
Abstract
Several studies have explored a possible association between migraine and hyper- tension, with contradictory results. Because of this uncertainty the relation between blood pressure (BP) and migraine was studied in 10 366 men and 11 171 women in a population-based longitudinal study. A modified version of the 1988 International Headache Society criteria was used for diagnosis of migraine. Logistic regression analysis was used. The crude 1-year prevalence of migraine was 5.2% among men and 14.1% among women. No significant association was found between hypertension and migraine. For a one standard deviation (SD) increase in diastolic BP the probability of having migraine increased 14% (P = 0.11) for men and 30% (P < 0.0001) for women. For a 1-SD increase in systolic BP the probability of having migraine decreased 19% (P = 0.007) for men and 25% (P < 0.0001) for women. It was also found that for a 1-SD increase in pulse pressure the probability of having migraine decreased 13% (P = 0.005) for men and 14% (P < 0.0001) for women. In a population-based study of men and women it was found that subjects with migraine had lower pulse pressure, lower systolic BP and higher diastolic BP compared with controls.
Introduction
Several studies have explored a possible association between migraine and hypertension, with contradictory results. Some studies have shown a positive association between migraine and hypertension (1–5), others have shown no difference in prevalence of migraine between hypertensive and non-hypertensive subjects (6–8). Two recent studies found a significant negative association between migraine and hypertension (9, 10).
When looking at association between migraine and blood pressure the results have also been contradictory. Case–control studies have shown a positive association between migraine and systolic blood pressure (SBP) (11) and both SBP and diastolic blood pressure (DBP) (12).
In a cross-sectional epidemiological study the relation between DBP and SBP, respectively, and migraine was examined. No significant difference in SBP was found, but women migraineurs had higher DBP than non-migraineurs. This difference was not found for men (8). It has also been found that migraine was more frequent in individuals with normal blood pressure compared with high blood pressure (9). A recent population-based longitudinal study showed that participants with migraine had lower SBP and lower mean arterial pressure, and significant trend of decreasing frequency of migraine with increasing SBP (10). Other epidemiological studies have not shown a clear association between blood pressure and migraine (6, 13).
Possible reasons for some of these contradictory results may be differences in definition of migraine and hypertension, differences in blood pressure measurement procedures and differences in sample size. The methods for comparison in these studies vary also, some comparing migraine with SBP or DPB alone and others with SBP and DBP combined.
Because of the uncertainty of the association between migraine and hypertension, and migraine and blood pressure this possible association was studied, using data from The Reykjavik Study. The study provides an opportunity to re-examine the association between migraine and hypertension and migraine and blood pressure in a large population-based study, thus allowing stratification by sex, focusing on systolic, diastolic, mean arterial and pulse pressure.
Methods
The study was performed in accordance with the Helsinki Declaration and was approved by the National Bioethics Committee and the Data Protection Authority in Iceland. All participants gave informed consent.
People invited to participate in the Reykjavik Study were all the legal residents in the Reykjavik area on 1 December 1966. The men were born in the following years: 1907, 1910, 1912, 1914, 1916, 1917, 1918, 1919, 1920, 1921, 1922, 1924, 1926, 1928, 1931 and 1934; the women 1 year later, i.e. 1908, 1911, etc. Both sexes were divided into groups A, B and C according to birthday, i.e. those in group B were born on the 1st, 4th, 7th, etc., of each month, those in group C were born on the 2nd, 5th, 8th, etc., of each month, and those in group A were born on the 3rd, 6th, 9th, etc., of each month (see Fig. 1). Groups D, E and F comprised people born in the years previously omitted in the period 1907–1935, excluding those years listed above and divided in the same manner as A, B and C. The study population thus comprised all men born in the years 1907–1934 and all women born in the years 1908–1935 living in the Reykjavik area on 1 December 1966. The study was performed in six stages. The first took place in 1967–1969, the second in 1970–1972, the third in 1974–1979, the fourth in 1979–1984, the fifth in 1985–1991 and the sixth in 1991–1996. Group B was invited to participate in the first five stages of the study, group C in stages 2 and 3, group A in stage 3, group D in stage 4, group E in stage 5, and those in group B and who had reached the age 70 in 1991 (men) or 1993 (women) participated in stage 6. One of the original aims of the Reykjavik Study was to assess the health benefits to be gained from such mass screening programmes. Therefore one group (B) was invited to be examined repeatedly. Figure 1 shows the years for examination for each group. The number of subjects alive at midpoint of each stage was used to calculate response rate. In the six stages 9328 men were invited 26 071 times to be examined, which resulted in 18 494 examinations, an average response rate of 70.9% (range 64.6–75.25%). Ten thousand and sixty-two women were invited 26 080 times, which resulted in 18 281 examinations, an average response rate of 70.1% (range 66.8–76.9%) (14, 15). In this study only the first examination for each subject was used.

