
Abstract
The aim of this study was to investigate prospectively the course of migraine during pregnancy and postpartum. Of all the pregnant women consecutively attending an obstetrics and gynaecology department for a routine first-trimester antenatal check-up, 49 migraine sufferers - two were affected by migraine with aura (MA) and 47 by migraine without aura (MO) - who had experienced at least one attack during the 3 months preceding pregnancy were identified, enrolled in the study and given a headache diary. Subsequent examinations were performed at the end of the second and third trimesters and 1 month after delivery. Migraine was seen to improve in 46.8% of the 47 MO sufferers during the first trimester, in 83.0% during the second and in 87.2% during the third, while complete remission was attained by 10.6%, 53.2%, and 78.7% of the women, respectively. Migraine recurred during the first week after childbirth in 34.0% of the women and during the first month in 55.3%. Certain risk factors for lack of improvement of migraine during pregnancy were identified: the presence of menstrually related migraine before pregnancy was associated with a lack of headache improvement in the first and third trimesters, while second-trimester hyperemesis, and a pathological pregnancy course were associated with a lack of headache improvement in the second trimester. Breast feeding seemed to protect from migraine recurrence during postpartum.
Introduction
It is common knowledge that migraine, particularly migraine without aura (MO), is influenced by the cyclical changes in sex hormones during reproductive life (1–3). The attacks often occur during the menstrual period, prevalently in about 60% (3) and exclusively in 7–9% of women affected by MO (3, 4).
Migraine is generally seen to improve during pregnancy and during the menopause, two conditions that are characterized by opposing oestrogen plasma level trends: rising during the former and decreasing after the latter (1, 3, 5–12). This is probably due to the absence of hormonal fluctuations in both these situations. In fact, the most widely accepted hypothesis on the pathogenesis of menstrual attacks points to the fall in oestrogens during the premenstrual period (13).
Several studies have demonstrated that migraine improves or disappears in most women during pregnancy. However, the majority of these observations are retrospective, the patients having been evaluated several years after pregnancy or, at best, in the postpartum period (1, 3, 5–11).
The aim of this work was to investigate prospectively, through a diary-based study, the course of migraine during pregnancy and postpartum in a sample of migraineurs from an obstetrics and gynaecology department.
Subjects and methods
Of all the pregnant women consecutively attending the Department of Obstetrics and Gynaecology of the University of Pavia for a first routine antenatal check-up, those who suffered from migraine with aura (MA) or MO and had experienced at least one attack during the 3 months preceding pregnancy were enrolled in the study.
The diagnosis of MA and MO was made according to the diagnostic criteria of the International Headache Society (IHS) classification (14).
At the first examination (taking place on average in week 11; range weeks 9–13) the women were administered a detailed questionnaire investigating: demographic data, gynaecological history and migraine history and characteristics (particular attention was paid to the relationship between migraine attacks and menses, to migraine onset at menarche and to migraine course during previous pregnancies).
In view of the difficulty in identifying retrospectively a pure menstrual migraine and in distinguishing it from a menstrually related migraine (15), we grouped these two categories under the umbrella heading of menstrually related migraine, thus including migraines occurring only during menses and those occurring both during and outside menses. The occurrence of other types of headache besides migraine was carefully investigated.
The women returned for three further examinations: at the end of second and third trimesters of pregnancy, and 1 month after delivery.
At the first examination, all the women were given a diagnostic headache diary. This was to be used for defining the type of headache attacks (migraine or tension-type headache) and for assessing migraine attack frequency, severity and duration and analgesic consumption. At the subsequent examinations the headache diaries were collected and the course of pregnancy was monitored. Blood pressure and heart rate were recorded, as well as body weight and lifestyle habits, such as smoking, alcohol consumption, physical activity, and use of medication. The use of specific drugs for tocolysis, such as ritodrine and isoxysuprine, was carefully monitored throughout gestation. All the women had been taking folic acid supplements since the start of pregnancy and were treated with iron supplementation upon blood testing.
At the postpartum examination, information was also gathered on the delivery, the type of feeding and the newborn. Women who had to bottle feed were administered a single dose of cabergoline to inhibit plasma prolactin levels during postpartum. The number of attacks in the trimester preceding pregnancy and during the weeks of pregnancy leading up to the first examination was noted retrospectively, while all subsequent attacks were recorded prospectively.
