
Abstract
The careful monitoring of the trigger factors of headache could be an important step in treatment, because their avoidance may lessen the frequency and severity of attacks. Furthermore, they may provide a clue to the aetiology of headache. The aim of the present study was to estimate the prevalence of tension-type headache (TTH) and to establish the frequency of precipitating factors in subjects with migraine and TTH in the adult population of Bakar, County of the Coast and Gorski Kotar, Croatia. Another important purpose of the study was to examine the relationship of the precipitating factors with migraine and TTH, and with migraine subtypes: migraine with aura (MA) and migraine without aura (MO). We performed a population-based survey using a ‘face-to-face door-to-door’ interview method. The surveyed population consisted of 5173 residents aged between 15 and 65 years. The 3794 participants (73.3%) were screened for headache history according to the International Headache Society (IHS) criteria. Headache screen-positive responders, 2475 (65.2%), were interviewed by trained medical students with a structured detailed interview focused on the precipitating factors. The following precipitating factors in lifetime migraineurs and tension-type headachers have been assessed: stress, sleep disturbances, eating habits, menstrual cycle, oral contraceptives, food items, afferent stimulation, changes in weather conditions and temperature, frequent travelling and physical activity. A total of 720 lifetime migraineurs and 1319 tension-type headachers have been identified. The most common precipitants for both migraine and TTH were stress and frequent travelling. Stress (odds ratio (OR) 1.4, 95% confidence interval (CI) 1.17, 1.69) was associated with migraine, whereas physical activity (OR 0.72, 95% CI 0.59, 0.87) was related to TTH. Considering MA and MO, frequent travelling (OR 2.2, 95% CI 1.59, 2.99), food items (OR 2.2, 95% CI 1.35, 3.51) and changes in weather conditions and temperature (OR 1.75, 95% CI 1.27, 2.41) exhibited a significant positive association with MA. The present study demonstrated that precipitant-dependent attacks are frequent among both migraineurs and tensiontype headachers. Lifetime migraineurs experienced headache attacks preceded by triggering factors more frequently than tension-type headachers. MA was more frequently associated with precipitating factors than MO. We suggest that some triggering factors may contribute to the higher occurrence of precipitant-dependent headache attacks in susceptible individuals.
Introduction
Migraine and tension-type headache (TTH) are the most common headaches in the general population, and the overall socioeconomic impact of these diseases on the community is considerable (1–5). The introduction of the International Headache Society (IHS) criteria (6) was a major step toward the standardization of the diagnosis of headaches and the differentiation between migraine and TTH. However, the debate regarding the interrelationship between migraine and TTH in the general population is ongoing (1, 3–5, 7, 8).
Precipitants (also called trigger factors or promotors) are factors which alone or in combination with other exogenous or endogenous exposures induce headache attacks in susceptible individuals (3). Precipitating factors precede the headache attack by a short time interval and have to be distinguished from risk factors for the disease and from initiators, which include constitutional factors present at birth or long before the initial onset of the attack (9). A large number of suspected precipitants for migraine and TTH have been reported, including mental and endogenous factors, absorbed factors and others (Table 1) (10). The extensive literature on the precipitants establish that there is little evidence that a specific precipitating factor can be linked definitely with the onset of migraine and TTH attacks (10–17). Moreover, the published data suggest that precipitants of migraine with aura (MA) and migraine without aura (MO) are occasional triggers (3, 18, 19). Thus, precipitants induce headache attacks in susceptible subjects and are not regarded as causal agents. This suggests that precipitants are not absolutely determinant, since the presence of a trigger factor does not always cause an attack in the same individual. Therefore, it could be hypothesized that the presence of a precipitant is a necessary but not sufficent factor to initiate an attack, and that a multifactorial trigger mechanism may play a fundamental role in the development of specific attacks.
Precipitanting factors of migraine and tension-type headache (modified from Peatfield and Olesen (10)

The careful monitoring of trigger factors could be an important step in treatment, because their avoidance may lessen the frequency and severity of headache attacks. Furthermore, they may provide a clue to the aetiology of headache. The aim of the present study was to estimate the prevalence of TTH and to investigate the frequency and the association of precipitating risk factors with migraine, its subtypes and TTH in a population-based ‘face-to-face, door-to-door’ epidemiological survey among Croatian adults, in Bakar, County of the Coast and Gorski Kotar.
