
Abstract
The objective of this study was to gain insight into the patients' decision-making for migraine and chronic daily headache management. Patients were recruited by theoretical sampling in Surrey (UK). Semi-structured and tape-recorded interviews (n = 13) were conducted, transcribed verbatim, coded and analysed according to the grounded theory methodology. Thirteen patients (8 migraine and 5 chronic daily headache) described their management. All patients employed multiple behaviours to manage their headaches. From the patients' descriptions emerged their decision-making. Based on experience, perceptions and new information, the decision-making process involved four stages: headache severity, evaluation, decision making and behaviours. Although the participants were passive with regards to certain management strategies, overall they were actively involved in treating and preventing their headaches. Furthermore, they were active decision-makers in choosing appropriate management. Migraine and chronic daily headache patients are actively involved in managing their headaches. They are key decision-makers and should not be overlooked as a resource for effective management.
Introduction
Affecting about 12% of the population, migraine is a chronic disease with acute episodes and needs to be managed over a prolonged period of time. To date, migraine is under-diagnosed and under-treated (1, 2). Initiatives taken to improve management in clinical practice have mainly focused on facilitating the physicians’ role in the management of migraine by providing guidelines (3, 4), disability assessment tools (5) and stratified care (6). The low consultation rates and the under-use of prescription medication, suggest that migraineurs learn to cope and live with their disease, rather than actively seek effective treatment (7). Consequently the burden of migraine remains great, and most migraineurs suffer at least some disability and have a reduced quality of life. However, with the wide range of management strategies available, it is possible to improve headache management and ease the suffering of many migraineurs.
Since ‘headache control is best when patients play an active role in their treatment’ p. S46 (8), the patients’ involvement in the treatment of their disease is essential. Selecting a suitable and effective therapy can be a complex task for both the physician and the patient. Recent publications (8, 9) and headache management guidelines (3, 4, 10), predominantly educate the physician on selecting appropriate drug therapy for individual migraineurs. The Migraine in Primary Care Advisors (MIPCA) guidelines (3) additionally educate practice nurses and pharmacists about migraine management, to move towards patient centred care. However, since the majority of migraineurs do not consult their physician about their condition (11, 12), they do not benefit from the physician's expertise and from prescription medication. Furthermore, as attacks occur generally in the absence of the physician, patients, even those who do consult, need, and maybe even prefer, to make their own choices for managing their migraines.
Few studies have addressed the patients’ perspective in the management of headache. Studies to date focus on what migraine patients want from medical consultations (13) and their satisfaction (14) and preferences for acute drug therapy to compare medication (15) or different doses of the same medication (16). These studies shed some light on the patient perspective, but by remaining focused on physicians’ consultations and acute medications, they fail to recognize other management strategies that the patients may choose to adopt, as well as the factors that influence the patients’ decision-making.
Furthermore, the issues investigated in these studies were determined by the researchers. Little opportunity has been given to the patients to speak openly and unrestrictedly about the factors that influence their decisions for migraine and chronic daily headache (CDH) management. Qualitative research provides the opportunity to address these limitations. Qualitative research has been applied in non-headache research to explore similar research questions, for example in asthma management (17). Concerned with understanding the perspectives, interpretations and meanings of the world of those who are being researched (18, 19), qualitative research reveals new phenomena and complexity by giving voice to those whose views are rarely heard (20). The data presented in this article are part of a study, which aimed at gaining insight into the patients’ perspective and into the factors influencing migraine and CDH management. This article sets out to describe the factors involved in the patients’ decision-making.
Methods
Grounded theory
First described by Glaser and Strauss (21), grounded theory is a specific, highly developed and rigorous set of procedures for generating theory through comparative analysis. The theory emerges out of and is created through and grounded on empirical data (19). Grounded theory is mostly concerned with sampling and data analysis. There is no specified method of data collection, although interviews are commonly used. The steps involved in grounded theory include theoretical sampling, data collection and analysis through coding, writing notes and memos about key non-probability concepts and their relationships until theoretical saturation. The steps are closely interrelated and may be employed simultaneously.
