
Abstract
Since visual aura is usually described as expanding zigzag lines, neurones involved with the perception of line orientation may initiate this phenomenon. A visual incongruent line stimulation protocol was developed to obtain functional magnetic resonance images (fMRI) interictally in 5 female migraine patients with typical fortification spectra and in 5 normal matched controls. Activation in the visual cortex was present contralateral to the side of stimulation in 4 of 5 patients, notably in the extrastriate visual cortex. In 4 of 5 controls activation was observed in the medial and anterior orbitofrontal cortex. In one of them additional activation at the right nucleus accumbens/ventral striatum and right ventral pallidum was present. In the remaining control subject activation was present in the left primary visual cortex. The enhanced interictal reactivity of the visual cortex in migraineurs supports the hypothesis of abnormal cortical excitability as an important pathophysiological mechanism in migraine aura, though the role of specific regions of the visual cortex remains to be explored.
Introduction
Due to its uniqueness, migraine visual aura remains one of the most intriguing topics in neurology. Usually preceding the headache, this phenomenon may present as a multitude of scintillating bars and corners, starting as a small greyish spot in the visual field. This area expands during the following 20 min, edged by typical bright horseshoe-shaped zigzag lines. Angles in this serration pattern average 60 degrees, varying from 45 degrees near the field centre up to 70 degrees near the periphery (1–4).
The pathophysiology of migraine aura remains partially obscure. The stereotyped visual pattern suggests that a paroxysmal occipital cortex malfunction related to neurones particularly involved with line orientation perception underlies the aura. In 1944, Leão and Morison (5, 6) identified a hitherto unknown cortical phenomenon in exposed rabbit cortex he named spreading depression (SD). Convincing evidence indicates that an SD-like phenomenon occurring at the occipital lobe is the neurophysiological basis of visual aura. SD, which may occur in humans (7, 8), seems to induce a concomitant spreading hypoperfusion already recorded during migraine (9). Blood oxygenation level-dependent (BOLD) signal changes suggestive of SD have been detected in migraine with aura subjects (10, 11). Diffusion-weighted MR imaging has also been successfully used to gauge SD induced experimentally in gyrencephalic feline cortex (12).
In primates, visual cortical cells may be classified according to their responses to orientated moving bar stimuli (13). The population of cells sensitive to specific orientation is functionally arranged in columns and layers. Cortical SD sweeps across the visual cortex as a wave of short excitation followed by neuronal inhibition. The successive activation of visual cortex neurones with distinct line orientation preferences may be intimately related to the genesis of the typical zigzag-like fortification spectra pattern. Moreover, the speed of SD propagation is compatible with the progression rate of the visual aura (4, 14).
Cortical hyperexcitability appears to play a Key role in migraine (15). Transcranial magnetic stimulation of the occipital cortex induces more phosphenes in migraine with aura patients than in controls (16, 17).
It is noteworthy that the visual type of migraine aura is particularly prevalent. Changes in extracellular potassium concentrations are important for SD propagation (18). Since the human primary visual occipital cortex has the lowest glial-neuronal ratio, and glial cells are important to redistribute potassium to areas with relatively lower potassium concentrations, this may explain why SD and consequently visual aura would be more common (19). The increased interictal and constant occipital cortex responsiveness in migraine putatively facilitates the genesis and propagation of SD-like waves in the primary visual cortex. Because a high density of neurones responsive to orientated line patterns is present in the early visual cortex (mainly in areas V1 and V2), these regions may have an important pathophysiological role in the generation of the migraineous aura. Based on the hypothesis that line orientation sensitive-neurones in the visual cortex of migraine patients may be abnormally responsive to certain orientated stimuli, we employed functional MRI and a specific visual stimulation protocol to study interictal brain responses in migraine patients and in control subjects.
