
Abstract
Increased muscle tenderness is the most prominent finding in patients with tension-type headache, and it has recently been shown that muscle blood flow is diminished in response to static exercise in tender points in these patients. Although tenderness has been ascribed to local inflammation and release of inflammatory mediators, the interstitial concentration of inflammatory mediators has not previously been studied in tender muscles of patients with tension-type headache. The aim of the present study was to investigate in vivo concentrations of prostaglandin E2 (PGE2), adenosine 5'-triphosphate (ATP), glutamate, bradykinin and other metabolites in a tender point of patients with chronic tension-type headache, in the resting state as well as in response to static exercise, and to compare findings with measurements in a matched non-tender point of healthy controls. We recruited 16 patients with chronic tension-type headache and 17 healthy control subjects. Two microdialysis catheters were inserted into the trapezius muscle and dialysates were collected at rest, 15 and 30 min after start of static exercise (10% of maximal force) and 15 and 30 min after end of exercise. All samples were coded and analysed blindly. There was no difference in resting concentration of any inflammatory mediators or metabolites between tender patients and non-tender controls (P > 0.05). We also found no difference in change in interstitial concentration of ATP, PGE2, glutamate, glucose, pyruvate and urea from baseline to exercise and post-exercise periods between patients and controls (P > 0.05). The present study provides in vivo evidence of normal interstitial levels of inflammatory mediators and metabolites in tender trapezius muscle in patients with chronic tension-type headache during both rest and static exercise. Thus, our data suggest that tender points in these patients are not sites of ongoing inflammation.
Introduction
In spite of considerable progress in tension-type headache research in recent years (1), the origin of pain in this prevalent primary headache is unknown. Findings of increased myofascial tenderness (2–4) and muscle hardness (5, 6) in patients with chronic tension-type headache suggest that tender points in pericranial muscles might be the sites of primary hyperalgesia (1). Thus, painful impulses from these sites may be referred to the head and perceived as tension-type headache (7). Recently, we reported a decreased blood flow in response to static exercise in a tender point in patients with chronic tension-type headache (8). It is, however, unclear whether altered blood flow is due to local inflammation or to centrally mediated abnormal vascular control. Tender points might be associated with increased concentrations of pain-stimulating substances and sensitized muscle nerve endings (9). In this case local ongoing inflammation or altered metabolism may result in increased myofascial tenderness and local and referred pain (10). It is well established that inflammatory mediators such as prostaglandin E2 (PGE2), bradykinin, adenosine 5′-triphosphate (ATP) and glutamate may be released from or around afferent nerve fibres and then activate or sensitize peripheral nociceptors (11). In particular, it has been shown that a low-intensity static contraction may increase the intramuscular concentration of PGE2 in ischaemic muscle (12) and that PGE2 may sensitize muscle nerve endings during static contraction (13). Thus, tender points might be sites of inflammation and thereby sites of primary hyperalgesia. Moreover, it is possible that release of inflammatory mediators is even more pronounced during muscle work. Therefore, assessment of intramuscular concentrations of inflammatory mediators in the tender points before, during and after exercise is warranted to elucidate the possible role of inflammation in the mechanisms underlying increased myofascial tenderness in tension-type headache.
To test this hypothesis we aimed to investigate in vivo concentrations of PGE2, ATP and glutamate and various other metabolites in tender muscle at rest and during static exercise in patients with chronic tension-type headache and in healthy controls. In addition, we examined in vivo concentrations of bradykinin and potassium in tender muscle of patients during rest.
Methods
Subjects
We recruited 16 patients (Table 1) with a diagnosis of chronic tension-type headache according to the criteria of the International Headache Society (headache frequency ≥ 15 days per month for ≥ 6 months) (14) from the out-patient headache clinic at Glostrup University Hospital. All patients completed a diagnostic headache diary (15) during a 4-week run-in period to confirm the diagnosis. At screening, we undertook a full physical and neurological examination. Body weight and height of all subjects were collected in order to calculate body mass index (BMI) at the end of the study. Patients were included if they had increased tenderness of the trapezius muscle to manual palpation (scored ≥ 2 on a 4-point (0–3) scale). Exclusion criteria were: a history of migraine or any other type of primary headache; use of any kind of daily medication including prophylactic headache therapy but not oral contraceptives; excessive alcohol use; serious somatic or psychiatric disorders including depression (Hamilton Depression Score ≥ 17) (16). Seventeen healthy volunteers served as controls (Table 1). They were included if they had no more than mild tenderness of trapezius muscle to manual palpation (scored ≤ 1 on a 4-point (0–3) scale). They never had migraine and had less than 12 days per year with tension-type headache. The study was approved by the Scientific-Ethical Committee of the County of Copenhagen, and was undertaken in accordance with the Helsinki Declaration of 1975, as revised in 1983. All subjects gave informed consent to participate in the study.