Because it is less subject to recall bias, attack frequency (<1/month; 1–3/month; 1–3/week) was taken as the main outcome parameter on the basis of which to assess migraine course during pregnancy compared with the pregravid period.
To evaluate the migraine course during the trimesters of pregnancy and the postpartum period, the number per trimester, severity (on a scale of 1–3: 1 = mild, it does not impair daily activities; 2 = moderate, it inhibits, but does not prohibit daily activities; 3 = severe, it prohibits daily activities) and duration (in days) of attacks were recorded, as were details of analgesic consumption. A ≥ 50% reduction in the number of attacks was classed as an improvement, while complete cessation of attacks was defined as remission.
Statistical analysis
Statistical analysis was performed using the χ2 test, Student's t-test and one-way
Results
Demographic characteristics
In the 6-month period of recruitment (1 October 1998 to 31 March 1999), 392 women attended the Department of Obstetrics and Gynaecology of the University of Pavia for a first routine antenatal check-up. Of the total 392, 71 were identified as migraineurs (59 having MO, and 12 MA). Twenty-two of these women (13 MO, nine MA) were excluded from the study because of: absence of attacks in the trimester preceding pregnancy (n = 14), unwillingness to cooperate (n = 3), inability to collaborate for cultural reasons (mainly immigrants with inadequate knowledge of the Italian language) or mental impairment (n = 5). Forty-nine women were thus included in the study, 47 suffering from MO and two from MA. The demographic characteristics of our population are detailed in Table 1.
Demographic characteristics of 49 pregnant women affected by migraine
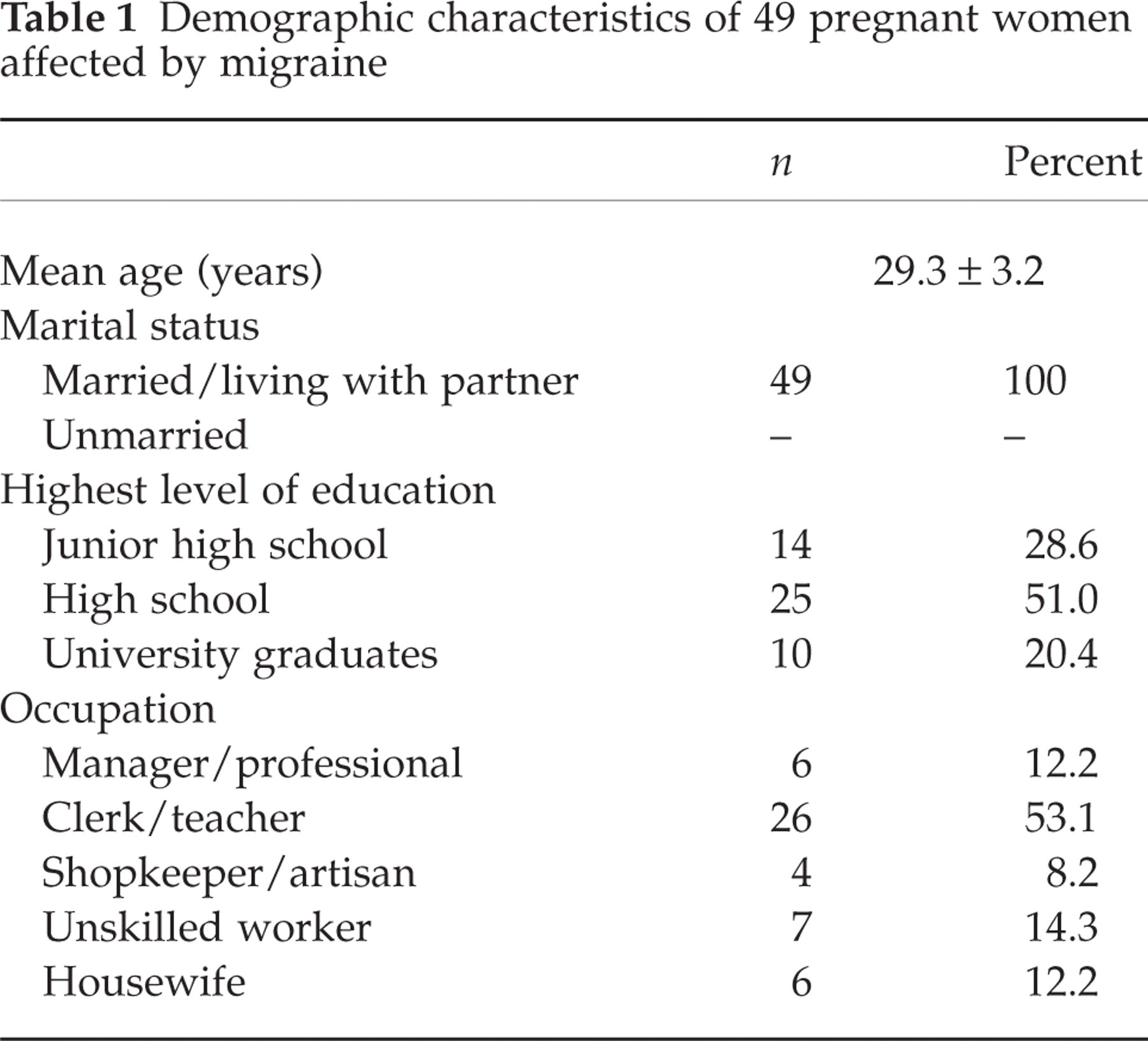
Thirty-seven women (75.5%) were primigravids, and the other 12 (24.5%) were secondiparas. The pregnancy was desired/planned in 45 women (91.8%), and unexpected in four (8.2%).
Migraine history
Table 2 shows the mean age of the patients at migraine onset and the relationship between migraine and some reproductive life events. Twelve women (24.5%) were also affected by episodic tension-type headache.
Age at migraine onset and relationship between migraine and reproductive life events in 49 pregnant migraineurs

Course of pregnancy and delivery