Subjects and methods
This study was approved by the local ethical committee and an informed consent was obtained from all patients and controls. Five normal female subjects of mean age 34 years (range 25–51 years) and five female IHS migraine with aura otherwise healthy patients of mean age 36.4 years (range 28–48 years) were studied interictally (Table 1). Participants were not undergoing medical treatment or taking drugs of any sort, including migraine prophylactic agents. Medications were not used prior fMRI examinations by any volunteer. All patients described typical fortification spectra phenomena. Visual aura was reported as right-sided in two individuals, left-sided in one, and alternating in two.
Demographic data

FS, fortification spectra.
Stimuli and task
Visual stimuli were controlled by a personal computer running a custom presentation software (Stimulus v.2.3), and were delivered through MRI compatible LCD goggles (Resonance Technologies, Northridge, CA, USA). During the anatomical data acquisition subjects watched a movie with natural scenes for relaxation and familiarization with the procedure. Stimuli consisted of line patterns formed by 8 rows of 12 parallel oblique (30 degrees) white bright bars on a black background, alternating rhythmically every half second with similar bars orientated 30 degrees to the opposite direction.
In the control condition, bars were always parallel to each other in the whole viewing area. In the main conditions, hereafter called ‘left-angle’ and ‘right-angle’, a column of bars, either on the left or right side, was orientated towards the opposite direction, always forming 60-degree angles with the remaining bars. The visual stimuli encompassed approximately 90–100 degrees of the angular field of view. Our intention was to stimulate both central and peripheral fields. Although we initially planned to provide selective right or left hemifield stimulation with angles, due to technical limitations of the maximum field of view and because of the existence of massive callosal connections allowing visual transfer between hemispheres, both sides could have been stimulated with angles in either condition. In the left-angle condition, the incongruent bars were presented to the left side, whereas in the right-angle condition they were presented to the right side (Fig. 1). Thus, a vast extension of the visual field was constantly stimulated by the parallel bar patterns, but in the angle conditions bars forming 60-degree angles were presented either to the left or right side. Every condition block lasted 15 s. Subjects were instructed to keep constant visual attention at a central red spot, which was always present at the centre of the visual patterns.