Theoretical sampling is nonprobability sampling based on seeking participants who have the most experience of the topic of interest (22). Recruitment of participants is driven by the emerging theory. Analysis reveals gaps in the data and theories, and the researchers need to collect more data to fill these conceptual gaps (23). This is achieved by recruiting participants who add to the fullness of the concepts. Therefore, a grounded theory study is best conducted if each participant is only selected after the data from the previous participant has been analysed. Sampling continues until each concept is saturated.
Analysis begins early and data is analysed as it is collected. Analysis involves generating conceptual categories by comparing similar and different facts from the raw data (for example interview transcripts). Coding starts the chain of theory development. Data are studied to create codes or categories of data, which are grouped to gain a new perspective on the data and to collect further data (23). Once initial categories have been established, additional data are collected to further compare concepts with more empirical indicators and with each other to sharpen the definition of the concepts and to define their properties (24). Theories are formed from proposing plausible relationships among sets of concepts (24). The evidence from which the categories and concepts emerge is used to illustrate the concepts (21). Comparisons continue until theoretical saturation, i.e. additional data do not contribute anything new to the concepts (24).
Recruitment, data collection and analysis
Ethical approval was obtained from the University of Surrey Ethics Committee. Recruitment, data collection and analysis were carried out simultaneously by MP (unless stated otherwise), in accordance with the grounded theory methodology. This allowed for theoretical sampling, revision of the interview guide, to help with data interpretation and to identify emerging themes and data and theoretical saturation.
Recruitment
Based on theoretical sampling, a convenience sample, consisting of 15 adults, was recruited in Surrey (UK). The participants, aged 18–65 years, were suffering from migraine according to the International Headache Society (IHS) criteria (25). Patients with coexisting headaches or patients who had developed CDH were not excluded. For the purpose of this study, CDH was defined as headaches occurring at a frequency above 15 days per month. Initially participants were recruited through personal contacts (MP, MM). Since this mainly led to recruitment of migraineurs within the University, posters were put up in 2 local supermarkets to broaden the background of the participants. Finally, letters were sent to 20 members of the Migraine Action Association to complete the sample. A total of 39 patients had been contacted and 15 were recruited. The patients, who were not recruited, did not suffer from IHS migraine, could not be interviewed during the time of the study or could not contribute to the emerging theory.
The participants were recruited to reflect a range of characteristics (dissimilar cases). The aim was to include 1 male to every 3 female sufferers (to reflect migraine prevalence), a variety of socio-demographics and one participant per age group, per disability group and per consultation group. Socio-demographic factors were determined by the participants’ marital and employment status, type of employment and/or level of education. There were 4 age groups: 18–29, 30–39, 40–49 and 50–65. Consultation status was determined according to Lipton and Stewart's criteria (14). Patients who had never consulted a physician about migraine were classed as ‘never consulter’. Patients who had consulted within the last year were classed as ‘current consulter’ and those who had not consulted for more than one year were classed as ‘lapsed consulter’. Disability assessment (by MIDAS questionnaire) was used to include patients with varying levels of headache severity, which was reflected in their current headache status of migraine or CDH.
Data collection
Interviews were semistructured, individual and tape-recorded. A flexible interview guide was devised by the authors based on recent migraine literature to comprise opening and more specific follow-on or clarifying questions and prompts. Opening question were aimed to be nonleading (Table 1), whereas follow-on questions tended to be more leading. Initially the interviews focused on migraine experience, physician consultations and treatments for migraine. However, with the emerging theory, and as part of the verification procedure, the interview guide was further developed to include previously raised issues and emerging concepts. Additional questions focused on patients’ preferences, choices and decisions and a more holistic approach to management (i.e. beyond physicians’ consultations and pharmacological treatments).
Opening interview questions

Interviews were arranged to the participants’ convenience, at their home, work place or at the University of Surrey. One participant withdrew before the interview and 14 migraineurs, who all signed the consent form, were interviewed once. Interviews lasted up to 2 h with recording time averaging 1 h (range 50–90 min). The first interview served as a pilot interview and was not included in the analysis. HAS and VV read interviews to assess interview technique and content. Interviewing finished with data saturation. Interviews were transcribed verbatim. Participants were offered a copy of their interview transcript.