Nausea was reported by 40 (81.6%) women during the first trimester, and was still present in eight (16.3%) during the second trimester. None of the subjects reported nausea during the third trimester. Body-weight increase was 13.8 ± 2.4 kg (range 9–18 kg) at term. Four women (8.1%) experienced a pathological course of pregnancy during the second trimester – uterine hyperkynesia (n = 2) and risk of preterm delivery (n = 2) – and 10 (20.4%) during the third trimester – two subjects suffering pregnancy-induced hypertension with mild preeclampsia at term, and eight subjects having uterine contractions or premature rupture of membranes, leading to preterm labour in three cases. Thirty-five women (71.5%) had vaginal deliveries, six (12.2%) underwent uncomplicated caesarean section due to breech presentation or failure to progress, and eight (16.3%) underwent emergency caesarean section due to pathological states of both mother and fetus.
Course of migraine during pregnancy
In the two women affected by MA, there was no change in the pattern of their migraine during pregnancy: both had one attack during the 3 months preceding pregnancy, no attacks during first trimester and one attack during each of the last two trimesters. The small number of patients with MA precluded any attempt to outline the course of this condition during pregnancy. Therefore, all the results given here refer to the 47 women affected by MO.
The attack frequency in the 3 months preceding pregnancy and the three trimesters of pregnancy are illustrated in Fig. 1. While only a few women experienced no attacks during the first trimester, the majority experienced a reduction from one to three attacks/month to less than one attack/month. During the last two trimesters an increasing number of women experienced a complete remission, and only two women (4.3%) maintained a medium frequency of attacks (1–3/month). No woman experienced an increase in attack frequency during pregnancy compared with the pregravid period.

Attack frequency during the 3 months preceding pregnancy and during the trimesters of pregnancy in 47 women affected by migraine without aura. ▪, No attacks; □, less than one attack/month; hatched, 1–3 attacks/month; double hatched, 1–3 attacks/week. First trimester vs. pregravid period, P = 0.0001; second vs. first trimester, P = 0.0001; third vs. second trimester, P = 0.02.
The overall number of attacks fell from 80 in the first trimester to 34 in the second and 14 in the third. In the 22 women experiencing attacks in the first two trimesters, the mean number of attacks per trimester dropped from 2.4 ± 1.3 during the first to 1.5 ± 1.5 during the second trimester (P = 0.002); in the 10 women who continued to experience attacks during the last two trimesters, the mean number of attacks per trimester fell from 2.0 ± 2.1 in the second trimester to 1.4 ± 0.8 in the third (P = NS).