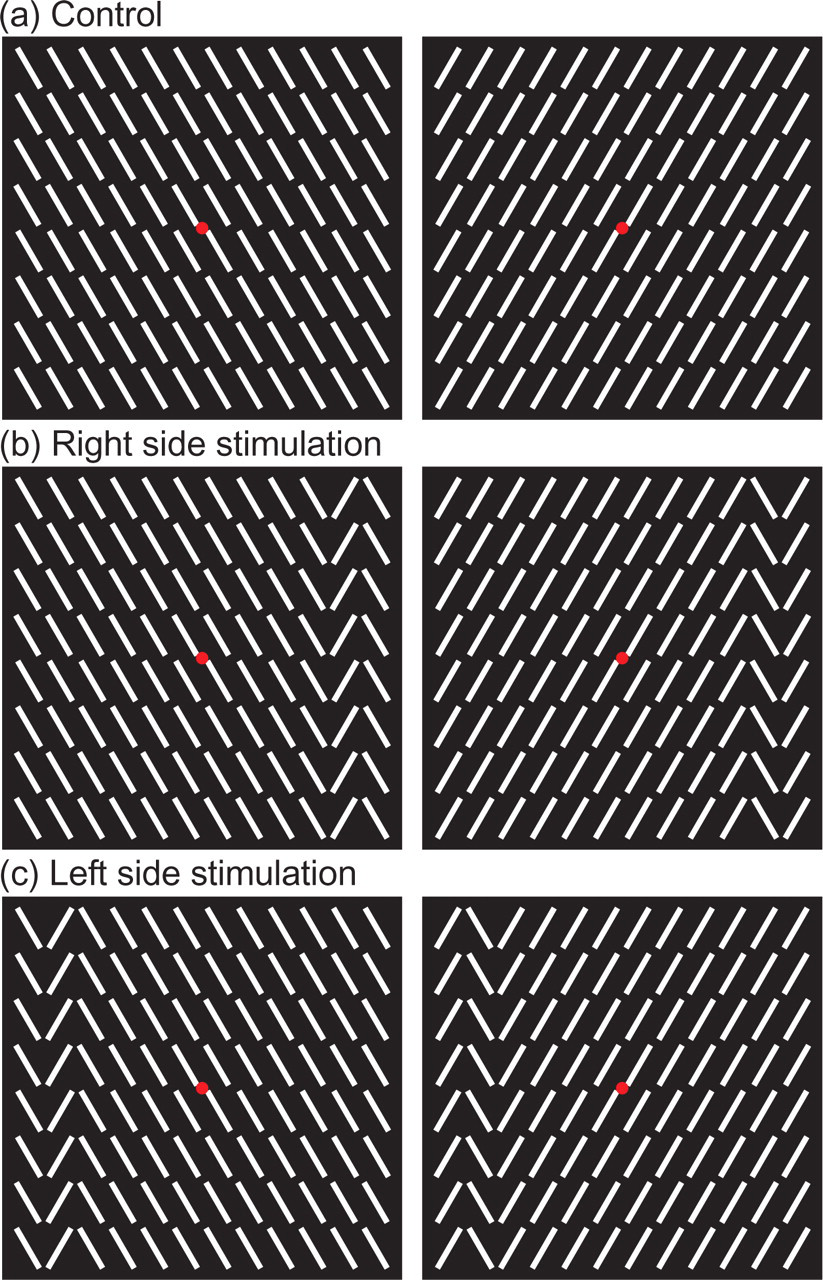
Visual stimulation with alternating images during signal acquisition. (a) corresponding to the baseline epoch, no angular stimuli were presented (control stimuli). (b, c) corresponding to the right-angle and left angle epochs, 60 degree angles formed by a column of contra-inclined bars were present at the right and left sides, respectively (incongruent stimuli). Each epoch lasted 15 s and contained 30 alternations of the specific visual patterns. The whole experiment involved 6 epochs for each main condition (left- or right-angle, b, c) interposed by a 15-s baseline epoch (a). Subjects were instructed to keep constant visual attention to the central red dot.
Functional MRI acquisition and analysis
Functional MRI was performed with a 1.5 MRI scanner (Siemens Vision, Germany). Anatomic data consisted of 128 high-resolution gradient-echo T1-weighted volumetric images (slice thickness = 1.25 mm). Head movements were restrained by foam padding. Functional images covering the whole brain were acquired across 16 slices parallel to the plane of the anterior and posterior commissures with echoplanar BOLD technique (TR/TE = 3000/66 ms, FA = 90°, matrix size = 96 × 128, FOV = 256 mm, thickness/gap = 5/0.25 mm). One hundred and twenty functional volumes, or TRs, were collected for each subject. Each epoch (right-angle, left-angle or baseline conditions) lasted 15 s and contained 30 alternations of the specific visual patterns (Figure each TR of 3 s containing 6 alternations; 5 TR s × 6 = 30 alternations, or 15 s). There were 6 epochs for each main condition (left-angle or right-angle). Since main condition epochs were interposed with a 15-s baseline epoch, there were 12 baseline epochs. Therefore, a total of 24 epochs (12 baseline, 6 right-angle and 6 left-angle) comprised the whole experiment (24 epochs × 5TR/epoch = 120 TRs). The stimulation with the sequence of different epochs was therefore as follows: baseline – left-angle – baseline – right-angle – baseline – left-angle – baseline – right-angle, and so on. Functional datasets were motion-corrected and highpass-filtered in the frequency domain. No individual data exceeded 0.4 mm of rotation or translation during acquisition. Spatial normalization with a 4-mm FWHM 3D gaussian kernel was used. Structural and functional volumes were transformed into standard Talairach-Tournoux stereotaxic space (20).
