
Abstract
We assessed the prevalence of menstrual migraine and its restrictions on daily activities in a representative Dutch population sample of 1181 Dutch women, aged 13-55 years. Further, we evaluated the potential role of oral contraceptives, and how menstrual migraine is treated. More than half suffered from menstrual complaints, a substantial proportion reported headache or migraine as a frequent problem. Use of oral contraceptives seemed to reduce the occurrence of menstrual complaints, but not the occurrence of headache and migraine. In our study, the prevalence of menstrual migraine (3%) is lower than in the literature, most probably because we did not use a selected group of patients but a population-based sample of ordinary women. It was confirmed that attacks of menstrual migraine are more severe, of longer duration, and more resistant to treatment than migraine attacks at other times of the month.
Introduction
Migraine is a common headache disorder. Attack onset is usually before the age of 20 years, with peak prevalence between the ages of 25 and 55 years. After puberty, migraine is two to three times more common in women than in men (1).
Many women report that their migraines are associated with the menses (2). In this context, patients and doctors commonly use the term ‘menstrual’ migraine. Clinical experience suggests that menstrual migraine attacks are more severe, longer in duration, and more difficult to treat than migraine attacks at other times of the month. However, this has not been confirmed in objective comparative studies (3). Menstrual migraine attacks are usually not associated with aura (4). Epstein reported that menstrual migraine has a peak onset associated with menarche, is most prevalent around 40 years of age, and declines with menopause (5).
Despite the frequent use of the term menstrual migraine, there is no definition in the classification system of the International Headache Society (IHS) (6). The current classification states: ‘Migraine without aura may occur almost exclusively at a particular time of the menstrual cycle—so-called menstrual migraine. Generally accepted criteria for this entity are not available. It seems reasonable to demand that 90% of attacks should occur between two days before menses and the last day of menses, but further epidemiological knowledge is needed’. As a result, many questions remain about the prevalence, cause and treatment options. Based on studies demonstrating that menstrual migraine attacks peak shortly before or after the onset of menstruation, MacGregor proposed that menstrual migraine should be defined as ‘migraine attacks that occur regularly on or between days −2 or +2 of the menstrual cycle and at no other time’ (7).
In this study, our aim was to assess the prevalence of menstrual migraine in a representative Dutch population sample. In addition, we evaluated restrictions in daily activities associated with menstrual migraine, the potential role of oral contraceptives, and how menstrual migraine is treated.
Methods
The study was conducted by the Netherlands Institute on Public Opinion (NIPO) among 1181 Dutch women, aged 13–55 years, between June and September 2001. The sample was representative for the Dutch female population of the same age. For data collection NIPO used a database called CAPI@HOME, containing more than 20 000 households who use their own personal computer to participate in all types of research. Questionnaires are sent to the respondent or to a selected group by modem or internet. CAPI@HOME offers the advantages of the CAPI formula (Computer-Assisted Personal Interviewing), including optimum sampling and error-free routing of questionnaires. The demographic variables of the respondents are known. This implies that sample size of a specific group can be estimated in order to obtain representativity of the Dutch population (8).
The study population was identified in two steps. Between 22 June and 24 July 2001, a sample of 1139 women 13–55 years of age was systematically screened to find women with regular menstrual cycles, defined as at least eight menstrual bleedings in the past 12 months. In September 2001, an additional 42 women with menstrually related IHS migraine were included in the study through a second sample survey in order to get a larger data set on the characteristics of menstrual migraine. This resulted in a complete sample of 1181 women, of whom 982 had regular menstrual cycles. Each woman was then asked to respond to questions about ‘a health-related topic’. They were not told in advance they would be queried about menstrual migraine. The questions we used enquired about menstrual complaints, use of oral contraceptives, symptoms, frequency and severity of headache, headache-related disability, treatment, and healthcare consulting behaviour. The migraine diagnosis was determined from responses to the questionnaire (Fig. 1). Headache-related disability was assessed by questions on duration, frequency and severity of impairment in various daily activities, including household chores, social activities, sports, work and school. For calculation of the prevalence, the latter sample was weighted to correct for adding extra cases, yielding unbiased national estimates. The following definitions were used for the distribution of women according to their type of menstrually related migraine:

(a) Study profile—unweighted sample. (b) Study profile—weighted sample. ∗Migraine not confirmed by International Headache Society criteria.
Menstrually related IHS migraine: migraine attacks confirmed by IHS criteria that start on or between 2 days before menstruation and the last day of menstruation. In this category, women were also allowed to have migraine attacks at other times than menstruation.