Figure 2 shows the course of migraine during pregnancy. Almost half of the women (46.8%) showed an improvement in the first trimester, but complete remission was infrequent (10.6%). A substantial decrease in migraine activity occurred during the second trimester (improvement 29.8%, remission 53.2%). During the third trimester an additional improvement was seen, mainly in terms of a shift from improvement to complete remission (remission 78.7%; improvement or remission 87.2%). None of the women experiencing a complete remission during the first trimester went on to have migraine attacks during the last two trimesters; likewise, none of the women experiencing a complete remission during the second trimester reported a migraine attack during the third trimester.

Course of migraine during pregnancy in 47 women affected by migraine without aura. ▪, Improvement (reduction ≥50% of the attack number per trimester); □, remission (complete absence of attacks); hatched, improvement or remission. Remission: second vs. first trimester, P = 0.0001; third vs. second trimester, P = 0.02. Improvement or remission: second vs. first trimester, P = 0.006; third vs. second trimester, P = NS.
The mean pain intensity of residual attacks showed a trend towards improvement during pregnancy (first trimester = 2.2 ± 0.3; second trimester = 2.3 ± 0.4; third trimester = 2.0 ± 0.0; P = 0.06). Indeed, in the 10 women who experienced attacks throughout their pregnancies, the mean attack severity decreased from 2.5 ± 0.3 in the first trimester to 2.0 ± 0.0 in the third trimester (P = 0.001). In contrast, no change was found in the duration of the attacks (first trimester = 1.1 ± 0.2 days; third trimester 1.0 ± 0.0 days).
All the women took analgesics (paracetamol 500 mg) for all their attacks. Analgesic consumption decreased in the third trimester, reflecting the decrease in pain intensity in this latter part of pregnancy. In fact, of the 10 women who experienced attacks throughout their pregnancies, analgesic intake per attack fell from 1.9 ± 0.7 tablets in the first trimester to 1.2 ± 0.4 tablets in the third trimester (P = 0.02).
Factors influencing the course of migraine during pregnancy