Activations were computed using statistical parametric mapping methods (21). Left- and right-angle stimulations were the conditions of interest, and parallel bar stimulation was the baseline condition. The reference time-courses were created by applying a canonical haemodynamic response function to the square-wave representing either the left- or right-angle condition. Using this filter, the modelled BOLD response peaked with a 6-s delay. Significance was assessed by setting P < 0.0001 (uncorrected for multiple comparisons). A 3D cluster-size extent threshold corresponding to 100 mm3 was used to further protect against Type-I errors (22). The resulting colour-coded statistical maps were individually overlaid on anatomical images acquired from each subject.
The individual parametric activation maps thus generated were charted to anatomical regions by one of the authors (JM), as described elsewhere (23). Regional activations were nominally rated as 1 (present) or 0 (absent). Results were statistically compared with the Mann–Whitney test (U), two-tailed. A significance threshold (α) of 0.05 was adopted for all comparisons (24). Given the small number of subjects in each group, comparisons were restricted to relatively large anatomical regions of interest.
Results
Visual stimulation and MR acquisition procedures were well tolerated by both patient and control groups. Two patients reported no symptoms during image acquisitions and for the ensuing 4 weeks (subjects RI and CAR). Patient RSN presented mild headache 24 h later. One subject (RAQ) described small blueish small circles in her right hemifield, regardless the side of stimulation. During the control epochs, she reported seeing horizontal lines. After 20 min she noticed a moderate headache with nausea that lasted 24 h, without aura. Patient NE reported scintillations in the right hemifield during the natural scenes projection, no visual symptoms or headache during fMRI acquisition.
The activation patterns of control subjects were examined first (Fig. 2). In 4 of them there was activation in the medial and anterior orbitofrontal cortex when the incongruent (angle) condition was compared to the baseline. This was the only significantly activated brain region in three of these subjects. One subject showed an additional activation encompassing the right nucleus accumbens/ventral striatum and right ventral pallidum in response to the left-angle condition. In the remaining control subject a single activation cluster was present in the left visual cortex close to the calcarine sulcus when the angles were presented to the ipsilateral side. Although significant effects related to the angle vs. parallel condition task were found in all individuals, there was no relationship between the stimulated side and the side of activation in the basal frontal lobes.

Activation in controls. Subject initials and the side of visual stimulation are shown for each subject. Areas of activation highlighted by white squares are repeated in greater detail.
Results in migraineurs stood in sharp contrast to what was observed in controls (Table 2). All patients showed significant activations in the visual cortex, and none of them had activations in the frontal cortex or basal forebrain. Most activated clusters (depicted in Fig. 3) were found in extrastriate and striate visual cortex. Although retinotopic mapping was not carried out in the present study, visual analysis suggested that most of these activated clusters corresponded to Brodmann's areas (BA) 17 (calcarine region) and 18, located in the lingual, occipital and fusiform gyri (hereafter collectively referred to as peristriate cortex). In 4 of the 5 subjects (nos. 1, 4, 5 and 3), visual cortex activation contralateral to the side stimulated by angles was detected. In one patient (no. 2), the activation fell close to the midline, making it difficult to make a lateralization assumption. In one subject (no. 4), the left occipital cortex was activated regardless of the side stimulated by angles. In two subjects additional activations were found outside the peristriate cortex. They were located in the cortex adjacent to the intraoccipital sulcus (no. 4) and in the anterior portion of the middle temporal gyrus (no. 5), both contralateral to side stimulation by the angle condition.

Activation in patients. Subject initials and the side of visual stimulation are shown for each subject. Areas of activation highlighted by white squares are repeated in greater detail.
Centre Talairach coordinates

Overall, all migraine subjects activated occipital visual areas in response to the incongruent bar stimuli, while only one control subject did so. In contrast, 4 control subjects activated basal frontal lobe, a region that was not activated in any of the migraine patients. A comparison by anatomical regions of interest showed significant differences in activation between controls and patients in the orbitofrontal (U = 2.50, P= 0.014) and visual cortex (U = 2.50, P= 0.014), but not in basal forebrain structures (U = 10.0, P= 0.31).