Study plan of the Reykjavik Study. The selected population were all men (M, n = 14 923) with legal residence in Reykjavik and the surrounding area on 1 December 1966, who were born 1907–1934. The women (W, n = 15 872), selected from the same area, were born 1908–1935. The men and women were divided into groups labelled A–F. The numbers shown represent the number in each group. The hatched and shaded boxes show when subjects in each group were examined.
In order to look at subjects younger than in the Reykjavik Study, a new sample was selected in 1972, the Reykjavik Study for the young. It comprised equal groups of men and women, 2781 in all, born 1940–1954 (a stratified sample of subjects born in 1940, 1944, 1945, 1949, 1950, 1954). The subjects were invited to be examined in the years 1973–1974 and again in 1983–1985. Only the first examination was used. The number of subjects that were examined at least once was 1038 men and 1109 women. Combining the subjects from the Reykjavik Study and the study for the young, the total number of men was 10 366 and of women 11 171, and their ages were 19–87 years.
Every participant received an invitation letter that included standardized questions about health and social factors.
Examinations
Participants came in a fasting state to the clinic. After a 5-min rest, the supine blood pressure was measured, on two occasions, between 08.30 and 10.30 h, by a nurse, and 10–14 days later between 11.00 and 13.30 h, by a physician. Subjects were not instructed to be fasting at the second blood pressure measurement. The instruments used were mercury sphyngomanometers of the type ‘Erkameter’ wall-model (Erka, Germany). The cuffs had a rubber bladder 15 × 32 cm, and the total length of the cuff was 66 cm. The same types of cuffs and instruments were used throughout the study. The procedure followed in measuring blood pressure was according to World Health Organization recommendations (16). The diagnosis of hypertension was based on the mean of two measurements: SBP ≥ 160 mmHg and/or DBP ≥ 95 mmHg. Subjects on antihypertensive medication were considered hypertensive.
Definition of migraine
In this study a modified version of the 1988 International Headache Society (IHS) criteria was used (17). The questions on headache in the study questionnaire have been the same throughout the study. The questions are as follows.
Questions concerning symptoms during the last 12 months:
Is the pain usually in one side of the head?
Do you feel nauseated or vomit when you get the headache?
Do you get visual disturbances simultaneously or shortly before the pain starts?
Do you get photophobia during the headache attack?
Do you get numbness in one side of the face or numbness in either arm before the headache begins?
Subjects were considered to have migraine ‘loose criteria’ if answering yes to any two or more of questions 1–5.
A ‘stricter criterion’ was also made where a subject had to answer yes to any three or more of questions 1–5.
The questionnaire of the present study was composed in 1967 and has to be compared with the more modern 1988 IHS criteria (17). The main differences are that in the present questionnaire questions are missing about duration, intensity, phonophobia and pulsating quality of the headache. Also missing are questions about the less common symptoms of unilateral weakness and speech difficulty.