Upon multivariate analysis (Table 3), the following emerged as factors associated with failure of migraine to improve: pre-pregnancy menstrually related migraine was linked with a lack of improvement during the first trimester (P = 0.005); hyperemesis (P = 0.0002) and pathological pregnancy course (P = 0.03) were linked with a lack of improvement during the second trimester; pre-pregnancy menstrually related migraine (P = 0.0002) and pathological pregnancy course (P < 0.00001) were linked with a lack of improvement during the third trimester.
Distribution of migraine course during pregnancy according to characteristics of patients, migraine and pregnancy
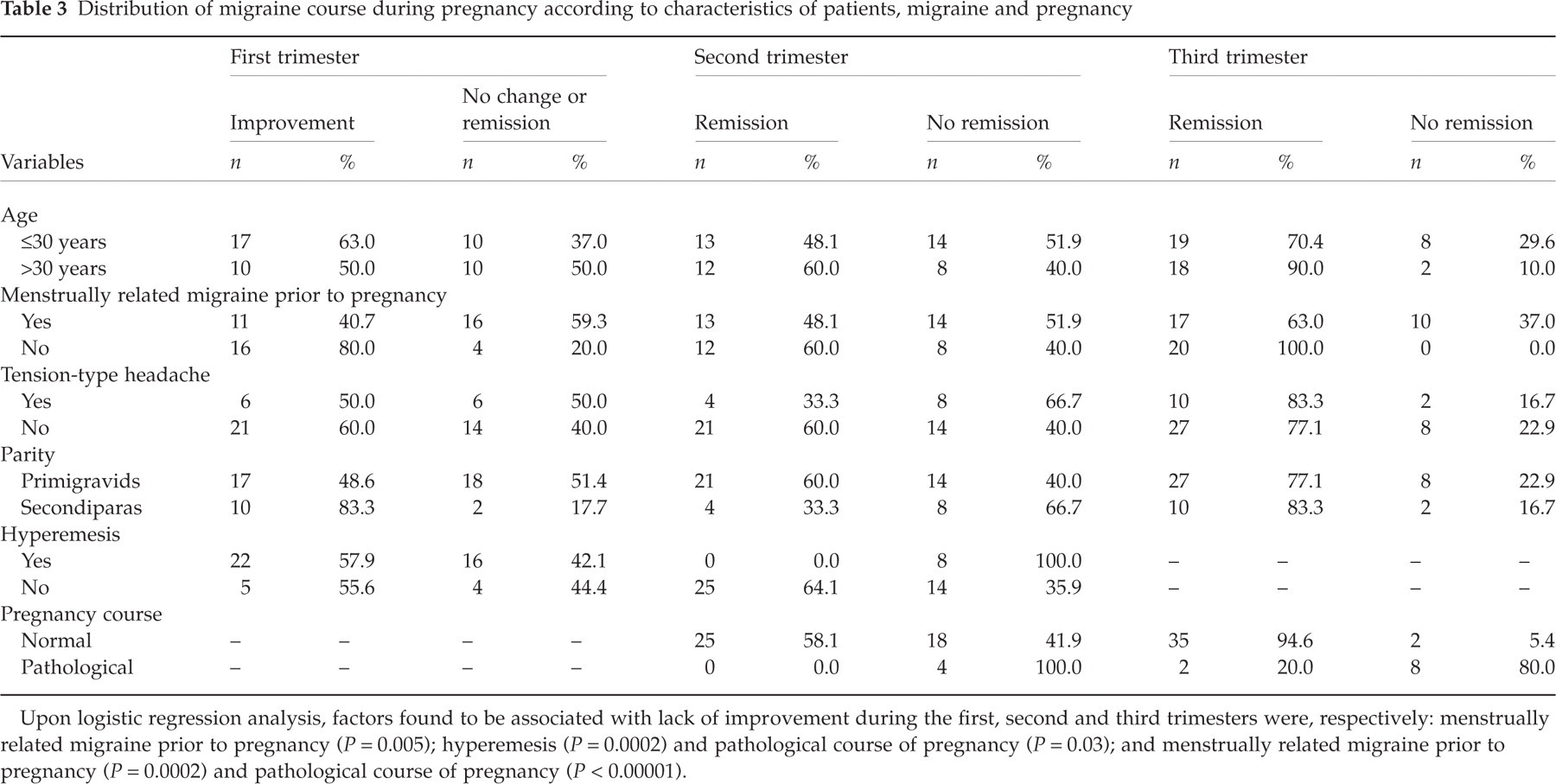
Upon logistic regression analysis, factors found to be associated with lack of improvement during the first, second and third trimesters were, respectively: menstrually related migraine prior to pregnancy (P = 0.005); hyperemesis (P = 0.0002) and pathological course of pregnancy (P = 0.03); and menstrually related migraine prior to pregnancy (P = 0.0002) and pathological course of pregnancy (P < 0.00001).
Course of migraine during postpartum
Migraine was often found to return quickly after delivery: within 48 h in two patients (4.3%), within 1 week in 16 (34.0%), and within 1 month in 26 (55.3%). Of the 26 patients who experienced attacks during first month after delivery, 18 (69.2%) reported one attack and eight (30.8%) two attacks. The mean severity of the attacks was 2.4 ± 0.5 and the mean duration 1.2 ± 0.5 days. All the women had recourse to analgesics (paracetamol, piroxicam, sumatriptan, combination drugs) for their headaches, taking a mean of 1.9 ± 1.0 tablets per attack. In the eight patients who had continued to experience attacks in the third trimester, attack severity was found to worsen during postpartum, rising from 2.0 ± 0.0 to 2.3 ± 0.4 (P = 0.05).
Factors influencing migraine recurrence during postpartum
Table 4 illustrates the factors that, upon multivariate analysis, were found to be associated with migraine recurrence following childbirth: bottle feeding was associated with recurrence within the first week (P = 0.0006), while bottle feeding (P = 0.0003) and age ≤ 30 years (P = 0.01) were associated with recurrence within the first month.