Discussion
The present experiments were designed to address the responsiveness of the migrainous brain to a visual stimulation pattern containing angles, presumably an important component of the naturally occurring fortification spectra. The results indicate that the migrainous occipital cortex is especially responsive to this stimulation pattern as compared to the cortex of controls. Besides, these differential responses do not appear to be attack-dependent, as all subjects were examined interictally.
The first fMRI study ever performed addressed visual activity, and functional aspects of the human occipital cortex have been extensively studied since (25). BOLD-fMRI imaging is sensitive to changes in tissue content of oxy- and deoxy-haemoglobin in small vessels of brain parenchyma, which occur in response to sensory, motor or cognitive tasks. These changes can reflect local increases in blood flow related to alterations in neuronal activity (26). Deoxy-haemoglobin is paramagnetic, causing a MR signal drop due to locally increased field homogeneity. Since the increased delivery of oxygen molecules to an activated brain region is in excess of the increase in oxygen consumption, the surplus of oxygenated blood results in an increase in the MR signal. The finding of increased BOLD responses to incongruently orientated bars in migraine visual cortex points to an enhanced metabolic response in visual cortical areas in migraine patients involved with this particular visual perception.
The present findings are indicative of a lower activation threshold in visual areas of the cortex stimulated by the incongruent stimuli in migraine. The peristriate visual cortex was reliably activated in migraine with aura patients when the incongruent stimuli was presented, as compared to the parallel bar condition. The peristriate cortex includes the putative V1 and V2/V3/V4 areas, which constitute early cortical visual processing stages. These regions shelter orientation-responsive neurones (27). Besides, activation of extrastriate cortical areas similar to those here described in migraine patients have been found to respond more selectively to visual textures (28). Perceptually, the orientated bars used in our study may indeed appear as a texture, thereby activating texture-processing visual regions. Non-complex, linear and angulated flashes of light typical of migraine aura may be the result of abnormal activity of neurones in these early visual processing regions. Functional MRI responses are typically based on a difference in signal intensity obtained by contrasting one stimulus condition with another, ideally matched for all aspects, except for the variable of interest. Our results show predominantly contralateral, but not exclusive, visual cortex activation in response to left- or right-sided presentation of angle stimuli. As described before, though angles were presented to the right or left eye, there were technical constraints in the maximum viewing angle of the screen, i.e. stimulation was not entirely hemifield-selective. Besides, interhemispheric visual transfer via the splenium of the callosum would preclude any attempt to selectively stimulate the visual cortex of each hemisphere. Nevertheless, the eccentricity of the columns having incongruent bars was logically smaller relative to the ipsilateral visual field. Therefore, angle stimulation fell closer to the foveal field of the ipsilateral eye; which might have influenced the lateralization of the activation responses.
Relatively few fMRI studies of migraine are available so far, and most of them have focused on cortical changes during migraine aura. Spontaneous visual auras in 4 migraine patients have been studied using perfusion- and diffusion-weighted magnetic resonance imaging. A decrease in relative cerebral blood flow and blood volume was observed (29). Stimulation with a red-green checkerboard and BOLD-fMRI was used to study 10 migraineurs and 6 controls (10). A spreading suppression of an initially increased occipital cortex oxygenation was detected in some of the subjects in whom attacks were triggered. This change propagated across the occipital cortex at a rate of 3–6 mm/min, suggesting a link with an SD-like phenomenon. Similar stimulation was used to study both spontaneous and triggered migraine with aura attacks in 3 male migraineurs (11). A spreading increase in BOLD signal progressing over the occipital cortex by 3.5 mm/min was detected, in accordance to the retinotopy of the visual percept. Repeated checkerboard visual stimulation in a BOLD-fMRI study was used to demonstrate a MR signal increase in the red nucleus and substantia nigra before occipital cortex signal elevation or the onset of visually triggered symptoms in the majority of subjects, indicating that such areas at the brain stem could be activated during a migraine attack (30). In the present study, no activation was detected in the brain stem. This could be related to the fact that migraine attacks were not triggered in our patients, in contrast to study mentioned above.
