
Abstract
This study estimates the 1-year prevalence of migraine in adults in England in relation to the major demographic variables of age, gender and ethnicity, and describes some of its features, including aspects of consequential disability. A telephone survey was conducted of a random sample (n = 4007) of the population aged 16-65 years of mainland England using a previously validated diagnostic interview. The response rate was 76.5%. Overall, 7.6% of males and 18.3% of females reported migraine with or without aura within the last year meeting diagnostic criteria closely approximate to those of the International Headache Society. Prevalence of migraine varied with age, rising through early adult life and declining in the late 40s and early 50s. Prevalence was higher in Caucasians than in other races. Attack rates were ≥ 1/month in most migraineurs, and most experienced interference with daily activities in ≥ 50% of their attacks. On average, an estimated 5.7 working days were lost per year for every working or student migraineur, although the most disabled 10% accounted for 85% of the total. Results were in keeping with those from surveys in other countries. If these findings in mainland England are projected to the entire UK population, we estimate that 5.85 million people aged 16-65 years experience 190 000 migraine attacks every day and lose 25 million days from work or school each year because of them. Migraine is an important public health problem in the UK, associated with very substantial costs.
Introduction
Migraine is a common, episodic, temporarily disabling neurological disease. It imposes significant burdens on individuals and on society (1–3).
Prevalence estimates provide a measure of societal disease burden by indicating how many in a population have the disease during a defined period. Epidemiological studies can also identify groups of people at higher risk of disease, and the distribution of disability, as a prelude to devising interventions to reduce disease burden. Prevalence estimates for migraine have varied widely, depending on the methods used, the case definition applied and the demographic characteristics of the studied populations (2). The development of widely accepted diagnostic criteria for migraine by the International Headache Society (IHS) in 1988 (4) has resulted in more consistent estimates of migraine prevalence and an opportunity to make valid international comparisons. There are now more than 20 population-based studies of migraine in almost as many countries that have used the IHS criteria (2), but none published of migraine prevalence in the UK other than one paediatric (5) and one primarily economic study (6).
The present study estimates the 1-year prevalence of migraine in the UK by surveying a representative sample of the population of mainland England. Further objectives were to assess the distribution of the disease according to the major demographic variables in the population, measure some aspects of disease burden, and compare the figures for England with those from other countries.
Methods
A systematic sampling of households from the mainland of England was derived from the UK electoral register by Sample Answers Ltd (Teddington, UK), a UK-based geodemographic company. Up to 10 attempts were made to telephone each household by 62 trained lay interviewers. At the first successful contact, whoever answered the telephone was interviewed if eligible; if not, another household member selected by that person was interviewed instead. An eligible respondent was 16–65 years of age, a permanent resident of the household and able to converse easily in English.
After this interview, a household census was conducted and one member of it randomly selected. More usually, a household census is conducted before the first interview, but our experience is that respondents are often reluctant to reveal information about others in their household at the beginning of interviews. We used the following procedure. The respondent was asked to list all household members between 16 and 65 years of age. Each was assigned a number according to the sequence in which they were listed, beginning with the respondent. A random number between one and the total of eligible household members listed was assigned to the house. If this random number matched the respondent, the interviews were complete. Alternatively, if it belonged to another household member, that person was also interviewed either then or during another telephone call. Only the interview of the randomly selected member, whether the initial respondent or not, was used in the final data set.
Interview
Because of the complex nature of the branching questions (followed according to the answers given), the survey employed a computer-assisted telephone interview (CATI) based on a model used previously in more than 100 000 interviews in the USA (7). In a UK validation study (8) the CATI, compared with diagnoses made by clinicians applying IHS criteria (4) in a face-to-face semistructured interview, had a sensitivity of 91% and a specificity of 97% for migraine with or without aura (IHS categories 1.1 and 1.2).