Clinical data for headache patients and healthy controls

Data are mean (range).
Experimental design
All subjects reported to the laboratory at 08.00 h following an overnight fast (12 h) including abstinence from tobacco, coffee and tea. All procedures were performed in a quiet room at a temperature of 22–24°C. The patients were examined during a typical day of tension-type headache, i.e. they had pain characteristic of tension-type headache with no more than one associated symptom (14). Headache intensity was measured on a visual analogue scale (VAS) (0–100 mm: 0, no pain; 100, worst imaginable pain). Subjects were not allowed to take analgesics 24 h prior to examination or to do recreational exercise at least 48 h prior to examination. After a brief rehearsal session, we recorded local tenderness and then the maximal voluntary force during isometric contraction of trapezius muscle. The subjects were seated upright in a dental chair with hanging arms and legs. Adjustable force transducers with a contact area of 10 × 10 cm (Bisco Vaegte A/S, Farum, Denmark) were placed over the shoulders and connected to a force monitor. On command, the subjects were encouraged to elevate both shoulders with maximal force for 3 s. The maximal voluntary isometric contraction force of the trapezius muscle was defined as the average of three recordings. Fifteen minutes after the test for maximal voluntary isometric contraction, two microdialysis catheters were inserted in parallel approx. 1.5 cm apart into the trapezius muscle at a standard anatomical point on the non-dominant side. During the insertion of catheters we used ultrasound imaging (Acuson XP10 ultrasound unit equipped with a 7-MHz linear transducer; Acuson, Mountain View, CA, USA) to ensure that the membrane part of the catheters was placed in the muscle in a direction parallel to the muscle fibres. Subsequently, perfusion of the catheters was started and they were allowed to stabilize for 60 min. During the next 60 min baseline dialysate was collected. During this period the subjects were sitting in a dental chair with a headrest and were allowed to watch video film or listen to music. After the resting period the subjects performed a voluntary isometric contraction of the trapezius muscle at 10% of the maximal voluntary isometric force for 30 min. Visual inspection of the monitor by the investigator and the subjects ensured that the desired exercise intensity was performed within ± 200 g variation (corresponding to about 4% of intended force development). Dialysates were collected 15 and 30 min after start of exercise and 15 and 30 min after stop of exercise. Because of small amount of dialysate during exercise and post-exercise sampling periods, bradykinin and potassium concentrations were measured only during stabilization and resting periods. During the post-exercise period, the subjects were seated in the same position as during rest. Blood flow data from the study have previously been reported (8).
Microdialysis
Two microdialysis catheters (CMA/60; CMA Microdialysis, Stockholm, Sweden) with a membrane length of 30 mm (diameter of 0.6 mm) and a molecular weight cut-off of 20 kDa were used to estimate the nutritive skeletal muscle blood flow and the interstitial lactate concentration. The perfusate (the fluid going into the catheter) runs slowly along the dialysis membrane, and the concentration of substances in the dialysate (the fluid coming out of the probe) mirrors the concentration of substances in the interstitial fluid. The catheters were perfused with Ringer acetate containing 3 m
Analyses
Dialysate concentrations of PGE2 (NENTM Life Science Products PGE2[125I] RIA Kit) and bradykinin (RIK-7051 Bradykinin; Peninsula Laboratories, Inc., San Carlos) were determined by radioimmunoassay. The ATP monitoring kit (Labsystems, Oy, Finland) was used to measure dialysate concentration of ATP by bioluminescence technique. Potassium concentrations were measured by flame photometry. Metabolites (glutamate, glucose, pyruvate and urea) were analysed on a CMA 600 microdialysis analyser (CMA Microdialysis).