Migraine recurrence during postpartum in relation to patient characteristics and the course of migraine during pregnancy and delivery
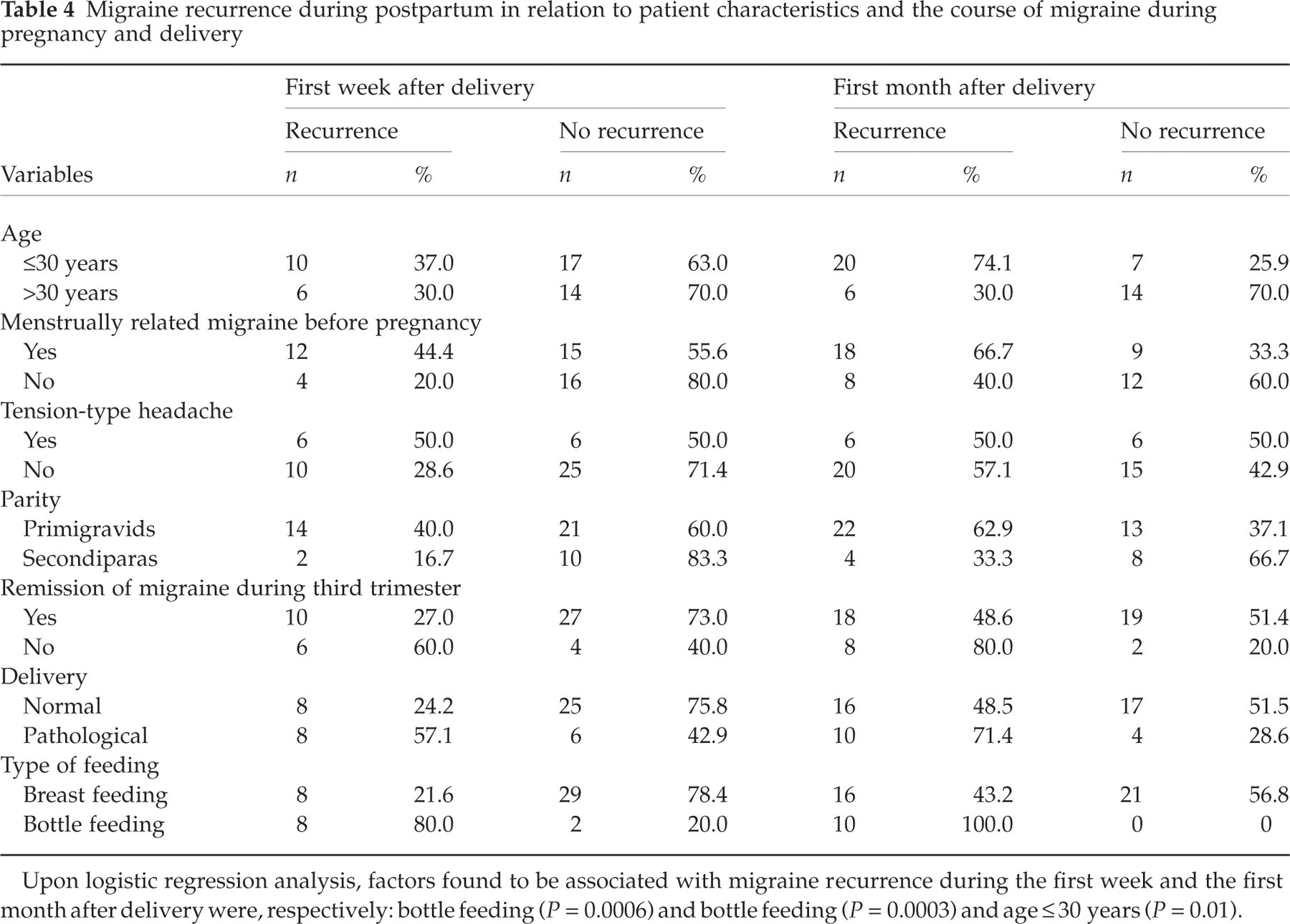
Upon logistic regression analysis, factors found to be associated with migraine recurrence during the first week and the first month after delivery were, respectively: bottle feeding (P = 0.0006) and bottle feeding (P = 0.0003) and age ≤ 30 years (P = 0.01).