The interview was opened with the following question: ‘In the past year have you had at least one headache, other than those caused by a head injury, a hangover, pregnancy or an illness such as a cold or the flu?’. If this was answered affirmatively, the respondent was asked how many different types of headaches he or she experienced. The remainder of the questions were directed towards the headache type identified as most bothersome (i.e. most interfered with work, study or chores) on the assumption that this was the most likely to be migraine, if any were. They began with age at onset, headache frequency and duration (unmedicated), pain intensity and disability (e.g. missed work, interference with daily activities and need for bed rest). Next they related to specific headache features: location and quality of pain, effect on headaches of physical activity, and the occurrence of nausea, vomiting, photophobia, phonophobia and visual or sensorimotor aura. Whenever a feature was reported, further questions addressed its frequency (never, rarely, less than half the time, half the time or more). When nausea, photophobia or phonophobia were reported, follow-up questions asked about the intensity of each (mild, moderate or severe). If it became clear during questions that the interviewee did not have migraine, the interview was terminated.
Lost workdays (LWD) due to migraine were estimated by the formula (9) LWD = HAFREQ × PARTDAY × %MISSED, where HAFREQ was the number of migraine attacks per year and PARTDAY was the fraction of an 8-h workday lost per attack based on the usual attack duration. When the usual duration was> 8 h, or sleep was always required, one entire workday was assumed to be lost. For shorter-lasting headaches, PARTDAY was the duration in hours divided by 8. %MISSED was the estimated percentage of attacks actually causing lost workdays, taken to be 5% for those who reported missed work ‘rarely’, 30% for missed work ‘less than half the time’ and 75% for ‘half the time or more’.
Case definition
Respondents met slightly modified IHS diagnostic criteria for migraine without aura (4) if they reported one or more headaches in the past year, five in their lifetime, and: (i) headache duration was 4–72 h; (ii) any two of the following four headache features occurred more than rarely: unilateral location; pulsatile pain; exacerbation with activity; need to miss work, or lie down, for> 2 h (reflecting a functional correlate of the IHS criterion of at least moderate headache intensity); and (iii) moderate to severe nausea and/or vomiting or both photophobia and phonophobia. A symptom feature reported as ‘rarely present’ with headache was considered as though absent. In our validation studies of the CATI, such features lacked discriminative validity for the migraine symptom complex.
Respondents met similarly modified IHS diagnostic criteria for migraine with aura (4) if they reported one or more headaches in the past year and two in their lifetimes with these characteristics: (i) association of headaches more than rarely with symptoms of visual aura (‘spots, stars, lines, flashing lights, zigzag lines, heat waves, visual loss or blurry vision’) or sensorimotor aura (‘numbness or tingling’); and (ii) any two of three criteria related to the development and duration of aura: gradual onset, duration of 3–60 min, headache onset within 60 min of aura resolution. In addition, to improve specificity, either nausea or both photophobia and phonophobia must accompany headaches more than rarely. The diagnostic validity for migraine with aura was found in a validation study of the CATI to be improved by imposing this last criterion (7).
Analysis
Gender-specific estimates of migraine prevalence were derived by race, educational level, household income and household size. Two racial categories (Caucasian and non-Caucasian), three income categories (<GBP10 000, GBP10 000–24 999, ≥ GBP25 000 per annum) and four educational categories (no exams, ‘O’ levels/GCSE, technical training/HND or ‘A’ levels, university) were defined. Crude prevalence ratios were derived as the ratio of migraine prevalence for each category relative to the prevalence in the reference category (defined as the category with most members).
Poisson regression (log-linear models) (10) was used to derive gender-specific prevalence ratios simultaneously adjusted for race, age, and education (SAS Institute Inc., Version 6.12; Cary, NC, USA). Age (age and age squared) was modelled as a continuous variable. The χ2 test (with degrees of freedom equal to the number of categories for the variable minus 1) was used to determine whether a single variable significantly improved the fit of the log-linear model to the data.
Results
A total of 7224 households were contacted by telephone over a 4-week period, but 1569 (21.7%) refused to participate before the eligibility of any member could be established. Among those who agreed, 1555 (27.5%) were not eligible (1457 because there was no age-eligible member, 26 because of language barrier, 53 because of mental or physical conditions such that they could not usefully communicate by telephone, and 19 for other reasons). Of 4100 eligible households, 4007 (97.7%) provided a complete interview. Assuming that 27.5% (i.e. 432) of the unwilling households were also ineligible, we estimated that the overall participation rate was 4007/(7224 − [1555 + 432]), or 76.5%.
The characteristics of respondents are shown in Table 1. A majority (62.9%) were female and most (92.9%) were Caucasian. Compared with the overall UK population, the survey respondents were more likely to be female and were somewhat older, a pattern often seen in surveys of this type.