Menstrual migraine: migraine attacks confirmed by IHS criteria that start on or between days −2 or +2 of menstruation. In this category, women were also allowed to have migraine attacks at other times than menstruation.
Menstrual migraine according to MacGregor or ‘true’ menstrual migraine: migraine attacks confirmed by IHS criteria that start on or between days −2 or +2 of menstruation and at no other time.
Subjective migraine: migraine attacks that start between 2 days before menstruation and the last day of menstruation, reported on women's own account (i.e. women in this category said they had migraine, but their headaches did not fulfil the IHS criteria). In this category, women were also allowed to have migraine attacks at other times than menstruation.
Results
Oral contraceptives
Of women with regular menstrual cycles, 52% used oral contraceptives. The use of oral contraceptives declined with age. Of women between the ages of 20 and 29 years, 74% used oral contraceptives, compared with 50% of women between the ages of 30 and 39 years and 32% of women between the ages of 40 and 55 years. More than half (58%) of the women with regular cycles reported menstrual complaints. Women using oral contraceptives were less likely to report menstrual complaints (52%) than women not using oral contraceptives (65%).
Menstrual complaints
Of women with menstrual complaints, 34% reported the complaints to occur on or between days −2 and +2 of the menstrual cycle. In 24% of women the complaints occurred before the onset of menstruation and in 18% of women during menstruation. Another 15% of women reported the complaints to occur during a period longer than on or between days −2 and +2 of the menstrual cycle. A substantial proportion of women reported headache (except migraine) (48%) or migraine (14%) to be a frequent menstrual complaint (Table 1). These numbers did not significantly differ between women who used oral contraceptives and women who did not (data not shown). The proportion of women with headache significantly increased with age, with 32% of women with headache in the group aged 13–19 years, 48% of women with headache in the groups aged 20–29 and 30–39 years, and 57% of women with headache in the group aged 40–55 years. The proportion of women with migraine also increased with age, but this was not significant (8% in the group aged 13–19 years, 13% in the groups aged 20–29 and 30–39 years, and 19% in the group aged 40–55 years).
Menstrual complaints∗

∗More than one answer possible.
Menstrual migraine
Of the 982 women with regular menstrual cycles, 116 suffered from menstrually related IHS migraine (weighted prevalence 8%[75/936]), 45 of them having menstrual migraine (weighted prevalence 3%[28/936]). Twelve women suffered from menstrual migraine according to MacGregor (weighted prevalence 0.85%[8/936]) (Fig. 1b). Another 225 women had other types of headache related to menstruation (weighted prevalence 23%[217/936]). Subjective migraine was reported by 126 women (weighted prevalence 9.0%[84/936]) (Fig. 1b). Women with menstrually related IHS migraine and women with menstrual migraine reported their headache complaints to occur on a frequent basis (mean 9.8 and 9.9 times per year, respectively).