Discussion
Very few studies have investigated prospectively the course of migraine during pregnancy. Chen and Leviton (16), studying 484 migraineurs drawn from a huge sample of pregnant women (n = 40 273), found an improvement in 79% of cases, while 21% of the women reported no headaches during pregnancy. However, this study has several shortcomings. Even though the paper was published in 1994, it refers to data collected (as part of a study designed to identify the antecedents of neurological problems in children) as long ago as 1959–1966. Not only did it fail, obviously, to use the IHS diagnostic criteria, but the very low prevalence of migraine (1.3%) suggests that it included only a small, and thus not representative, fraction of migrainous women. Moreover, the migraine course was assessed only very roughly: all that was established at each antenatal check-up was whether or not there had been a headache since the last antenatal check-up. At variance with all the previous studies, Marcus et al. (17), using a headache diary, prospectively monitored from the second trimester a highly selected sample (women experiencing headache at least twice a month, recruited through advertisements placed in obstetricians’ surgeries and local newspapers) of 49 primary headache sufferers, only 18 of whom were pure migraineurs, and found an improvement in only 41% of the women. The study also revealed a non-significant trend towards a greater improvement in migraineurs than in tension-type headache patients. Several factors reduce the validity of this study: the self-selection of the subject sample, the inclusion of subjects only as from the second trimester (thus excluding women experiencing a first-trimester improvement), and the small number of migraineurs recruited.
Due to the paucity and limitations of prospective studies, our results must necessarily be compared with those produced by retrospective studies (1, 3, 5–11). In these studies, the percentage of migrainous women whose headache improved during pregnancy varies broadly, from 43% (9) to 86% (10). These results could have been influenced by a number of factors: the geographical area in which the study was carried out, the type of population investigated (headache centre, obstetrics department, general population), the diagnostic criteria of migraine employed (IHS, Ad Hoc Committee, etc.), the type of migraine investigated (all the types or only MO), the definition of improvement, etc. However, of all the possible factors, a major role was played, in our opinion, by the timing of the interview: the studies performed close to delivery showed percentages of improvement – ranging from 78% (6, 7) to 86% (10) – that were higher than those found in studies carried out years after childbirth, in which the percentages ranged from 43% (9) to 67% (3, 11). It appears that the time elapsing since pregnancy biases recall, attenuating its positive effect. Our study, carried out using a more sophisticated methodology – prospective design, assessment by a headache diary – produces a percentage of improvement (87%) that is higher than the maximum values produced by retrospective studies performed close to the time of delivery, and very similar to that (86%) found by Maggioni et al. (10) in their accurate survey. It demonstrates that almost all the migrainous women derive considerable benefit from pregnancy, in terms either of improvement or true remission of their migraine. Remission was, in fact, obtained by 78.7% of the women during the third trimester of pregnancy; moreover, any residual attacks tended to be less severe, even though their duration did not alter. Furthermore, no women experienced a worsening of headache during pregnancy. Around 10% of the women were attack free throughout pregnancy.
The positive effect of pregnancy was not exerted uniformly across the trimesters: having emerged in the first trimester (when an improvement was seen in 46.8% of the women), it increased substantially in the second (producing an improvement or remission in 83.0% of women). Some further benefit was then seen in the third trimester, mainly in terms of a shift from improvement to complete remission (the remission rate rose from 53.2% in the second trimester to 78.7% in the third). Thus, the improvement was found to continue throughout pregnancy, reflecting the rising oestrogen levels. It is known from animal studies that oestrogens increase pain thresholds (18); conversely, pain threshold has been found to increase during pregnancy (19). Not only oestrogens, but also endogenous opioids increase progressively with pregnancy, reaching levels that are many times higher than those recorded in the pregravid period (20). From an antalgic point of view, pregnancy is therefore a positive state. In addition to the rise in pain thresholds due to increased oestrogen and opioid levels, a contribution is probably also made by the cessation of the sex hormone fluctuations that are responsible for cyclical perimenstrual attacks. Our study is partially at variance with the only other survey to consider attack trends in the various trimesters (10), a study in which the improvement became almost fully established during the first trimester (77% improvement/remission rate), peaked during the second (86%) and fell slightly during the third (82%).
There is very little in the literature on the course of migraine during postpartum. Stein (21) studied 71 women randomly selected from a postnatal ward during the first postpartum week. Postpartum headache developed in 37% of the subjects. This percentage rose to 61% among women with a family history of migraine and to 64% among previous migraineurs. In migraine patients, postpartum headache generally had some migrainous features, but was milder and less frequently unilateral than the patients’ typical migraine. We found a considerable rate of migraine recurrence: 34% within the first week and 55.3% within the first month following childbirth. In our patients, postnatal migraine attacks were indistinguishable from those experienced before pregnancy and more severe than those that had occurred during the third trimester. On the basis of the clinical characteristics of the headache attacks, we were able to exclude postdural puncture headache in the women who had had epidural anaesthesia for labour and cesarean section. Attacks that occurred early after delivery were probably triggered by the abrupt fall in the level of oestrogens, while later headaches may have been favoured by other factors, such as postpartum depression or the stress of adjusting to the new parental role and responsibilities.
