEDs should have routine examination of BMD by using DXA, particularly if prescribed an enzyme-inducing AED, and although few studies have evaluated treatment in AED-associated bone disease, multiple therapies are available, including calcium and vitamin D supplementation, bisphosphonates, hormone replacement, SERMs, and calcitonin.