Advice and treatment
Women with subjective migraine were most likely to visit their primary care doctor, followed by women with menstrually related IHS migraine and women with menstrual migraine. The proportion of women advised to use medication was also greatest among women with subjective migraine (Table 2).
Visit primary care doctor, advice and medication
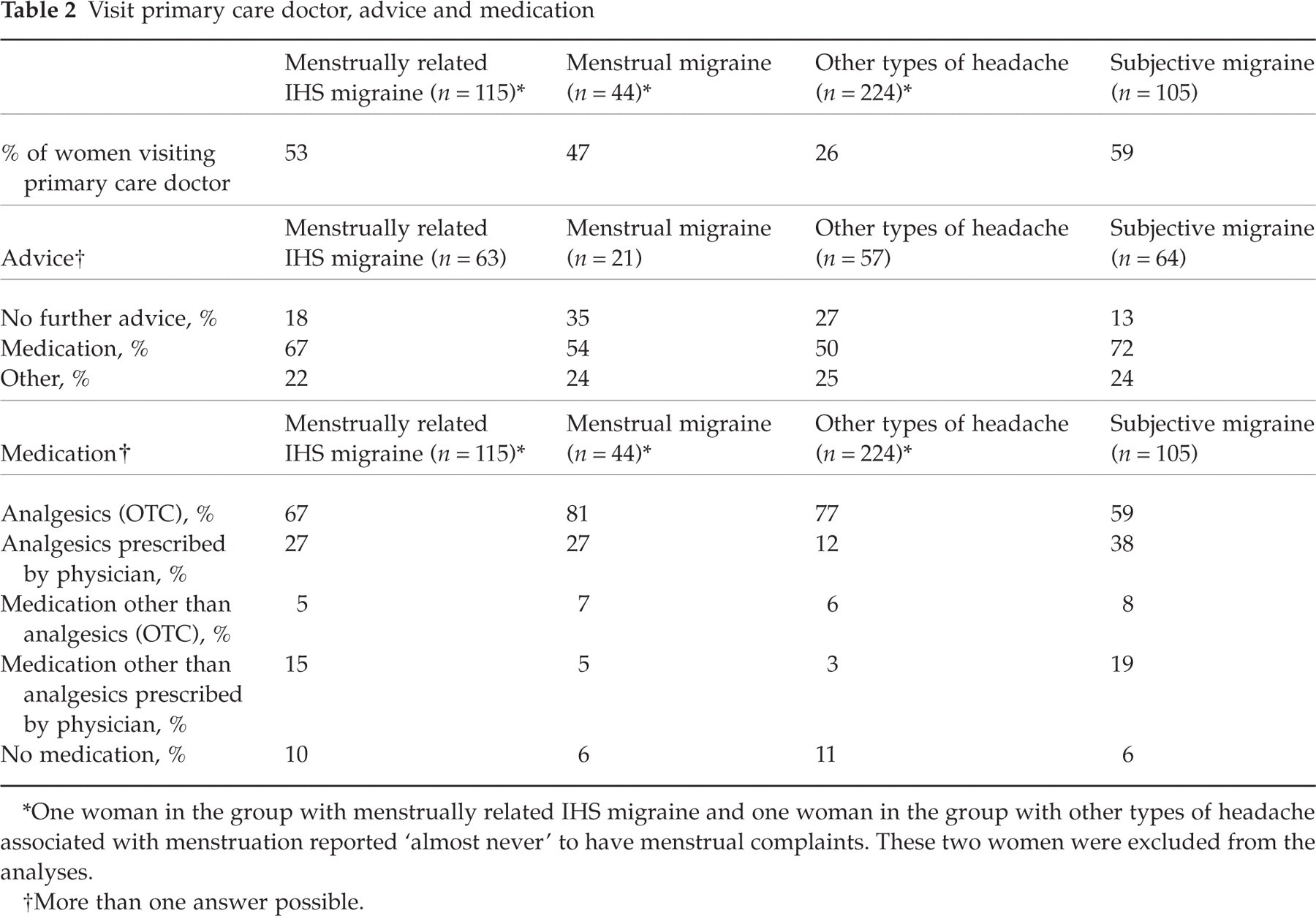
∗One woman in the group with menstrually related IHS migraine and one woman in the group with other types of headache associated with menstruation reported ‘almost never’ to have menstrual complaints. These two women were excluded from the analyses.
†More than one answer possible.
In all groups, analgesics were the most frequently used medication. Relatively few women reported the use of prescription medication, particularly in the group of women with menstrual migraine (Table 2). Women with menstrually related IHS migraine were more inclined to change therapies, e.g. to switch, stop or start oral contraceptives, than women with other types of menstrually related headaches (Table 3).
Use of oral contraceptives

∗One woman in the group with menstrually related IHS migraine and one woman in the group with other types of headache associated with menstruation reported ‘almost never’ to have menstrual complaints. These two women were excluded from the analyses.
Women with menstrually related IHS migraine and menstrual migraine also asked family members (44–55%) and friends or colleagues (43%) for advice. Another 26–30% asked no advice. In the group of women with other types of headache, 23% said to approach family members, 25% said to approach friends or colleagues, and 59% asked for no advice. In all groups, a small minority of women had visited medical specialists other than their primary care doctor, including gynaecologists, neurologists, anaesthesiologists, rheumatologists, ophthalmologists, and homeopaths (data not shown).
Disability patterns
As expected, women with menstrually related IHS migraine were more disabled by their headache attacks than women with other types of menstrually related headaches (Table 4). Overall, women who had their migraine both at the time of menstruation and at other times of the month (n = 32) reported that their menstrually related migraine attacks were more severe, of longer duration, and more resistant to treatment. The same was true for women with subjective migraine (n = 32).
Restrictions in daily activities

NA, Data not available.
∗One woman in the group with menstrually related IHS migraine and one woman in the group with other types of headache associated with menstruation reported ‘almost never’ to have menstrual complaints. These two women were excluded from the analyses.
Discussion
This study shows that more than half of Dutch women with regular menstrual cycles suffer from menstrual complaints. Of these women, a substantial proportion report headache or migraine as a frequent problem. Use of oral contraceptives seems to reduce the occurrence of menstrual complaints in general, but not the occurrence of headache and migraine in particular.