Statistics
Information on subjects at first visit was used in a logistic regression model. All regression analyses were performed separately for men and women. When calculating odds ratios (ORs), adjustments were made for age and year entering the study. Age was entered into the model as a continuous variable and as a categorical variable (12 categories and six categories). Comparing the Deviance (− 2 log likelihood) of the two models, using a χ2 test, age in 12 categories of 5 years each gave the best fit. DBP and SBP were introduced separately and jointly to the model. The model containing both SBP and DBP gave the best fit and was therefore used to estimate the effect of SBP and DBP on odds of having migraine. Pulse pressure (PP) was defined as SBP − DBP and mean arterial pressure as (1/3 SBP + 2/3 DBP).
To see if educational level was a confounder, four educational levels were identified in the questionnaire: elementary school or less, high school education, junior college education and university education, and used in the logistic regression model. Also to see if smoking was a confounder, smoking was entered into the logistic regression model as: never smoked, former and current smoker.
Collinearity (to see if there was a relationship among the predictor variables that did not involve the response variable) between SBP and DBP was analysed by calculating condition numbers from variance–covariance matrix of the predictor variables and the variance component of each predictor variable. Significance testing was two-sided and based on a 5% probability level. Thus, results are presented with 95% confidence intervals (CI). The software package used was SPIDA (18).
Results
Prevalence of migraine
The crude 1-year prevalence of migraine among men using loose and strict criteria of migraine was 5.2% and 2.1% and for women the prevalence was 14.1% and 8.0%, respectively. The corresponding 1-year prevalence of migraine for men, adjusted to Segi World population (19, 20) using loose and strict criteria, was 5.7% and 2.3% and for women the prevalence was 16.4% and 8.0%, respectively. The age- and sex-specific 1-year prevalence of migraine using loose and strict criteria of migraine in the Reykjavik study can be seen in Fig. 2. The subject's characteristics at first visit can be seen in Table 1. There are some differences in BP levels between groups but these differences are not adjusted for age, examination year and antihypertensive medication use.

Age- and sex-specific 1-year prevalence of migraine in the Reykjavik Study, 1967–1996. Prevalence of migraine, defined by a modified version of the 1988 International Headache Society criteria, in a cohort of 10 366 men and 11 171 women. Loose criteria of migraine: answering yes to two or more out of five questions on migraine, men (▪, n = 543) and women (•, n = 1573). Strict criteria of migraine: answering yes to three or more out of five questions on migraine, men (Δ, n = 214) and women (○, n = 826).