Comparison of demographic characteristics among the 4007 survey participants with those of the UK national census population∗
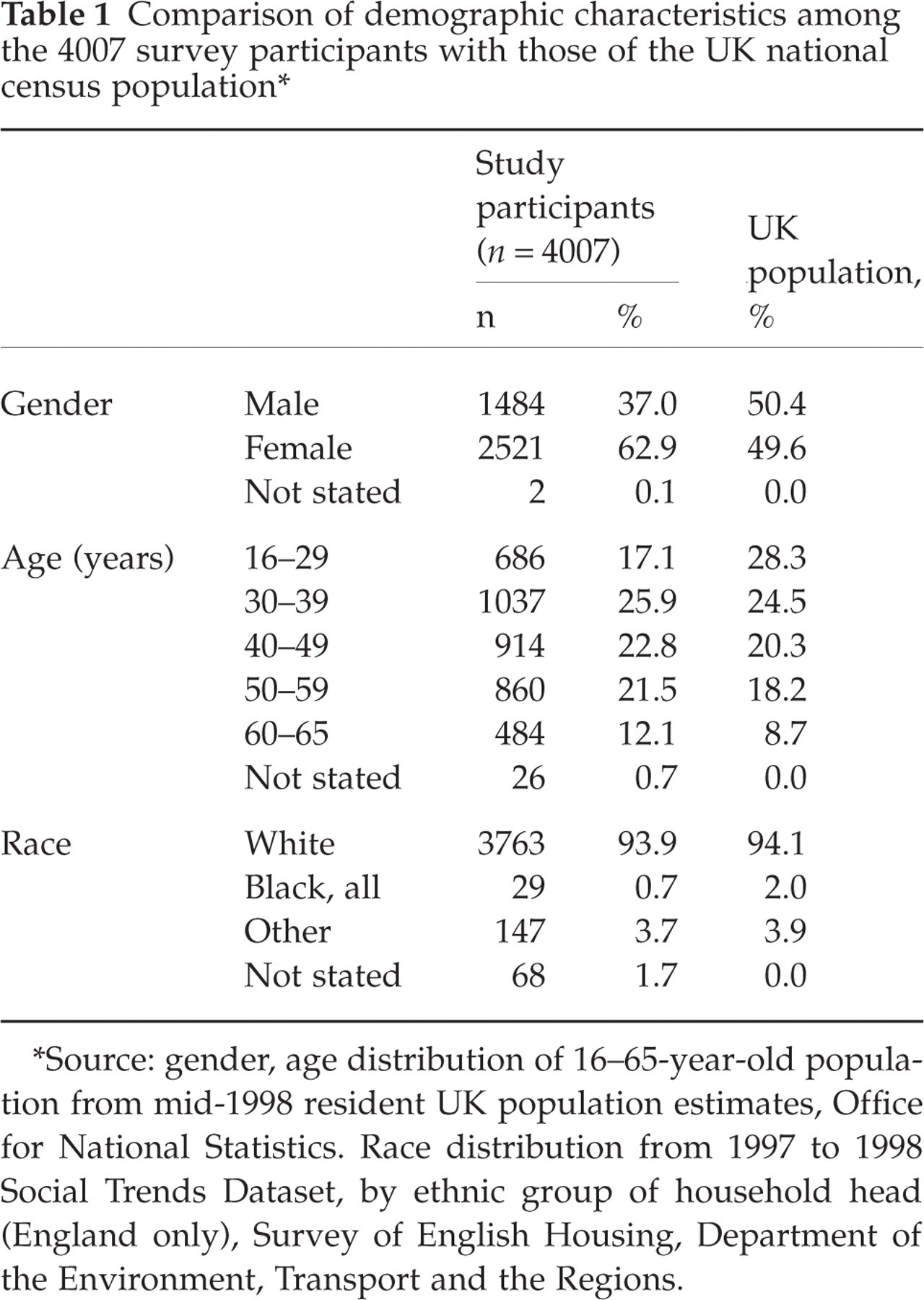
∗Source: gender, age distribution of 16–65-year-old population from mid-1998 resident UK population estimates, Office for National Statistics. Race distribution from 1997 to 1998 Social Trends Dataset, by ethnic group of household head (England only), Survey of English Housing, Department of the Environment, Transport and the Regions.