As firstly hypothesized by Leão, SD has potential implications in the pathophysiology of migraine (6, 31). It has been demonstrated that a spreading hypoperfusion with a progression rate of 2–3 mm/min may be detected in the cortex of migraine with aura patients (32, 33). Based on the hypothesis that SD or a similar phenomenon underlies migraine aura, focal circulatory abnormalities are expected during attack. The fMRI studies addressing migraine triggered visual stimulation strongly support the role of SD in migraine (10, 11).
Though the study of pathophysiological phenomena during migraine with aura attacks certainly offer new insights on the mechanisms underlying these processes, investigation of the migraineous cortex during the interictal periods may offer a whole new venue for the understanding of migraine. This study provides new evidence for differential response of the migraineous cortex to specific visual stimuli (angles) during the interictal phase. Although our results reflect the activation patterns in a relatively small number of subjects, they support the idea that the noncomplex, linear and angulated flashes of light typical of migraine aura are the result of activity in early stage processing areas of the visual cortex. Whether SD starts in the same areas during attacks is an interesting question that could be tackled by future fMRI studies combining similar visual stimulation protocols with effective provocation of visual aura symptoms. In one subject who had migraine with aura triggered by basketball playing, the BOLD signal appeared first in the V3A area (11). Because the aura described by their patient did not have the typical serration pattern (‘scintillating white noise, like TV snow’), no specific relationships can be safely drawn with those of the present study. In contrast to the above mentioned studies, our patients were evaluated interictally and our visual stimulation procedure was fundamentally different. Besides, it is known from clinical experience that aura of different modalities may start in various cortical areas, perhaps even simultaneously. As pointed out by Hadjikhani et al. auras could arise from many extrastriate areas (e.g. V2, V3/VP, V3A, V4v), as well as from V1. These authors also pondered that ‘other types of migraine aura, e.g. those containing corrugated lines might initiate in area V1’ (11). The differences in stimulation methodology could also explain why they did not find any signal changes in interictal acquisitions, in contrast to the present results. The activation of distinct regions in the striate and extrastriate visual cortex is in accordance with these observations, and may reflect a variability of abnormal cortical excitability in different patients. Further studies with larger samples are necessary to eventually establish a correlation between specific aura patterns and corresponding areas of interictal cortical abnormal excitability.
Why normal controls, but not patients, activated the OFC remains an intriguing question. The ventral and medial frontal cortex is critically involved in the brain mechanisms of punishment and reward (34). The orbitofrontal cortex (OFC) receives input from all sensory modalities and assigns values and emotional relevance to them accordingly. It has been demonstrated that the OFC is also involved with visual target detection and selection (35). Since we did not require our subjects to perform any overt cognitive processing of the visual stimuli, we cannot safely attribute these activations to visual selection mechanisms, although covert processing could well have occurred. It remains to be determined whether the lack of OFC activation in patients is related to the migraine pathophysiology or, alternatively, it reflects an epiphenomenon related to behavioural variables.
Being migraine a paroxysmal disorder of neurological origin (36), occurring in patients with a genetic predisposition (37), the findings shown herein may support, in such patients, the possibility of a permanent cortical susceptibility to a periodic cascade of events leading to migraine attacks. An attack would start by activation of migraine generators at the brain stem and SD-susceptible areas at the visual cortex. Secondary activation of trigemino-vascular structures would complement the attack events (36).
Conclusion
The present findings suggest that interictal cortical responses following visual stimuli in migraine patients and control subjects are distinct. Regardless of whether the visual areas activated in the present study are related to the actual regions that give rise to the migraine visual fortification aura, our fMRI paradigm provides a novel tool to explore additional aspects of migraine pathophysiology.