Characteristics at first examination of men (n = 10 366) and women (n = 11 171) in the Reykjavik Study 1967–1996
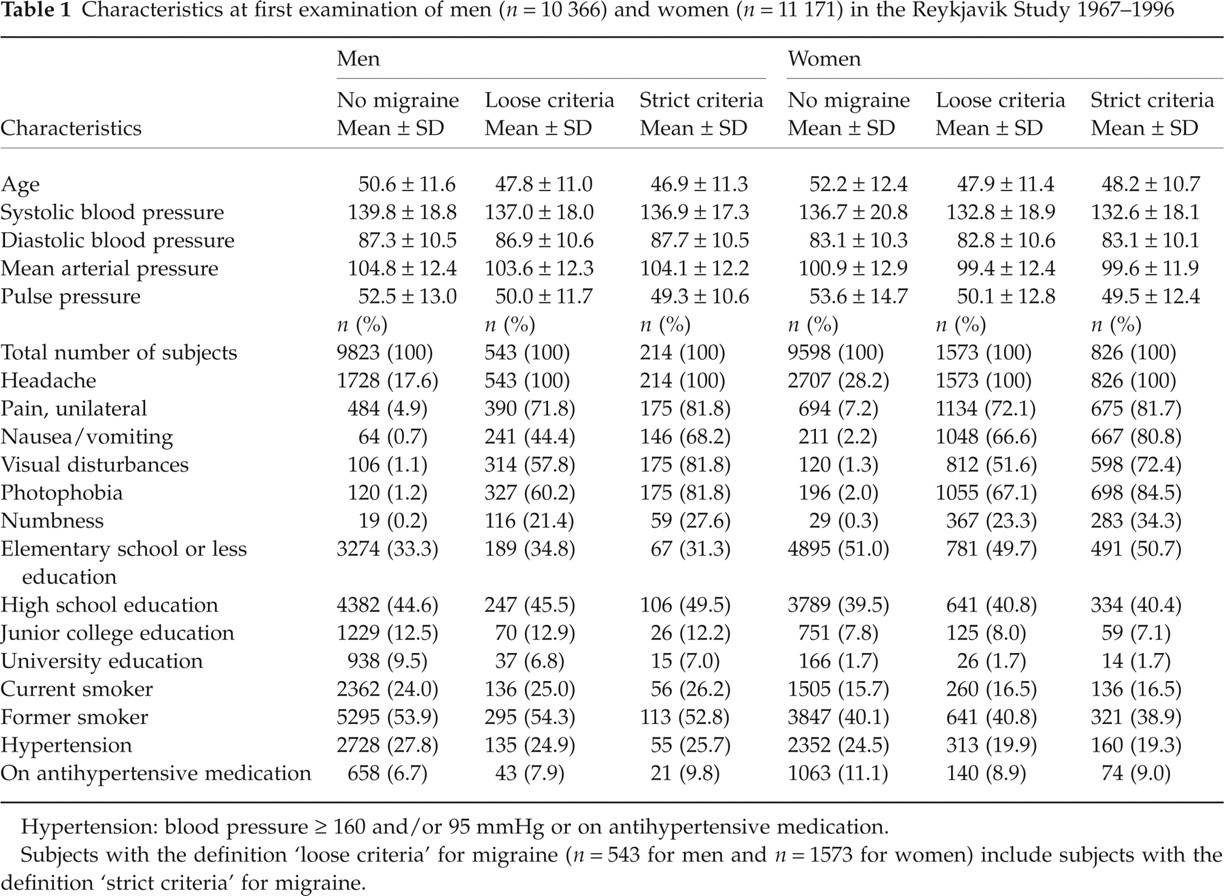
Hypertension: blood pressure ≥ 160 and/or 95 mmHg or on antihypertensive medication.
Subjects with the definition ‘loose criteria’ for migraine (n = 543 for men and n = 1573 for women) include subjects with the definition ‘strict criteria’ for migraine.
Migraine and hypertension
Using loose criteria, hypertension was not associated with migraine, OR 0.97 (95% CI 0.79, 1.19) for men and 1.03 (95% CI 0.89, 1.18) for women. When excluding those on antihypertensive medication, the ORs were lower but not significantly lower than one, OR 0.83 (95% CI 0.66, 1.06) and 0.93 (95% CI 0.78, 1.12), respectively.
When dichotomizing on SBP ≥ 160 mmHg, using loose criteria of migraine (adjusting for age and antihypertensive medication use), there was no association with migraine for men, OR 0.93 (95% CI 0.71, 1.22). However, for women there was a significant inverse association, OR 0.76 (95% CI 0.62, 0.92).
When dichotomizing on DBP ≥ 95 mmHg (adjusting for age and antihypertensive medication use), there was no association with migraine for men or for women, OR 0.89 (95% CI 0.71, 1.12) for men and 1.02 (95% CI 0.86, 1.21) for women.
Migraine and blood pressure
In Fig. 3 the association between blood pressure and migraine, using loose and strict criteria of migraine, can be seen. Due to lower sample size in the groups defined by the stricter criteria, the CIs for the odds ratios were wider than for the odds ratios in the groups defined by the loose criteria. SBP was significantly negatively associated with migraine but DBP was not. There was no significant association between migraine and mean arterial pressure. However, there was a significant negative association between pulse pressure and migraine for both men and women. When looking at the association between SBP and migraine for men and women, adjusting for DBP (see Fig. 3), an increase in SBP was associated with decreased prevalence of migraine. On the other hand, when looking at an association between DBP and migraine for men and women, adjusting for SBP (see Fig. 3), an increase in DBP was associated with increased migraine prevalence. When SBP and DBP were both in the logistic regression model there was a consistency between using loose and strict criteria of migraine both for men and women. There was a stronger association between blood pressure and migraine amongst subjects defined by strict criteria of migraine than amongst those defined by loose criteria (Fig. 3). Comparing the deviance of the regression models for men and women between blood pressure and migraine, the models giving the best fit were those containing both SBP and DBP and the model containing pulse pressure only, but the model with mean arterial pressure gave the highest deviance (data not shown).