Materials and methods
The study population consisted of all residents in Bakar, County of the Coast and Gorski Kotar, Croatia, aged between 15 and 65 years on 31 December 1998 (5173 residents). After the approval of the Bakar Municipal Council had been obtained, the addresses and the telephone numbers of all potential resident candidates for the survey were obtained from the local Statistical Centre. They were contacted by telephone or visit and those willing to participate were interviewed at home. During 1999, among the 5173 residents aged between 15 and 65 years, a total of 3794 individuals (73.3%) participated in the study. There was no significant difference among participants and non-participants regarding age and gender. Therefore, the participants have been considered representative of the total surveyed population sample. The reasons for non-participation were: unlisted or incorrect phone number or inaccurate address (901 residents, 65.3%) and refusal to participate in the study (479 residents, 34.7%). Among the participants, a total of 2475 (65.2%) screen-positive headache responders were identified.
A ‘face-to-face, door-to-door’ structured interview, developed by two senior neurologists (K.W. and D.S.-G.) of the Neurological Clinic of the University of Rijeka, Croatia, specializing in headache diagnosis and therapy, was administered to each participant in the study (20). The interview was developed in order to screen the population for the presence of migraine and TTH on the basis of the IHS criteria and was structured into three different sets of questions. The first set regarded the sociodemographic, psychosocial, medical and headache history data, and the results of these analyses are reported elsewhere (20). On the basis of these questions, screen-positive headache responders were defined as those who had ever or in the last 12 months had a severe headache (excluding those due to hangover or sinus infection) and the pain was 5 or higher on a 10-point scale, or where there was a history of severe headache in the last 12 months and the pain was rated between 1 and 4 and one of 10 visual aura symptoms was experienced (Stewart et al.) (21). The second set of questions aimed to classify the screen-positive headache responders as affected by migraine and/or TTH. The lifetime migraine prevalence was estimated according to the IHS criteria on the basis of patients who had ever had migraine. At least two different attacks of MA or at least five attacks of MO were the criteria. The lifetime prevalence of MA, MO and the 1-year prevalence of MA, MO and migraine both with and without aura were obtained. The migraine group also included subjects with coexisting TTH. It was decided not to use a pure migraine group, since the numbers for the analyses would be too small and non-representative of the whole migraine clinical sample. The diagnostic criteria of IHS (code 2.1, 2.2, 2.3) were used to assess the lifetime prevalence of TTH. The TTH group included subjects who presented at least 10 previous headache episodes fulfilling the IHS lifetime criteria. The TTH group also included subjects with coexisting migrainous headaches. The other headache sufferers were classified under the item ‘other type of headache’. Four hundred and thirty-six (17.6%) screen-positive headache responders were not subclassified. They suffered from other types of headache, but we did not sistematically assess their headache status according to the IHS criteria.
The third set of questions concerned the precipitating factors in lifetime migraineurs and tension-type headachers. Information about common precipitating factors was collected during the structured interview. The interviewee was asked to add any other precipitant they experienced. In order to establish whether the headache attacks had been precipitant-dependent, two or more lifetime episodes induced by the same trigger factor were requested. The precipitant factors questionnaire consisted of four groups of risk factors. The mental factors included stress, sleep disturbances, and eating habits; the endogenous factors examined the effect of hormonal changes (menstrual cycle and use of oral contraceptives); the absorbed factors concerned various food items (chocolate, cheese, alcoholic drinks, fried fatty foods, vegetables and coffee); other risk factors included afferent stimulation (flickering light and noise), changes in weather conditions and temperature, frequent travelling and physical activity. Several risk factors contained a range of different variables related to the same precipitant. For the purpose of analysis and in order to classify the migraineurs and tension-type headachers as precipitant-dependent or non-precipitant-dependent, the association of at least one of the examined variables with the onset of headache attacks was requested.
The interviews were performed and the questionnaires were filled in by 12 medical students after an appropriate period of training conducted by investigators expert in headache, and when an adequate interobserver agreement was achieved among the team of interviewers. At the end of the training period, validation of the screening procedure was performed in the interviewers blinded to the clinical diagnosis of 200 patients who were followed routinely by the Neurological Clinic of the University of Rijeka. The inter- and intra-observer agreement was 0.85 (range 0.65–0.92) and 0.84 (range 0.68–0.88), respectively. The sensitivity of the case finding procedure was 0.92 (range 0.58–0.99). The final diagnosis of MA or MO and TTH was made by senior neurologists (K.W., D.S.-G., A.J. and M.B.). All participants signed a general informed consent before study entry and the study was approved by the local Ethical Committee.
