
Abstract
The trigeminal autonomic cephalgias (TACs) are characterized by short-lasting unilateral headaches with autonomic features (1). They include four headache disorders, cluster headache (CH), paroxysmal hemicrania (PH), SUNCT syndrome and hemicrania continua (HC). The coexistence of different ipsilateral TACs in the same patient has been previously reported in six published cases (2-6). In five of these patients an association of CH and PH was noted (2-5). The two varieties of attacks occurred separately in three patients, while their simultaneous occurrence was observed in two cases. In another patient the successive occurrence of trigeminal neuralgia, SUNCT syndrome, PH and CH in one active headache period was noted (6). All the reported cases concerned male patients. We describe what we believe to be the first case of coexistence of two different contralateral TACs.
The trigeminal autonomic cephalgias (TACs) are characterized by short-lasting unilateral headaches with autonomic features (1). They include four headache disorders, cluster headache (CH), paroxysmal hemicrania (PH), SUNCT syndrome and hemicrania continua (HC). The coexistence of different ipsilateral TACs in the same patient has been previously reported in six published cases (2–6). In five of these patients an association of CH and PH was noted (2–5). The two varieties of attacks occurred separately in three patients, while their simultaneous occurrence was observed in two cases. In another patient the successive occurrence of trigeminal neuralgia, SUNCT syndrome, PH and CH in one active headache period was noted (6). All the reported cases concerned male patients. We describe what we believe to be the first case of coexistence of two different contralateral TACs.
Case report
A 32-year-old man presented with a 8-year history of daily right-sided headaches and with a 4-year history of episodic left-sided pain attacks. The characteristics of the two headaches are summarized in Table 1.
Clinical features of the two contralateral headaches
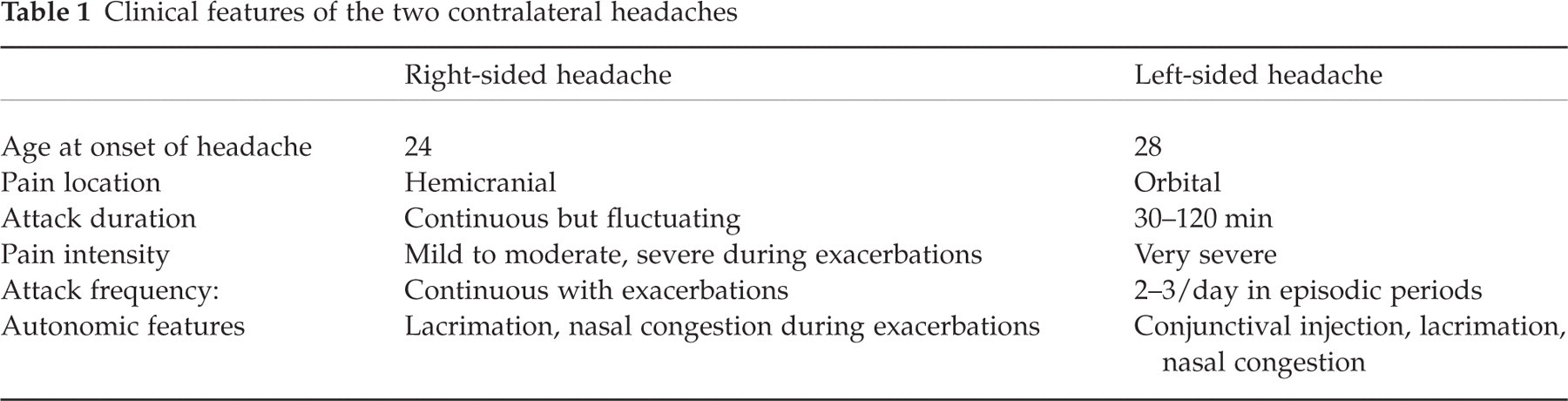
The past medical history was unremarkable; there was no family history of headache. The right-sided hemicranial headache was constant, but waxed and waned in severity. The pain was usually mild to moderate but from two to four times a month the patient experienced exacerbations which lasted up to 12 h. They were characterized by more severe right periorbital pain accompanied by ipsilateral lacrimation and nasal congestion. He had been treated with several non-steroidal anti-inflammatory drugs, but not with indomethacin, without relief. The left-sided headache fulfilled the International Headache Society (IHS) diagnostic criteria for episodic CH. The pain was located in the left right temple behind the eye; it was extremely severe and was associated with ipsilateral conjunctival injection, lacrimation and nasal congestion. The pain attacks occurred two to three times a day and their duration was 30–120 min. The attacks came in bouts of 1 month with intervening breaks of 5–7 months. We first saw the patient during a cluster period and we started a preventive treatment with verapamil 360 mg daily. The attacks responded completely to subcutaneous sumatriptan. After 1 week the left-sided headaches abated, but the contralateral pain remained continuous with periodical fluctuations, as it was between the bouts of CH. Verapamil was gradually tapered off in 3 weeks, with no recurrence of the left-sided attacks. Neurological examination and routine laboratory studies were unremarkable. Magnetic resonance imaging of the brain was normal. Following a tentative diagnosis of HC, the patient was commenced on indomethacin 50 mg b.d. and his daily right-sided headaches resolved following each dose. His regimen was gradually decreased to a final dose of 25 mg b.d., with no recurrence of the pain. When we tried to taper the drug, the pain recurred within 3 days and again settled rapidly when indomethacin was restarted at the same dose. The patient has been headache-free since then, with a follow-up of 1 year.
Discussion
In our patient the two unilateral headaches met, respectively, the IHS criteria for episodic CH and the criteria for HC proposed by Goadsby and Lipton (1) and recently revised by Pareja et al. (7). An interesting point made by our observation is the selective response of each variety of headache to different drugs. CH attacks disappeared with verapamil but were unresponsive to indomethacin, whereas HC pain responded completely to indomethacin but was not modified by verapamil and sumatriptan. It remains unclear whether the two headaches might share some pathophysiological aspects, possibly involving, in light of recent findings with CH, a central nervous system locus (8). Further studies could help to clarify this question.