Prevalence and sociodemographic variation
Crude estimates
The overall 1-year prevalence of migraine with or without aura was 14.3% with a clear female preponderance: 7.6% in males and 18.3% in females (female : male ratio 2.4 : 1) (Tables 2a and 2b). Weighted according to the demographic characteristics of the UK population (Table 1), the prevalence was 15%. The overall 1-year prevalence of migraine with aura was 5.8% (male 2.6%, female 7.7%), and the prevalences of aura subtypes were: visual 3.3% (male 1.8%, female 4.2%), sensorimotor 1.2% (male 0.3%, female 1.7%), and visual and sensorimotor together 1.3% (male 0.4%, female 1.9%).

∗Gender was not reported by two survey respondents.
†For each characteristic, the category with most members was taken as the reference group.
‡Adjusted for age, age squared and education.
§Adjusted for age, age squared and race.
¶Adjusted for age squared, race and education.
Crude and adjusted prevalence of migraine in females (n = 2521)∗, by race, household income and household size

∗Gender was not reported by two survey respondents.
†For each characteristic, the category with most members was taken as the reference group.
‡Adjusted for age, age squared and education.
§Adjusted for age, age squared and race.
¶Adjusted for age squared, race and education.
Migraine prevalence varied with age, rising through early adult life, peaking at 30–40 years and then declining in late 40s and after 50 years in both males and females. Prevalence was lower in non-Caucasians (5.1% male, 9.3% female) than in Caucasians (7.7% male, 19.0% female), although this difference was statistically significant for females only (Tables 2a and 2b). Crude prevalence did not vary in any systematic way with educational level, income or household size (Tables 2a and 2b).
Adjusted estimates
Poisson regression was used to adjust for possible confounding when estimating prevalence by each variable. The results of these analyses are shown in Table 2a and 2b expressed as adjusted prevalence ratios. For both males and females, age (age and age squared) significantly improved the fit of the model. Figure 1 shows the predicted prevalence of migraine by gender and age using the estimated age and age squared terms, demonstrating inverted U-shaped curves.
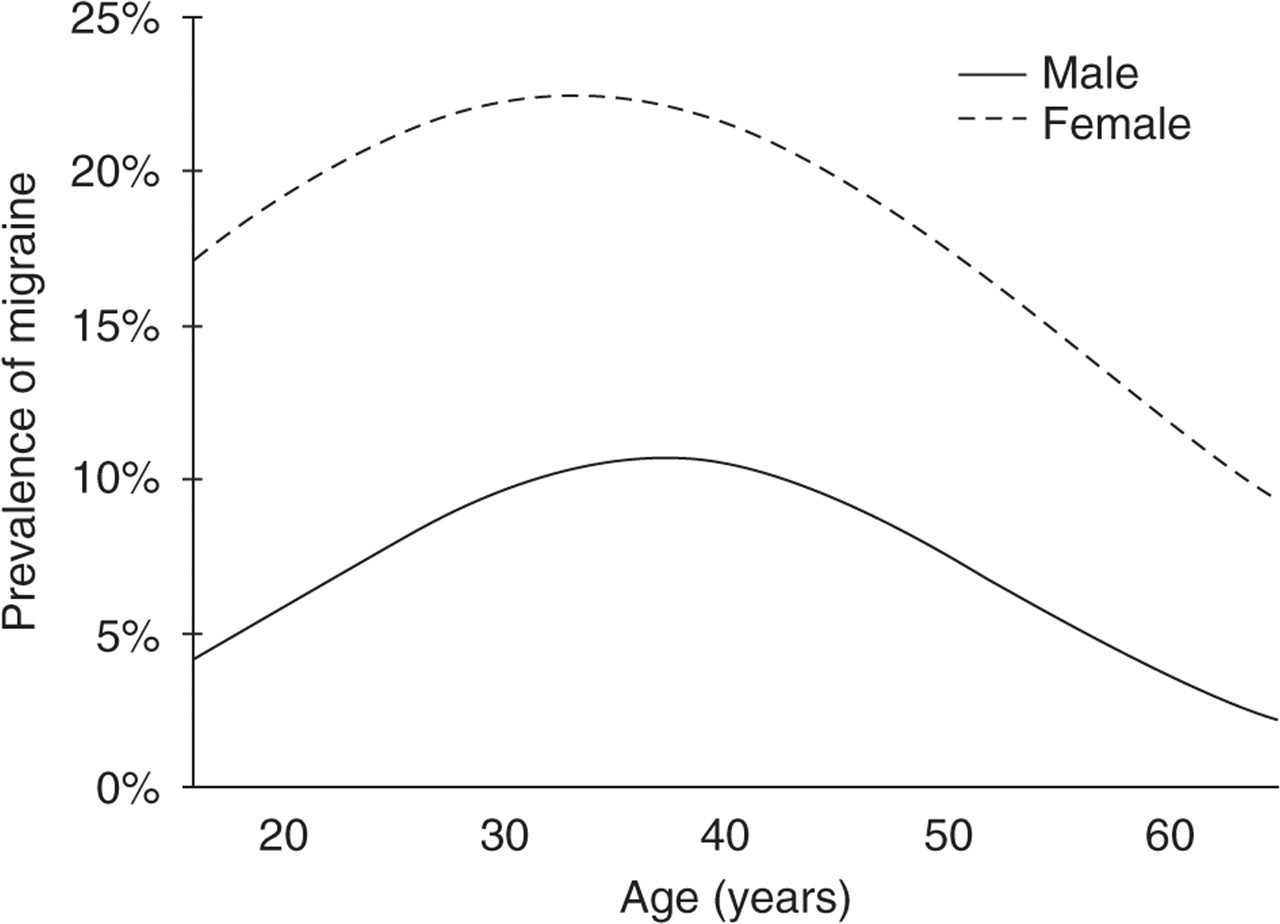
Predicted prevalence of migraine by age for males and females.
After adjusting for age and educational level, the prevalence of migraine was about 50% lower in non-Caucasians than in Caucasians for both genders, but the difference remained statistically significant only in females (P = 0.029). Among females also, race, income and household size significantly improved the fit of the model. These variables did not significantly improve the model for males, although the patterns were similar to those in females.
Headache features