Analysis
Interviews were prepared for analysis and coded using QSR NUD∗IST5 (N5), a qualitative software package. The interview transcripts were imported as text files into N5 to be coded. In N5, data are coded by units of text (either paragraphs, lines or sentences). In this study, the raw data were coded sentence by sentence. The aim of N5 is to code and re-arrange data according to the emerging codes and to build a hierarchical taxonomy within the software, while keeping memos with the raw data and the emerging codes.
To reduce bias of the coding scheme and emerging taxonomy and concepts, all authors, as well as an independent researcher, were involved in different stages of the analysis. A guide was devised (by MP and HAS) to standardize the coding procedure for triangulation. One by one, the first 5 interviews were summarized (by MP, HAS, VV and an independent researcher). Then the interviews were coded sentence by sentence to give an initial coding scheme (MP, VV and an independent researcher). No notable differences were found between the coding of different researchers. Codes were grouped into a hierarchical taxonomy to form concepts and theories. These concepts and theories were based on theoretical memos and discussions between the authors. The last 8 interviews, coded according to the same technique, were used to verify the coding scheme and refine the emerging taxonomy and concepts. First, a summary of the concepts and later detailed definitions, descriptions and interpretations of the main concepts were discussed by all authors.
Results
The descriptive codes that emerged from the interviews related to the interview questions. These codes were grouped into three main themes: headaches, consultations and management. These themes gave the base data of the participants to describe the patients’ characteristics and the patients’ subjective reality of headache management (consultations and strategies).
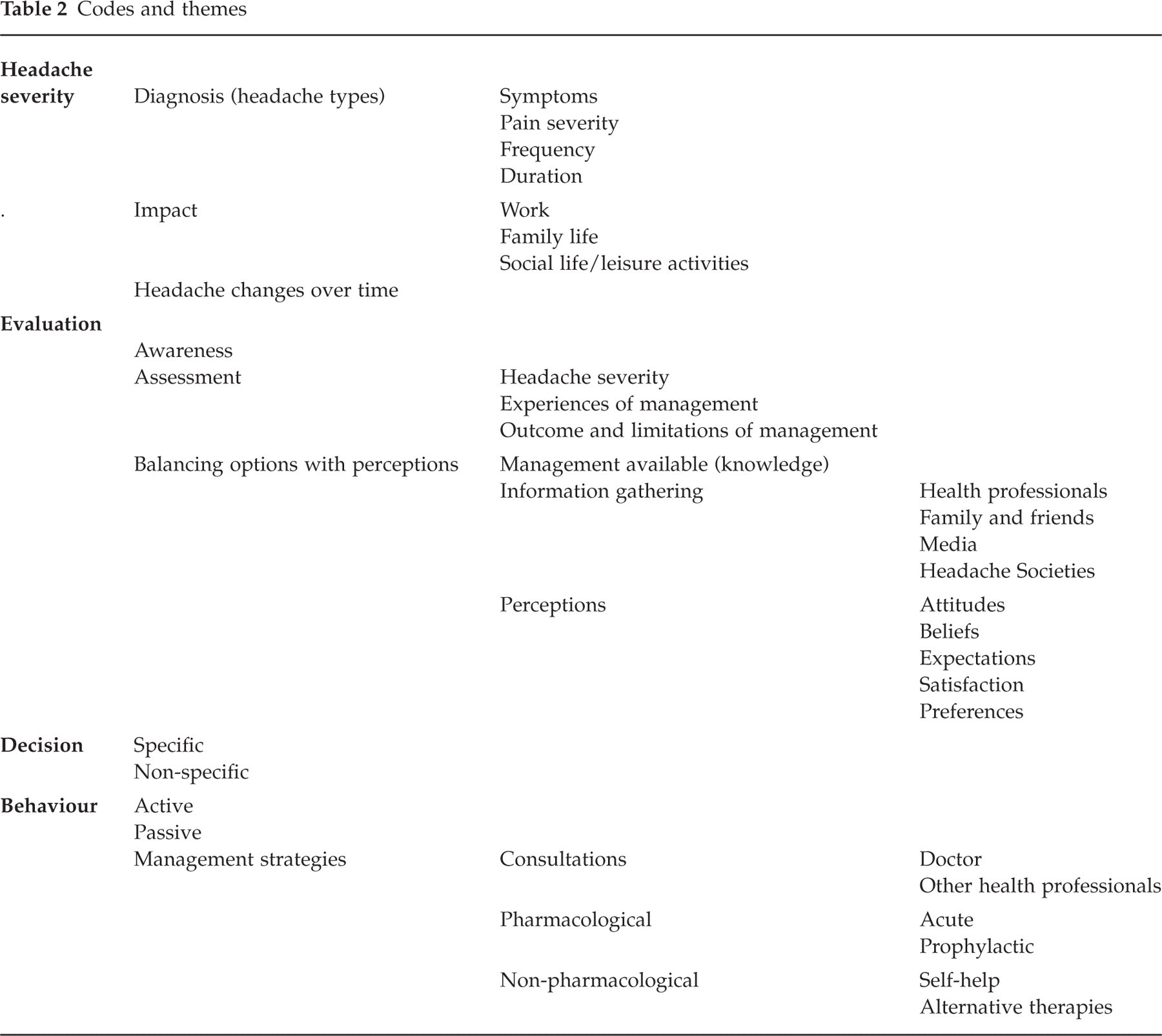
Furthermore, the patients explained their reasons for using or not using management strategies, by relying on and generalizing from their subjective experiences, which they perceived as significant in their management decisions. The interpretative codes (Table 2) of the descriptive themes, revealed the patients’ involvement in their headache management and the 4 stages of decision-making. Drawing on their experiences, the patients were the key decision-makers for the management of their headaches.
Codes and themes
Patients’ characteristics
All 13 participants (9 women and 4 men, aged from 24 to 60) suffered from IHS migraine. Three patients also suffered from tension-type headache (TTH). Based on their headache frequency above 15 days per months, 6 patients were classed as CDH patients. These patients experienced higher frequency and lower severity headaches, as well as full migraine attacks. Of these 6 patients, one had been effectively treated and did not suffer from CDH at the time of the study. One participant was a ‘never consulter’ for migraine, 6 participants were ‘lapsed consulters’ and 6 participants were ‘current consulters’. Current consultations were associated with the diagnosis of CDH. Four participants (1 lapsed and 3 current consulters) had consulted either a headache specialist or a neurologist. MIDAS scores ranged from 0 to 47. The individual patients’ characteristics are described in Table 3.