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS Inc., Version 10.0, Chicago, IL, USA). We used the χ2 test and the analysis of variance, as appropriate, to determine whether the difference between two or more frequencies was significant. The lifetime prevalence of migraine, MA, MO and TTH was calculated. Ninety-five percent confidence intervals (95% CI) were calculated using a binomial approximation of the Poisson distribution by the method suggested by Schoenberg (22). The odds ratio (OR) associated with the precipitating risk factors, the 95% CI and the P-value were calculated by χ2 statistic (crosstabs procedure). Various multiple logistic regression models have been tested to identify whether any precipitating risk factor was associated with a higher risk of migraine and TTH episodes. The analysis was performed for migraine and TTH, and MA and MO. Demographic data were obtained from the Statistics Centre of Bakar, County of the Coast and Gorski Kotar, Croatia. The minimum significance level for entry and for staying in the equation was 0.05. All P-values were based on two-tailed tests.
Results
Prevalence of headaches
A total of 720 lifetime migraineurs and 1319 lifetime tension-type headachers were identified. The lifetime prevalence of migraine was 22.9% (95% CI 20.9, 25.1) in women, 14.8% (95% CI 13.1, 16.8) in men and 19% (95% CI 17.6, 20.5) in both genders. Detailed age- and sex-specific lifetime prevalence data of migraine, MA and MO are reported elsewhere (20). The lifetime prevalence of TTH was 37.1% (95% CI 34.4, 40) in women, 32.3% (95% CI 29.8, 35) in men and 34.8% (95% CI 32.6, 37) in both genders. Among women the highest age-specific prevalence was in the age groups 15–19 and 50–59 years (72.4% and 51.5%, respectively). Among men the lifetime prevalence peak was in the age groups 15–19 and 40–49 years (61.5% and 37%, respectively).
Frequency and lifetime risk of precipitant-dependent attacks in patients with migraine and TTH
The frequencies and the ORs of the precipitating factors in migraine and TTH are given in Table 2. Among migraineurs, the most common precipitating factor was stress (57.8%), followed by frequent travelling (54.6%), menstrual cycle (49.4%), changes in weather conditions and temperature (49%), and sleep disturbance (40.1%). Among tension-type headachers the most important precipitant was frequent travelling (52.5%), followed by stress (49.4%), menstrual cycle (45.7%), changes in weather conditions and temperature (44.7%), and physical activity (36.7%). In total, 555 (77%) migraineurs and 725 (54.9%) tension-type headachers presented at least one precipitating factor (P = 0.003). Comparing migraine and TTH, the analysis showed that stress (OR 1.4, 95% CI 1.17, 1.69; P = 0.002) was associated with migraine, whereas changes in weather conditions and temperature (OR 1.19, 95% CI 0.99, 1.43; P = 0.063), sleep disturbances (OR 1.19, 95% CI 0.99, 1.44; P = 0.067) and afferent stimulation (OR 1.2, 95% CI 0.99, 1.44; P = 0.069) showed only a trend towards association. The only precipitant which was associated with TTH was physical activity (OR 0.72, 95% CI 0.59, 0.87; P = 0.02). The frequency of precipitants did not differ in men and women either in migraine or in TTH, obviously excepting menstruation and oral contraceptives. In multiple logistic regression analysis, migraine and TTH were used as the dependent variables and the presence of precipitating factors as the independent ones in various models. Stress (R = 0.65, P < 0.0001) was the only precipitant which was independently associated with migraine.