Local tenderness
Local tenderness was defined as pressure-induced pain at a standard anatomical point on the trapezius muscle on the non-dominant side. Thus, local tenderness was measured at the same anatomical point where two microdialysis catheters were later inserted (the site of dialysate sampling). Using a palpometer (17), we applied a standardized pressure (160 U) on this point and the subjects scored pressure-induced pain on VAS.
Statistical analysis
Results are presented as mean ± SEM. A two-way repeated measures analysis of variance (
Results
All subjects completed the study. Overall, 2772 samples were collected. Due to technical problems a total of 34 samples were missing in patients and 23 samples in controls. The missing samples were equally distributed between various variables.
There was no difference between patients and controls in either BMI (P = 0.85) or in maximal voluntary force (P = 0.37) (Table 1). Before the insertion of catheters, local tenderness at the standardized point was significantly higher in patients, 34 ± 5, than in controls, 3 ± 1 (P = 0.0001). On the experiment day the mean headache intensity in patients was 32 ± 4 mm on VAS.
Dialysate concentration of inflammatory mediators and metabolites
We found no difference in ATP concentrations between stabilization period (0–60 min) and baseline (60–120 min) in either patients (P = 0.77) or controls (P = 0.92) (Fig. 1). However, interstitial concentration of PGE2 (P = 0.0001), glutamate (P = 0.0001) and bradykinin (P = 0.014) decreased significantly at baseline compared with the stabilization period in patients (Fig. 1). Also in controls we observed a significant decrease in PGE2 (P = 0.001), glutamate (P = 0.0001) and bradykinin (P = 0.0001) at baseline compared with the stabilization period (Fig. 1).
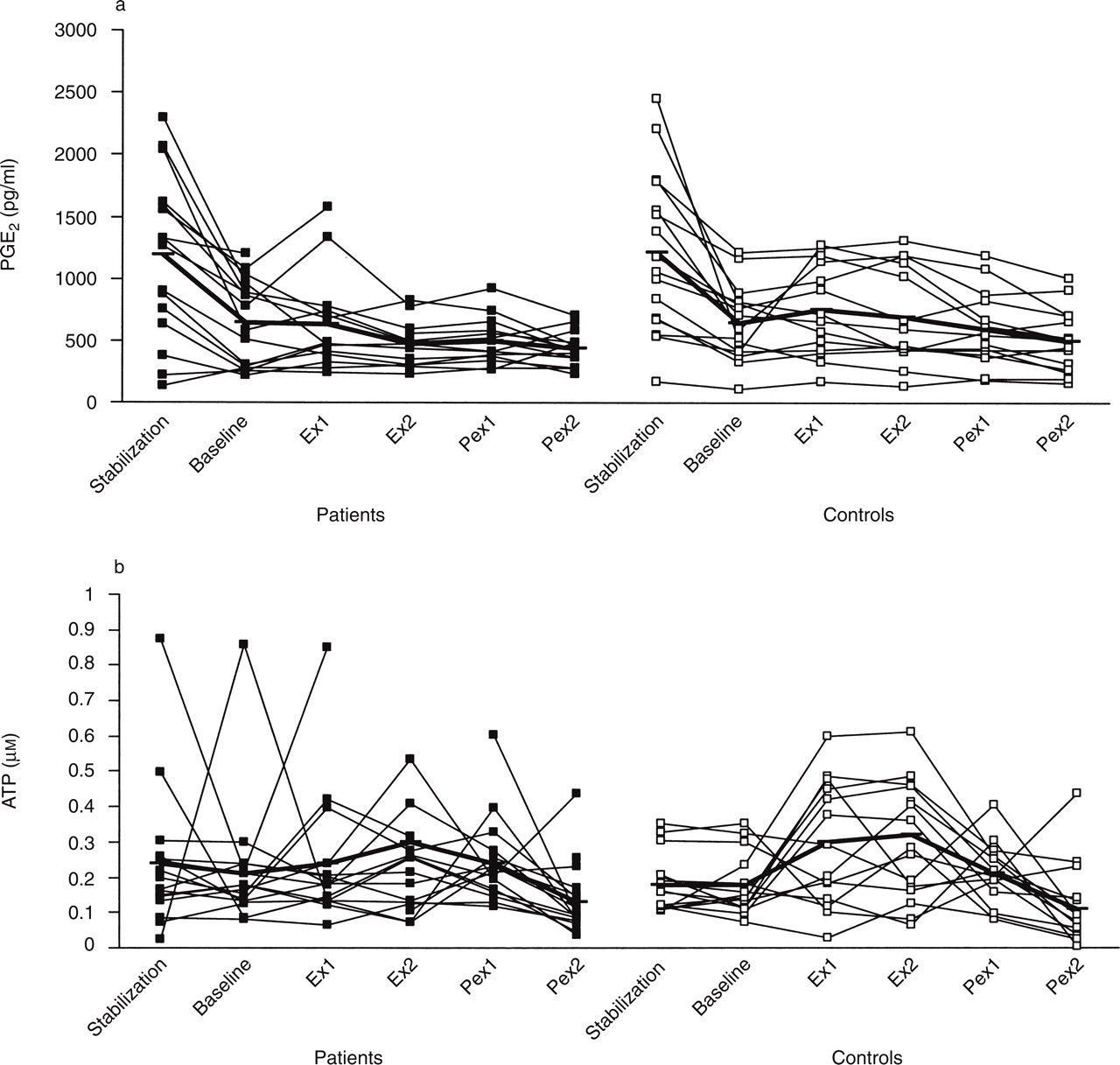
Interstitial concentration of prostaglandin E2 (PGE2) (a), adenosine 5′-triphosphate (ATP) (b), glutamate (c) and bradykinin (d) in 16 patients (▪) and 17 controls (□). (a, b, c) There was no difference in change in interstitial concentration of inflammatory mediators from baseline (Rest) to exercise (15 min (Ex 1) and 30 min (Ex 2) after start of exercise) and post-exercise (15 min (Pex 1) and 30 min (Pex 2) after stop of exercise) periods between patients and controls (P > 0.05). (d) Baseline interstitial concentration of bradykinin did not differ between patients and controls (P = 0.68). Thick line in figures shows mean concentrations.