Some of these are displayed in Table 3 for the 113 males and 461 females with migraine. Females were somewhat older than the males but, in both cases, half reported onset of headaches before the age of 20. The median number of attacks per year was 12, with 54% of migraineurs reporting one or more per month but 13% claiming one or more attack per week. A quarter (25%) reported high levels of pain (9–10 on a 10-point scale). The median unmedicated attack duration was 24 h.
Distribution by gender of age and selected headache characteristics among persons with migraine

Mean values were similar after adjustment for age.
∗Wilcoxon rank sum test was used to compare males and females.
†Seventy-four subjects always used medications; those providing valid responses were: males, n= 94; females, n= 384; total, n= 478.
Visual aura occurred in 32% of migraineurs and sensorimotor aura in 18%. Because these features were used in the disease definition, their high prevalences were expected. Many of the associated symptoms were reported in well over half of attacks, with prevalence generally higher in females than in males: differences were statistically significant (P < 0.05) for photophobia, phonophobia, sensorimotor aura and attack duration (36.7 h vs. 28.4 h).
Disability
Most (73%) of the migraineurs reported that headaches interfered with their daily activities more than rarely (Table 4). An estimated 5.7 workdays per year were missed by those who worked or attended school and provided this information (n = 501), but this average was heavily skewed towards the most disabled. Eliminating the worst affected 10% from the calculation resulted in a much smaller estimate of 0.9 days of missed work or school per year for every working/student migraineur. Females (34%) were more likely than males (25%) to miss time at work or school more than rarely. Almost half (>45%) of males and females who rarely or never missed work or school nevertheless required bed rest with a median duration of 2 h (Table 4).
Distribution by gender of activity limitation among persons with migraine

Discussion
We have provided estimates of adult migraine prevalence in England using minor modifications of widely accepted diagnostic criteria (4). The unmodified criteria require a full clinical encounter, and some compromise is necessary for epidemiological studies which do not require precision in every case.
Our study had some other limitations which were difficult to avoid. Because questions were asked only about the most bothersome type of headache when more than one was reported, prevalence of migraine may be underestimated but, we believe, only to a small extent. We were able to test this by reanalysing an earlier, larger study based in Baltimore County, USA (7). In that study, estimated prevalence of migraine increased by 1.3% (and of migraine with aura by 0.2%) when two headache types were considered rather than the most bothersome only. On the other hand, false positives (expected to be few because of the previously demonstrated high specificity for migraine of the diagnostic instrument) are minimized by considering only one headache type.