Frequencies of lifetime precipitant-dependent attacks in migraine and tension-type headache and odds ratios (OR) associated with each precipitating factor
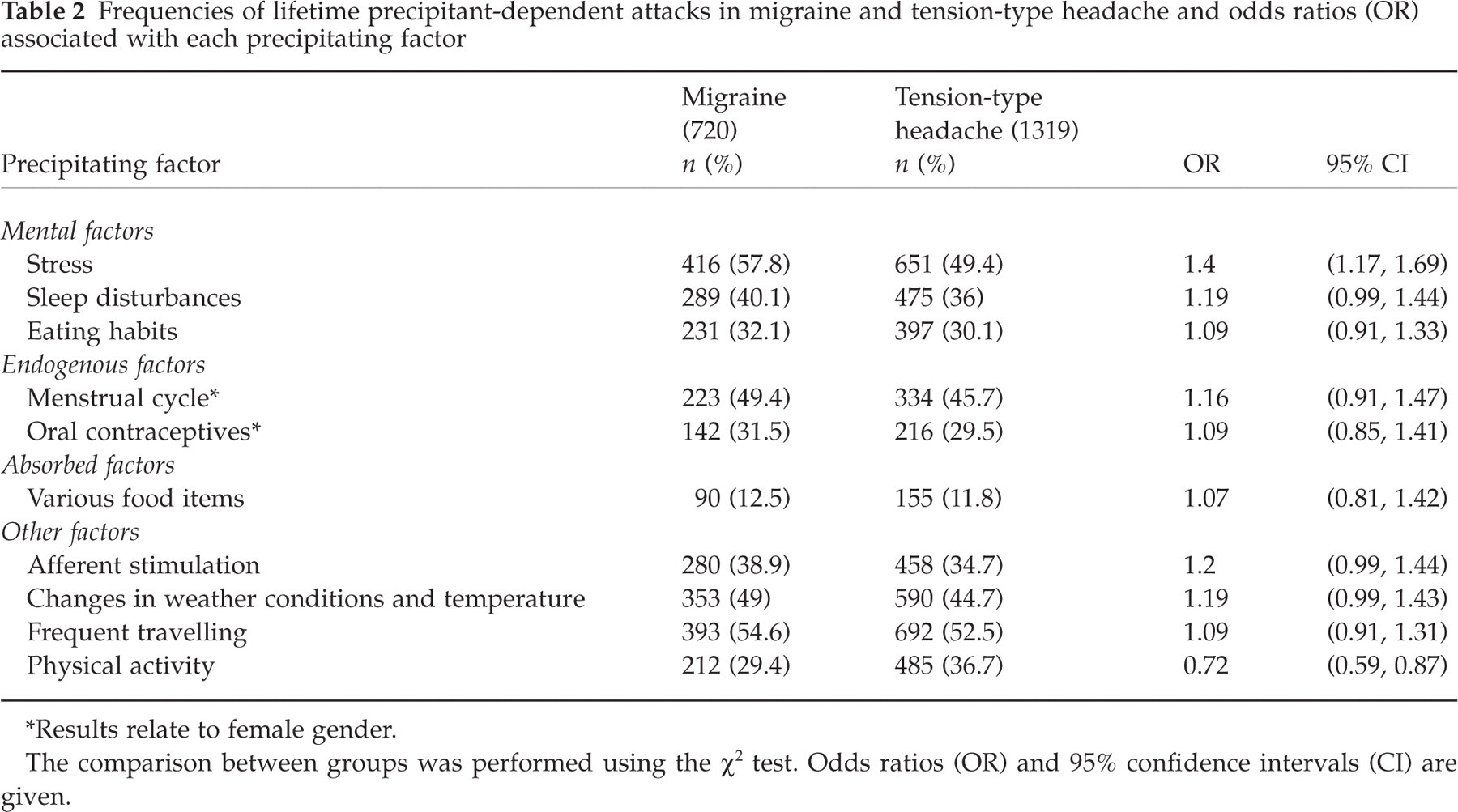
∗Results relate to female gender.
The comparison between groups was performed using the χ∗ test. Odds ratios (OR) and 95% confidence intervals (CI) are given.
Frequency and lifetime risk of precipitant-dependent attacks in MA and MO
The frequencies and the ORs of the precipitating factors in MA and MO are shown in Table 3. In patients affected by MA a higher frequency of the following precipitating factors was observed: frequent travelling (66.7%), stress (60.9%), menstrual cycle (51.1%) and changes in weather conditions and temperature (39.9%). Among subjects with MO the most frequent precipitants were: stress (56.1%), menstrual cycle (48.6%), and frequent travelling (47.8%). Among subjects with MA, men mentioned sleep disturbance as a trigger factor more frequently than women (P = 0.03). No other sex difference in the frequency of precipitants was observed, either for MA or for MO (excepting menstruation and oral contraceptives). In total, at least one precipitating factor was present in 222 (86%) subjects with MA and in 333 (72%) subjects with MO (P = 0.04). Comparing MA and MO, the analysis demonstrated that frequent travelling (OR 2.2, 95% CI 1.59, 2.99; P < 0.0001), food items (OR 2.2, 95% CI 1.35, 3.51; P < 0.0001) and changes in weather conditions and temperature (OR 1.75, 95% CI 1.27, 2.41; P = 0.0005) exhibited a significant positive association with MA.