We sought to identify the factors possibly associated with lack of improvement during pregnancy and with recurrence of migraine during postpartum. Very few attempts had previously been made to do this. Somerville (6) failed to find differences between the plasma progesterone levels (measured during the 4 weeks before delivery) of improved and of non-improved women. Lance and Anthony (1) reported greater relief in women who had had a menstrual periodicity (defined as the regular occurrence of migraine at the time of menses) prior to pregnancy, while the gender of the unborn child was not found to be correlated with the course of migraine. At variance with these authors, and quite surprisingly, we found that the occurrence of menstrually related migraine prior to pregnancy constituted a risk factor for a lack of improvement in both the first and the third trimesters. An explanation of the phenomenon may lie in our definition of menstrually related migraine, which included not only migraine occurring solely during menses, but also migraine occurring during and outside menses. This broad definition led to the inclusion of over half of our subjects in the menstrually related migraine group, and we were not able to single out the subjects affected by true menstrual migraine and describe the course of migraine in these women. Moreover, it is well known that recall bias may increase the percentage of menstrually related migraine retrospectively recorded (22). The other major factors predicting lack of improvement, this time in the last two trimesters, were a pathological course of pregnancy, and the persistence of hyperemesis during the second trimester. It is easy to understand how physical problems arising during pregnancy, generating concern and anxiety over the health of both the mother and the fetus, may cancel out the benefits normally accompanying pregnancy. We did not find differences between primigravid and multiparous women, a finding that is in keeping with the conclusions of Maggioni et al. (10).
According to the results of our study, the main risk factor for the postnatal recurrence of migraine, both early on (in the first week) and during the first month, was bottle feeding, and we can only speculate about the mechanisms underlying the unfavourable effect of this type of feeding. Women who should have withdrawn from lactation were treated pharmacologically with cabergoline. It is unlikely, however, that this drug had a negative effect: first, because it was administered in a single dose, and second, and more importantly, because previous studies have shown how other dopaminergic agonists, like bromocriptine (23) and α-dihydroergocryptine (24), have been used successfully to counter migraine. The psychological repercussions of interrupting breast feeding, inducing a feeling of inadequacy in some women, may have played an important role. However, rather than bottle feeding representing a risk factor, it can be hypothesized that breast feeding exerted a protective action. Breast feeding, in fact, increases the levels of the anti-nociceptive hormones vasopressin and oxytocin (25, 26) and contributes to successful natural bonding.
Our study has some limitations. We included only patients who had experienced at least one attack in the 3 months preceding pregnancy: this means that our sample does not cover the whole spectrum of migraine patients. Moreover, due to this choice, we excluded most patients with MA, which is typically characterized by a low attack frequency. Our results therefore apply only to MO. Although we examined all the women referred to the obstetrics and gynaecology department of a large hospital for a first routine antenatal check-up, and who thus formed a sample that might be considered sufficiently representative of the general population, our subjects were mostly primigravid (reflecting the very low Italian fertility rate), ethnically homogeneous (all were Caucasians), married, well educated and from the middle and middle–high social classes (reflecting the social milieu of Lombardy, one of Italy's most wealthy areas). Caution should therefore be applied in generalizing our results to other social settings.
In conclusion, our prospective diary-based study demonstrated a very favourable effect of pregnancy in the overwhelming majority of patients affected by MO, an effect that was more striking than that observed in almost all the retrospective studies we considered. The improvement, already evident during the first trimester, increased markedly during the second trimester, and continued throughout the third, a period of pregnancy in which almost 80% of the women were migraine free. Migraine, however, recurred during the first month after childbirth in more than half of the subjects. The main factor predicting a lack of migraine improvement during pregnancy was a pathological course of pregnancy, while breast feeding was associated with lower migraine recurrence during both the first week and the first month after delivery.
Footnotes
Acknowledgements
This study was supported by a grant from the Ministry of Public Health – RC98.