In the literature, prevalence figures of menstrual migraine vary from 4% to 73% (2). In retrospective studies in headache clinic patients, the prevalence ranges from 26% to 60% (9). A prospective study in 55 women attending a headache clinic demonstrated that 7.2% of women had menstrual migraine according to MacGregor (2). Another 34.5% of women had an increased number of migraine attacks at the time of menstruation in addition to attacks at other times of the month. The prevalence of menstrual migraine in our study (3%) and menstrual migraine according to MacGregor (0.85%) is strikingly lower, most probably because we did not use a selected group of patients but a population-based sample of ordinary women. Nevertheless, a substantial proportion of Dutch women with regular menstrual cycles suffer from menstrually related migraine or headache, extrapolated 310 000 women with menstrually related IHS migraine, 115 000 women with menstrual migraine, 33 000 women with menstrual migraine according to MacGregor, and 890 000 women with other types of headache.
Our study also shows that menstrually related IHS migraine and menstrual migraine occur on frequently (approx. 10 times per year) and cause significant limitations of daily activities. Previous population-based surveys found similar disability patterns among migraineurs. The American Migraine Study reported that 85% of migraine patients had at least some headache-related disability (10). A Canadian survey found that patients with migraine were more disabled than patients with tension-type headache (11). Our finding that menstrually related migraine attacks are more severe, of longer duration, and more resistant to treatment than migraine attacks at other times of the month is in keeping with the overall clinical experience reported by others (3, 9), but remains controversial (12). A recent prospective population-based daily diary study among 81 menstruating women was not able to demonstrate that menstrually related migraine attacks differ significantly from migraine attacks at other times of the month with regard to symptoms, duration, disability and pain intensity (12).
We further observed that women with menstrually related IHS migraine, menstrual migraine or subjective migraine are more likely to visit their primary care doctor than women with other types of headache. This might be directly related to the disabling character of the attacks, yet a substantial proportion of women do not see a doctor or, when seeing a doctor, are not advised to use medication. This suggests that women and physicians tend to underestimate the severity of the disorder or tend to accept migraine as ‘part of the menses’. Other possible explanations might be hypochondria or somatic preoccupation. On the other hand, it might be a well-considered choice of both the patient and the physician to treat the attacks with over-the-counter medication instead of using prescription medication, despite a confirmed diagnosis of migraine.
Finally, women with menstrually related IHS migraine were more likely to switch, stop or start oral contraceptives, compared with women with other types of headache associated with menstruation. The association between migraine and oral contraceptives is still controversial. Becker reported that oral contraceptive use can result in worsening, improvement, or no change in a woman's migraine. The pattern of the migraine attack may also change with oral contraceptives (13). Studies comparing oral contraceptives containing different amounts of oestrogen and progesterone were not able to demonstrate a difference in the occurrence of headache or migraine (14).
Our study has several methodological limitations. The association of migraine with the menstrual cycle as reported by the women is subject to bias. Menstrually related migraine would have been more accurately identified by the use of prospective headache diaries for at least 3 months (15–17). The same is true for the migraine-related disability. Furthermore, the migraine diagnosis was determined from responses to the questionnaire and not on an in-person evaluation by a physician. This might have led to an over- or under-estimation of the number of women with migraine. A study on self-awareness of migraine found that individuals who claimed to have migraine were correct only one-third of the time. Individuals failing to self-recognize migraine often misreported terms like ‘location’, ‘severity’ and ‘throbbing’ (18). With respect to medical advice and medication use, we have no data on the physician's perspective. Therefore, we have no insight into the reasons ofor not treating the patient.
We conclude that more than half of the Dutch female population with regular menstrual cycles suffer from menstrual complaints, with headache and migraine being frequent problems. Menstrually related IHS migraine is a prevalent disorder and is more likely to cause limitations of daily activities than other types of menstrually related headache. The prevalence of menstrual migraine and menstrual migraine according to MacGregor (‘true’ menstrual migraine) is, however, strikingly low. In our sample, attacks of migraine in relation to menstruation were more severe, of longer duration, and more resistant to treatment than migraine attacks at other times of the month. Lack of awareness in both patient and physician results in underdiagnosis and undertreatment. There is strong need for greater patient and professional education about menstrual migraine and the best ways to manage the disorder. More research is needed to look into the role of hormones in migraine pathophysiology, the impact of oral contraceptives, and therapy options.
Footnotes
Acknowledgements
We thank Anita van den Oetelaar for the preparation of the manuscript, and the Stichting Voorlichtingsbureau Hoofdpijn for their grant to use the NIPO.