Frequencies of lifetime precipitant-dependent attacks in migraine with aura (MA) and migraine without aura (MO) and odds ratios (OR) associated with each precipitating factor

∗Results relate to female gender.
The comparison between groups was performed using the χ2 test. Odds ratios (OR) and 95% confidence intervals (CI) are shown.
Multiple logistic regression analysis showed that MA was independently associated with frequent travelling (R = 0.72, P < 0.0001) and food items (R = 0.52, P = 0.0001).
Discussion
This was the first epidemiological study of migraine and TTH in Croatia in which the operational diagnostic IHS criteria were used and the precipitating risk factors were investigated.
In the present study we employed a ‘face-to-face, door-to-door’ interview method in the whole clinical sample, including the screen-negative headache responders. This method of data collection should be more sensitive for migraine and TTH case definition than telephone interview or self-administered mail questionnaire. A face-to-face clinical interview remains the gold standard for migraine and TTH diagnosis in absence of any neuroradiological or biological markers. In the present study we performed, before the beginning of the study, a 1-month period of training conducted by study physicians expert in headache involving 12 medical students. In addition, during the study data collection, senior neurologists performed monthly consultation meetings with the interviewers in order to establish a final diagnosis of migraine and its subtypes and TTH. Such an approach minimizes potential diagnosis bias and contributes to obtaining more reliable information on the prevalence of migraine and TTH (20).
The overall lifetime prevalence of TTH in our study was high, 34.8% in both genders. This rate is higher than lifetime prevalence rates reported in some studies (23, 24), but lower than that reported in other population studies (1, 25). The lifetime prevalence of TTH is higher than the 1-year prevalence. Variation in prevalence estimates may be due to different study methodologies, including case definition as well as demographic factors. The prevalence of chronic tension-type headache (CTTH) is markedly lower than that of episodic tension-type headache (ETTH). In the present study we estimated the lifetime prevalence of overall TTH according to the IHS diagnostic criteria (code 2.1, 2.2, 2.3). Therefore, our lifetime prevalence rates of TTH could not be compared with the 1-year CTTH and ETTH prevalence rates reported by other authors (25–29). The prevalence was slightly higher among women (37.1%) than men (32.3%). Most studies reported that the female preponderance occurs irrespective of age, race and educational level (1, 25–29). The prevalence of TTH may vary by age, although results are inconsistent across studies. Several studies suggest that prevalence increases from adolescence to about age 40 years and declines thereafter, with a peak in the 30s and 40s (1, 25–30). Our age-specific lifetime prevalence rates were similar to the rates reported in those studies, showing a bimodal pattern with a peak in the age groups 15–19 and 40–49 years (65% and 38.1%, respectively). The exact cause of the peak prevalence in the younger age group both for migraine and TTH in this study is not clear. One of the possible explanations could be a high occurrence of stress syndrome among high-school students preparing for college entrance, as reported by other authors (31).
Some previous studies (14, 32) did not distinguish between precipitating factors of migraine, its subtypes and TTH, but reported precipitants of headache in general. A population-based survey of headache precipitants may be difficult to interpret, since these factors may be dependent on the consulting status of the subjects in examination. Precipitants are most often studied simply by examining patient reports. There are several aspects of our precipitant collecting procedure that need to be considered. Particular attention was focused on distinguishing the precipitating factors from the typical premonitory symptoms mimicking several trigger factors. Previous studies concerning precipitating factors (10–17) did not define specifically the number of lifetime precipitant-dependent headache episodes requested to classify a subject as precipitant-dependent. In the present study, one of the inclusion criteria to establish whether the headache attacks were precipitant-dependent was at least two lifetime headache episodes induced by the same trigger factor. This decision was based on the belief that in such a way our collection procedure would be more accurate and sensitive in identifying the precipitant-dependent subjects, although no systematic effort was made to assess the sensitivity and accuracy of such an approach.