During the rest period (baseline), we found no difference in interstitial concentration of ATP (P = 0.47), PGE2 (P = 0.99), glutamate (P = 0.46), glucose (P = 0.95), pyruvate (P = 0.70), urea (P = 0.67) and bradykinin (235 ± 33 vs. 218 ± 24 pmol/l, P = 0.68) between patients and controls (Table 2 and Fig. 1). Also interstitial concentration of potassium did not differ between patients, 4.4 ± 0.3 m
Interstitial concentrations of metabolites in 16 patients with chronic tension-type headache (p) and 17 healthy controls (c) during stabilization period (0–60 min), baseline (60–120 min), 15 (Ex 1) and 30 (Ex 2) min after start of exercise and 15 (Pex 1) and 30 (Pex 2) min after stop of exercise

Data are mean ± SEM.
The two-way repeated measures
Local tenderness
At the end of the experiment, after removal of the catheters from the muscle, the mean local tenderness had increased significantly from 34 ± 5 to 53 ± 6 mm in patients (P = 0.001) and from 3 ± 1 to 25 ± 4 mm in controls (P = 0.0001) (8).
Discussion
Present results
The major outcome of the present study is that there were no signs of ongoing inflammation in a tender trapezius muscle of patients with chronic tension-type headache in either resting muscle or in response to static exercise. Furthermore, the present findings indicate that diminished blood flow in the tender muscle during static work in the same patients (8) is probably not associated with inflammation or altered muscle metabolism. These conclusions are based on the present findings that interstitial concentrations of PGE2, ATP, glutamate, bradykinin, potassium, glucose, pyruvate and urea did not differ between patients and controls. The question then is whether increased tenderness could be explained by muscle allodynia, i.e. an excessive reaction to stimuli that normally do not evoke pain. If so, where is the site of primary hyperalgesia in patients with chronic tension-type headache? It has been suggested that pericranial myofascial tissues may be sites of primary hyperalgesia in episodic tension-type headache (3) and that prolonged painful input from these tissues, e.g. tender points, may result in central sensitization, i.e. increased excitability of neurones in the CNS (1). The major outcome of these events would be conversion of episodic into chronic tension-type headache that might be an entirely central process without further or only minimal input from the periphery (1). Thus, our data are compatible with this hypothesis, i.e. that muscular factors play no or only a minor role once central sensitization and thereby the chronic pain state has been established (1). However, the pathophysiological basis for the painful input from the periphery in episodic tension-type headache is still unknown, and this important issue should be addressed in future studies.