Subjects with coexisting migraine with aura and migraine without aura would, if they distinguished between them, have been diagnosed according to whichever they found more bothersome. There is general difficulty, experienced in clinical practice as well as epidemiological research, of formulating questions that identify aura (particularly visual aura) with high specificity. Gold standards do not exist against which to judge the performance of our questions and it is likely that the prevalence of migraine with aura – but not of migraine overall – is over-estimated. We prevented diagnosis of aura driving diagnosis of migraine by requiring nausea and/or both photophobia and phonophobia to accompany the ensuing headache more than rarely. On the other hand, because we began with the requirement of headache, those few people with migraine aura but never headache to follow were missed. Again, the underestimate is likely to be small.
Finally, we made no attempt to exclude those with secondary headaches: it is possible that some organic mimics of migraine were misdiagnosed, but these are rare in the general population (11).
Migraine is a common condition. We found an overall prevalence of migraine with or without aura, weighted according to UK population demographic characteristics, of 15% (males 7.6%, females 19.1%). Extrapolating to the entire UK population of 16–65-year-olds (projected to demographic characteristics of estimated mid-1998 resident UK population – source UK Office for National Statistics), we estimate that 5.8 million people are current sufferers from migraine. Half of these experience one or more attacks per month and all of them, in total, over 190 000 attacks every day.
These figures are consistent with recent European surveys (12–16) based on IHS diagnostic criteria and are in line with prevalence rates found in a US survey using a virtually identical interview (7). A number of British population-based studies by Waters and colleagues (17–21), conducted in the 1970s, provide interesting points of comparison. In those studies, which predated IHS diagnostic criteria, headache prevalence was reported along with the occurrence of each of three features characteristic of migraine: unilateral pain, nausea or vomiting, and warning or visual aura. Prevalence estimates of headache associated with at least two of these ranged in these studies from 20% to 37%. With a definition of migraine requiring all three, prevalence estimates were between 6% and 15%. We found a prevalence of about 6% for migraine with aura, a figure toward the high end of other published estimates (7, 16, 22–24) and probably reflecting the problems of reliance on telephone respondents’ descriptions of visual disturbance or paraesthesiae (see above). This did not affect the estimate of overall prevalence.
About half of the migraineurs reported onset before the age of 20. This figure may be an underestimate, as people tend to recall past events as happening more recently than was actually so (25). The finding highlights the importance of the condition in young people, and therefore of its recognition.
Prevalence of migraine headache in non-Caucasians (black, Asian, Bangladeshi, Chinese and other races) was about half that in Caucasians in both males and females and for both the crude and adjusted prevalence values. Although numbers were very small, this difference was statistically significant for females. These results are consistent with those from US surveys of multiracial populations (7, 26) and those from a number of African and Asian studies, which have generally (but not universally) shown relatively low prevalences of migraine and other headache (2, 27–36). Whether environmental factors, genetic differences or cultural diversity in the reporting of pain explain this apparent difference in headache susceptibility is unknown. It remains an area of future research.
There was no statistically significant association of migraine prevalence with educational level or income; trends towards lower prevalence with higher education level or income were not consistent. Several US surveys have found migraine to be inversely associated with income and/or educational level (7, 22, 26, 37), although this has not generally been observed elsewhere (12, 16, 38, 39).
The great majority of migraineurs reported some interference with their daily activities because of their migraine headaches. Other population-based estimates of lost work due to migraine have been substantial, ranging from 2 to 7 days per year (6, 9, 40–42). In our survey, although many claimed never or rarely to miss work or school for this reason, the estimated average of lost days, about 5.7 per year, was in this range but only because of a very disabled small minority. If these are discounted, and assuming 235 days are worked per year, the probability of an individual migraine sufferer being off work on any workday because of migraine is 0.004. In a workforce of 30 million of whom 15% have migraine, including those most affected, over 100 000 will be absent every day, contributing to 25 million lost work- or schooldays every year. This survey did not measure reduced effectiveness while at work with migraine, which has been shown to have equal or greater impact on work productivity than actual missed days (3, 9, 40, 41).
Footnotes
Acknowledgements
The authors gratefully acknowledge Pfizer, Inc. for funding this research.