More than half of subjects suffering from migraine and TTH experienced lifetime precipitant-dependent headache attacks in this study. The most common provoking factors, both for migraine and TTH, were, in agreement with previous studies (13–17, 32, 33), mental tension risk factors and frequent travelling. Menstrual cycle, changes in weather conditions and temperature were identified also as frequent precipitants among migraineurs and tension-type headachers, as previously reported in the literature (12–17, 32–34). In the present study we did not find any significant association of a particular food with migraine and TTH, in agreement with recently published Danish and North American population-based studies (15–17), although it is well known that some kinds of food and alcohol may precipitate individual headache episodes in migraine and TTH.
In the present study we searched for the best predictors of lifetime precipitant-dependent headache attacks. The analysis demonstrated that only stress was independently associated with migraine. Our findings confirm the results of several previous studies (15–17, 32, 33). A number of reports (13, 15–17) showed a positive association between physical activity and TTH. In the present study, also, the only precipitant associated with TTH was physical activity. This observation suggests that muscular factors may play a role in the genesis of TTH, but are not of decisive importance in migraine.
Population-based studies describing precipitants of MA and MO are rare (3). Most reports which investigated the precipitating factors for MA and MO were based on case-control studies performed on hospital-based population or out-patient series. In the present study, the most frequent precipitants, both for MA and MO, were stress and frequent travelling. In particular, frequent travelling was the most common precipitant in subjects affected by MA, and it was independently associated with this type of migraine (P < 0.0001).
The role that food allergy plays in migraine is undetermined. The most common cause of what patients call ‘food allergy’ is food aversion, a psychological response to the food itself (11). Most food reactions are chemically mediated by, for example, lactose (35), nitrites (‘hot dog headache’) (36), monosodium glutamate (‘Chinese restaurant syndrome’) (37), red wine (38). Most migraineurs in the present study show a low occurence of headache attacks induced by different food factors. However, subjects affected by MA presented a higher susceptibility to different food triggers when compared with MO subjects, in particular to red wine (P < 0.0001). It is not completely clear which are the mechanisms that heighten the risk of individual attacks associated with a particular food (11).
The occurrence of headache attacks, induced by the use of oral contraceptives, was higher in subjects affected by MO, although the difference was not statisticaly significant. It has been reported previously that the relationship between female hormones and MO was clearly stronger than with MA (39). Our data confim this observation. The mechanism through which the hormones act in migraine is not understood, although it has been suggested that fluid and salt retention, platelet aggregation or change in serotonin and prostaglandin levels may play a role (40). Recently, it has been reported that children with MA show a higher occurrence of headache episodes induced by afferent stimulation than tension-type headachers (19). To the best of our knowledge, there are no data on the relationship between MA and MO headache attacks and afferent stimulation triggering in population-based studies. Our data failed to detect a difference between MA and MO with respect to this particular precipitant and suggest that different mechanisms could be involved in the explanation of current findings (5, 41).
The present study gives some support to the theory that migraine and TTH may be separate clinical entities, although they may coexist and interrelate (3, 7, 8), and also reinforces the opinion (39) that MA and MO are distinct subforms of the same disorder. Based on the results of our study, it seems clear that a specific precipitant factor could not be linked definitely with migraine and TTH attacks, although mental tension risk factors and frequent travelling are probably the most common cause of precipitant-dependent headache attacks in susceptible subjects. The high occurrence of precipitant-dependent headache episodes induced by a variety of precipitants in our study confirms the hypothesis that a multifactorial trigger mechanism may play an important role in the development of individual attacks.
In conclusion, the present study demonstrates that precipitant-dependent attacks are frequent among both migraineurs and tension-type headachers. Lifetime migraineurs experienced headache attacks preceded by triggering factors more frequently than tension-type headachers. MA was more frequently associated than MO with precipitating risk factors. We suggest that some triggering factors may contribute to the higher occurrence of precipitant-dependent headache attacks in susceptible individuals.
Footnotes
Acknowledgements
This work was supported by a research fund of GlaxoWellcome Croatia. The authors thank the medical students of the University of Rijeka, Croatia, who performed the ‘face-to-face, door-to-door’ interviews.