Patient description

CDH, chronic daily headache; TTH, tension-type headache.
Management strategies
All participants described a range of management strategies and self-help measures that they had used in the past or were still using at the time of the interview. All participants used several strategies at any one time. The combination of strategies used was individual to every patient. Management strategies included such as medication, consultations with health care professionals, trigger detection and avoidance and gathering information from family and friends, the media and specialized organizations. The participants described their adoption, maintenance and cessation of their personal management strategies over time.
The four stages of decision-making
Through the patients’ descriptions of their management strategies emerged their decision-making to adopt, maintain or discontinue management behaviours. Four stages of decision-making, that were linked in a cyclical process (see Fig. 1), were identified. The 4 stages were: headache severity, evaluation, decision and behaviour. Decision-making was a complex, dynamic and continuous process that developed over time and operated on a justification and consequence system. Every decision, behaviour and change in migraine severity added to the experience and perceptions of the patients. In the figure (Fig. 1), the shadows represent the experience, illustrating the influences of previous decision-making. These experiences, perceptions and newly gathered information influenced the outcome of their next decision, behaviour and headache severity.

The patients’ process of decision-making for headache (migraine and chronic daily headache) management.
Headache severity
Headache severity, an objective and factual stage, comprised the diagnosis (symptoms, pain severity, frequency and duration) of migraine, CDH and TTH, the progressive nature of migraine during attacks and over the years and impact of the headaches. Patient 8 described the progressive nature of migraine: ‘… I would say that the migraines got noticeably worse in the last five or six years …’. Patient 7 outlined the impact of migraines on work: ‘… I’ll have the days off for the migraines and then I tend to be not at full capacity the day after …’
The onset of the headaches and their severity were the starting point of decision-making. Patient 6 explains how the pain severity induces her to rely on medication: ‘… the thing that really affects my working efficiency and just generally affects me, is the pain. Obviously I want to relieve the pain, so therefore I’m taking painkillers …’ However, headache severity was also an end-point as it served as an outcome measure to assess the efficacy of the management strategies. Patient 13 explains how headache severity served as outcome measure: ‘… try avoiding food, I gave up chocolate, cheese and red wine for three months … they made no difference, I still got headaches, even when I wasn’t taking it and then when I re-introduced it …’.