Increased interstitial ATP during static exercise
One of the interesting findings in the present study was an increase in interstitial levels of ATP in response to static exercise in both patients and controls. Slightly decreased levels of ATP have previously been reported in open muscle biopsy studies in patients with chronic trapezius myalgia (18, 19). However, in these studies there are several methodological reservations such as a small number of patients, only female patients were examined, and biopsies were not performed in a blind fashion in respect to patients and controls. Our data do not suggest a decreased ATP concentration in patients compared with controls. However, our findings confirm the previous findings by Hellsten et al. (20) who reported an increase of ATP in the exercising muscle interstitium in healthy subjects. Inflammation or traumatic injury may lead to cell lysis and subsequent release of intracellular ATP into the extracellular space (21). One may therefore suggest that the increased intramuscular pressure and movement of the catheter during exercise intensify the cell lysis caused by insertion of the catheter. This could lead to the increase of extracellular ATP during exercise demonstrated in the present study. However, Hellsten et al. (22) concluded that their findings of a gradual increase of ATP concentration in the five exercise intensities performed in random order seem to rule out tissue damage as the cause of increase in ATP. Thus, the source of extracellular ATP is far from clarified, and other sources such as release of ATP from nerve endings to the interstitial space (23) should also be considered.
Methodological considerations
In the present study we have taken great care to optimize the methodology. Thus, we used a microdialysis technique that enables examination of muscle metabolism in vivo within a small area (24) such as a tender point. Furthermore, we examined a well-characterized group of patients during headache. Inflammatory mediators were examined in a tender point confirmed by pressure-controlled palpation (2). Measurement was performed both at rest and in response to static exercise, which resembles a sustained working position known as a common trigger factor in tension-type headache. All samples were analysed blindly with respect to patients and controls, and patients were compared with healthy controls matched for age, sex, BMI and maximum voluntary trapezius muscle force. We did not calibrate microdialysis catheters directly for all the inflammatory mediators and metabolites and, accordingly, only dialysate concentrations were determined. However, the in vivo relative recovery for lactate differed neither between groups nor with time (8) and the dialysate concentration is therefore a direct measure of the interstitial concentration. This corresponds with the fact that concentrations of urea, shown to be an endogenous recovery marker (25), were identical between groups and constant throughout the experiment.
It could be argued that clinically relevant changes in interstitial concentrations of inflammatory mediators could be too small to be detected with the present methods. We find this unlikely, because there was not even a trend towards differences in the concentration of any of the inflammatory mediators between patients and controls at baseline. Neither did concentrations of inflammatory mediators differ between patients and controls in response to static exercise.
It would have been interesting to measure interstitial levels of other potentially important metabolites. However, this was difficult for practical reasons. In order to ensure that dialysate concentrations do not differ much from interstitial concentrations (i.e. that recovery is high), catheters have to be perfused with a low flow rate (2 µl/min), which yields small amounts of dialysate. Thus, our study does not exclude possible alterations in concentrations of other substances, e.g. neuropeptides.
Conclusion
The present study provides in vivo evidence of normal interstitial levels of inflammatory mediators and metabolites in tender trapezius muscle in patients with chronic tension-type headache during both rest and static exercise. These findings suggest that chronic myofascial tenderness is not caused by ongoing inflammation.
Footnotes
Acknowledgements
We would like to thank Hanne Andresen, Lisbeth Kall, Regitze Krauns⊘e and Alice Rudböl for skilful technical assistance and Dr Rigmor Jensen for valuable comments during the preparation of the manuscript. The Danish Medical Association Research Fund, the Danish Hospital Foundation for Medical Research, Region of Copenhagen, the Faroe Islands and Greenland, the Foundation for Research in Neurology, the Novo Nordisk Foundation, the Danish National Research Foundation (grant 504-14), the Gerda and Aage Haensch's Foundation, the Mauritzen La Fontane's Foundation, the Foundation of Jacob Madsen and his wife Olga Madsen supported the study financially.