Adjusted odds ratio (95% confidence interval) of having migraine for a 1-SD increase in blood pressure variable. Systolic (SBP) and diastolic (DBP) blood pressure are entered individually and jointly into the regression model. Loose criteria of migraine: answering yes to two or more out of five questions on migraine, men (n = 500) and women (n = 1433). Strict criteria of migraine: answering yes to three or more out of five questions on migraine, men (n = 193) and women (n = 752). Adjustment is made for age and year of examination. Subjects on antihypertensive medication are excluded. PP, Pulse pressure; MAP, mean arterial pressure.
Possible confounders
The introduction of educational level into the model did not change the association between pulse pressure and migraine significantly and was therefore left out of the model (P for difference in β coefficients, P = 0.99 for men and P = 0.93 for women, t-test).
Relative to those who had never smoked, current smoking was not a significantly predictive variable in the model for migraine in relation to age, pulse pressure and antihypertensive medication for men (P = 0.91; OR 1.01, 95% CI 0.81, 1.27) or for women (P = 0.96; OR 0.96, 95% CI 0.85, 1.08). In the same model, former smoking was not significantly predictive of migraine for men (P = 0.20; OR 1.18, 95% CI 0.91, 1.54) or for women (P = 0.13; OR 1.13, 95% CI 0.97, 1.32). Smoking was therefore left out of the model.
The variables that were used for each sex in the final regression model were age and year of examination. Mean arterial blood pressure, pulse pressure, SBP and/or DBP were all analysed in relation to migraine adjusting for these variables.
A possible collinearity between SBP and DBP was considered. When checking for collinearity in a logistic regression model it is advisable to check condition numbers that are over 20 and to check the variance component for these values. It should be analysed further when the variance component exceeds 0.5 for more than one variable where the condition numbers are over 20. The condition numbers where SBP and DBP had variance component 0.8–0.9 was about 40. When SBP and DBP were normalized (i.e. the average was deducted and then divided by the SD), the regression was almost identical and the deviance also. Where SBP and DBP was dominant the condition numbers were only about 4 so there was not much concern for collinearity. Also, the correlation coefficient for SBP and DBP was 0.75 but is usually close to 0.99 when there is considerable collinearity.
Discussion
In a population-based study of men and women there was no clear association between hypertension and migraine. Using logistic regression analysis, it was found that subjects with migraine had lower pulse pressure, lower SBP and higher DBP compared with controls.
Hypertension and migraine
This study showed no clear association between hypertension and migraine. Similar findings have been reported by others (6–8, 21). There was no association between migraine and diastolic hypertension but a negative association with systolic hypertension was found among women but not among men. In 1988 the IHS published a new definition of migraine (17). Most studies on the association between hypertension and migraine were published before that date. Recently, two studies showed a negative association with migraine and hypertension. One found a negative association for both systolic and diastolic hypertension (9), but when adjusting for sex and confounding factors the association was marginally significant. The other found the negative association with migraine to be similar whether SBP ≥ 140/DBP ≥ 90 mmHg or SBP ≥ 160/DBP ≥ 95 mmHg was used as the definition of hypertension (10). Differences in these results may be due to different definitions of migraine (and hypertension) and to differences between populations and environmental factors.