Evaluation
Evaluation was the most active, involved and complex stage of decision-making. It comprised 3 steps including awareness, assessment and balancing options with perceptions. Awareness was when the patients’ stopped believing that their migraines or headaches will not come back and they started thinking about how to deal with the problem.
The patients progressed to assess their headache severity, their experiences of headache management and the outcome and limitations of the previously employed strategies. Patient 2 recognized the limitations of his own ideas for headache management and resorted to a GP consultation: ‘… the initial ideas came from me, but there were some things, obviously without medical knowledge; I don’t have medical knowledge, so I thought the GP could certainly say “this is possibly a cause, you haven’t thought of this” …’.
The participants described options for pharmacological and nonpharmacological treatment. Knowledge about management strategies was acquired through the participants’ own and other people's experiences and through information gathering. New management strategies were learnt by actively seeking and/or spontaneously receiving information and advice from other people (health professionals, family and friends), the media and specialized migraine organizations. The patients balanced treatment options with their individual perceptions to underpin their decisions. For example for Patient 6, the severity of migraines did not justify prophylaxis: ‘… although migraines are bad, I don’t know if I’d want to take medication every day …’ and Patient 13 opted against acupuncture due to personal preference: ‘… the GP did mention acupuncture, but I don’t believe in acupuncture, so I didn’t choose that …’.
Perceptions, included preferences, satisfaction, expectations, beliefs, and attitudes. They were influenced by the participants’ personality and their and other people's experiences of health care, particularly migraine management, and the health care system. Based on her satisfaction with her GP generally, Patient 6 chooses to consult: ‘… the doctor I’ve got is very good and he's very understanding and he does listen and discuss things with you. So I thought it would be interesting to have his opinion on them [migraines], to see if there is anything that he could suggest …’ Difficulties with evaluation, and the patients’ subsequent decisions, arose with misconceptions, when the management outcome was not clear or when there was conflict between the patients’ preferences and the management approach. Patient 1 outlines how her beliefs about treatments influenced her consultation behaviour: ‘… I didn’t really think that there were particularly effective treatments. and if I don’t expect there to be anything for me … [consulting the GP]is a waste of time …’.
Other people influenced the participants’ evaluations and sometimes convinced or hindered the participants to take action. Patient 12 was encouraged by his wife to try various treatments: ‘… A[wife]is now pushing me to have reflexology, which apparently some people say is good for migraine … so I’m now considering that …’ As the central figure, the migraineurs felt that they knew best and the final decision was theirs, as Patient 13 explained: ‘… [the GP]couldn’t argue with me, because that was my opinion …’.
Decision
Evaluation served as justification for the decisions these patients made for their headache management. Patient 7 assessed the type of headache and accordingly selected treatment to achieve the best outcome: ‘… you work out what you think it's going to turn into and therefore taking the drugs that you will think will best suit it …’. Decision was an active stage that described the patients’ choices for management. Decision, the outcome of evaluation, was often a compromise between their options and perceptions. Decisions were specific and non-specific. Specific decisions were those related to a specified management strategy, whereas non-specific decisions were general decisions to headache management. Non-specific decision were described as follows by Patient 2: ‘… I want to move forward and try and deal with the problems …’; and a specific decision was outlined by Patient 13: ‘… I told him[GP]that I was going to the chiropractor and that I didn’t want to take the drugs[beta-blockers] …’.
Behaviour
Following their decisions, the participants adopted, maintained or discontinued behaviours to manage their headaches acutely or prophylactically. Behaviour, which could be active or passive, outlined the participants’ past and current management strategies (trials and errors), as well as their individual management combinations. Patient 2 relied on the combination medication and lying down for acute treatment: ‘… the only way I can deal with the pain is to obviously take medication, but really to commit myself to bed …’ Patient 7 talked about her past experience with alternative therapies: ‘… I’ve tried Feverfew as well, I didn’t like the smell of those … and I have tried massaging smelly oils in my forehead, which didn’t really help …’. Depending on the failure or success of a behaviour, a change occurred in the headache severity, thus making headache severity an outcome measure and also adding further to experience on which to base their subsequent decisions. Patient 13 described how unsatisfactory headache relief motivated her to try a variety of medications: ‘… I went to the nurse and she gave me, I was taking Ibuprofen, but she gave me Co-codamol. and I was on maximum dose of that and it didn’t touch it. and then I went on maximum dose of Ibuprofen and Co-codamol together. That didn’t touch it. And then I was prescribed Diclofenac and that didn’t have any effect either. So after that I pretty much decided that if that couldn’t kick it, then I couldn’t do anything …
Discussion
The main finding was that these patients were actively involved in managing their migraines or CDH, through both their decision-making or their behaviours. The patients were the central or key figure of migraine and CDH management and decision-making. Four stages of decision-making were identified: headache severity, evaluation, decision and behaviour. As illustrated by Fig. 1, these 4 stages were linked in a cyclical process that developed over time through experience gained from previous decisions, behaviours and new information. Similar illustrations have been proposed for general decision-making (26), the self-management of asthma (17), and decision-making for taking sumatriptan (27).
Ivers et al. (27) described the decision-making process for taking sumatriptan based on symptom monitoring, evaluation outcome, treatment decision-making, health behaviour and final outcome. However, the sumatriptan decision-making model was limited to decisions about one drug for acute treatment for migraine. The results of this study add further to decision-making in headache management by bringing acute and preventive decision-making about different types of headache together.
The findings of this study reveal the complexity and provide a more holistic picture of migraine management, which brings a new perspective on quantitative findings. Migraine patients have been described as being passive and as having a fatalistic attitude (7). This may be true if migraine management or health care behaviours are studied in isolation. However, in this study, all the participants were active in managing their migraines and CDH, despite not relying on all the available options as for example physicians’ consultations. The role of these participants went beyond playing an active role in their management. As the key decision-makers for headache management, the patients’ integrated their knowledge with their experiences and perceptions to make decisions and adopt behaviours that suited their individual expectations and preferences. Furthermore, self-management strategies, based on the patients’ experiences and preferences and input from other people, were found to play an important role in the patients’ perceptions of the management of high impact headaches.
Chronic disease has become the principal medical problem and it is thought that the patient must become a partner, who contributes at almost every decision and action level (28). The doctor provides the general information and the patients provide individual information to achieve effective management (28). Initiatives that have been taken to improve migraine care, such as disability assessment tools (29, 30), stratified care (using information available at the initial consultation to choose treatment) (6) and headache management guidelines (3) are aimed at physicians. Although an important step in improving migraine care, these initiatives may overlook the migraineur as an essential resource of migraine management. Patients want to be informed of their treatment options and they want to be involved in decisions when more than one alternative treatment exists (7). The active role the participants adopted in decision-making and behaviours in this study illustrates the extent to which migraine and CDH patients want to be involved in the management of their condition. The chronic features of migraine and particularly CDH, the patients’ desire of involvement and the fact that headache control is best when patients play an active role in their treatment (8) demand the patients’ input into headache management.
Conclusion
The study aimed to gain insight into the patients’ perspective of migraine and CDH management. The descriptive results showed the holistic picture of management. Due the qualitative methodology these findings cannot be generalized. However, they can be used to inform headache researchers and clinicians about the patients’ perspective of migraine and CDH management. Furthermore, these results can be used to generate future quantitative work, from which broader conclusions can be drawn.
In addition to describing the holistic picture of the topic under study, qualitative research aims to understand, explain and reveal processes. This study showed how headache patients use their and other people's experiences to justify, explain and generalize their decisions and behaviours. Health care problems can only be addressed if the user's perspective is understood and if health care professionals and patients co-operate (31). By raising headache researchers’ and clinicians’ awareness of the patients’ involvement in their own migraine and headache care, the results of this study can be used to educate and empower the patient and to make headache research and clinical practice more patient-centred and relevant to the headache patient.
Footnotes
Acknowledgements
The authors would like to thank Dr Inez Bandell-Hoekstra for triangulation. This study was part-funded by AstraZeneca UK and the Migraine Action Association, UK