Blood pressure and migraine
There was good consistency in the results between loose and strict criteria of migraine and blood pressure and between men and women (Fig. 3). When SBP or DBP was entered into the model, SBP was significantly negatively associated with migraine and DBP was not associated with migraine. This is in line with one recent study (10). But when entered jointly, DBP became positively associated with migraine and it gave significantly lower deviance, thus indicating it was a better model. When SBP and DBP were entered jointly into the regression model, the effect of increase in SBP could be seen when DBP was kept constant and vice versa. A positive association between DBP and migraine has been described before, but these studies did not report an inverse association between SBP and migraine (8, 13). An inverse association between SBP and migraine has recently been reported (9, 10), and in the first study there was also a inverse association between DBP and migraine (BP was defined as optimal normal, SBP < 130 and DBP < 85 mmHg, vs. high or above) (9), but in the second study the inverse association found between DBP and migraine was not significant (10). SBP being negatively associated and DBP being positively associated with migraine in the present study can possibly explain why many studies show no association between hypertension and migraine (6–8, 13). When an individual has systolic and diastolic hypertension the possible individual effect of SBP and DBP on migraine would cancel each other out. When comparing the deviance of different regression models it could be seen that SBP had a stronger association with migraine than DBP.
Pulse pressure was negatively associated with migraine both for men and women and to our knowledge this is the second study describing such an association. The first study (10) could not stratify by sex and did not adjust for antihypertensive medication use. It seems likely that the main connection between BP and migraine is through inverse association between SBP and migraine, because when adjusting for antihypertensive medication, systolic hypertension was negatively associated with migraine but diastolic hypertension was not. This, together with the results for the regression model that excludes subjects on antihypertensive medication, further supports that SBP has a stronger association with migraine than DBP.
Possible mechanism
The pathophysiological mechanisms behind migraine are poorly understood and while mechanistic explanations of the association between migraine and blood pressure are not available, some possibilities have emerged. There is some evidence for the involvement of calcitonin gene-related peptide (CGRP) in migraine (22). It has been found that the basal CGRP concentration in blood is higher in migraine patients (23), intravenous administration of CGRP can trigger a migraine attack (24) and a CGRP receptor antagonist is effective in the treatment of acute migraine attacks (22). As CGRP is a potent vasodilator (25), it seems possible that its involvement in migraine could explain some of the findings in the present study. Another possible mechanism is the involvement of serotonin (5-HT). Platelet serotonin has been found to be lower in migraineurs than in matched controls (26). Serotonin is mainly a vasoconstrictor which could also explain some of the findings of the present study. Other mechanisms could also be involved.
Strengths and limitations
The present study is large compared with many other studies on migraine. It also involves a relatively large proportion of an entire nation. The large number of subjects in the study and a relatively low number of subjects on antihypertensive treatment (<10%) allow omission of the antihypertensive-treated subjects when looking at the association between BP variables and migraine. The subjects are selected on basis of neither health nor socio-economic status and that gives the results more weight. Prevalence of migraine in this study is based on a modified version of the 1988 IHS criteria. When comparing the modified version used and the IHS criteria there are several questions missing in the modified version for a definite diagnosis according to the 1988 IHS criteria. However, the questions used cover the most common migraine symptoms.
When using loose criteria of migraine the age-standardized 1-year prevalence for men and women of 5.7% and 16.4% is similar to what has been described for western countries, which is about 6% for men and 15–18% for women (27, 28). Preliminary results from a study of 2000 randomly selected Icelanders, using IHS criteria, showed a 7% and 19% prevalence of migraine for men and women, respectively (29). This prevalence is similar to the results in the present study. Age distribution for the 1-year prevalence of migraine is similar to what has been described by others (27, 30). The average 1-year prevalence and age distribution found in the present study gives some assurance that the sample is composed mainly of migraine patients.
This is a cross-sectional study and does not allow any inference of causality. Temporality is one of the factors missing for causality inference in a study of this kind and it is not possible to decide which comes first—the migraine or the changes in blood pressure.
Conclusions
In a population-based study of men and women, no clear association was found between migraine and hypertension. It was found that subjects with migraine had lower pulse pressure, lower SBP and higher DBP compared with controls. The association between blood pressure and migraine was stronger among women than men.
The mechanisms behind the association between migraine and blood pressure may involve CGRP, serotonin and other factors.
Footnotes
Acknowledgements
We thank all the employees of the Icelandic Heart Preventive Clinic (Hjartavernd) for their skilful contribution to the data collection. The study was supported by the Medical Faculty and the Research Fund of the University of Iceland and by the Icelandic Research Council.