
Abstract
In spite of the fact that migraine often manifests as a familial disorder, the role of the family in migraine has not been adequately explored. In this study parent-child interactions in 20 families with a child suffering from migraine were analysed and compared with 20 healthy families and 20 families with an asthma child. The families had to solve a puzzle within a limited time. Parent-child interactions within migraine and asthma families were asymmetric, revealing a disease-specific interpersonal context in the family. Communication with the affected child in migraine families was significantly more directive, with more specific instructions and less help, towards migraineurs than with the healthy siblings. Dominance of parents and submissive behaviour of children were the main features of interactions. In asthma families interactions were more conflicting and less cooperative. This study demonstrated a specific, asymmetric, pattern of family interactions predisposing children either to migraine or asthma.
Introduction
Migraine is a biological disorder strongly influenced by environmental events (1). Stress and psychological factors play an important role in precipitation, provocation and exacerbation of migraine attacks, especially in juvenile migraine (2). On the one hand, young migraineurs were described as more tense, anxious, depressed, characterized by pronounced achievement motivation and fear of failure, high neuroticism, and frequent internalizing and externalizing behavioural abnormalities (3). On the other hand, stress was considered the most frequent precipitating and provoking agent in migraine (2, 4). Psychological therapies of migraine in childhood, such as relaxation training and biofeedback, were potentially superior to pharmacological prophylactic treatment (5).
Concerning the influences of genetic and psychosocial factors on the early development, it can be suggested that the personality of a child, his/her behavioural abnormalities, and psychophysiological reactivity to environmental events are formed first and foremost in the family (6, 7). The family is a primary agent in the socialization of environmental attitudes, and most health problems are first dealt with in the context of the family (8). Especially in younger children, the influence of the family is essential and contributes to a large degree to the development and clinical course of psychosomatic disorders (9).
In spite of the fact that migraine often manifests as a familial disorder, the role of the family in migraine has not been adequately explored. For the most part the family is at the centre of research interest when investigating the genetic contribution to migraine. Indeed, cases of migraine in the family vary between 37% and 91% in probands with migraine and between 5% and 26% in probands without migraine (10). However, genetic factors alone do not explain the development of migraine in individual cases and exacerbation of behavioural abnormalities in migraine children (1, 11). Especially migraine without aura, the most frequent form of migraine, is caused by a combination of genetic and environmental factors (10–12). However, migraine families have rarely been analysed from a psychological point of view.
The psychological role of the family in the development and clinical course of migraine in childhood can be reduced to either parenting by an adult migraineur in the family, or ‘significant others’ such as healthy parent or grandparents, or characteristics of the broader interpersonal context. Only a few studies focus on investigation of these aspects. Guidetti et al. (13) and Santucci et al. (14) performed structural interviews in clinical samples of patients and applied a number of projective and personality tests to the children and their migraine-affected mothers. He found that mothers of migraine children have a strong tendency to protect their child, restricting the child's autonomy and liberty. Moreover, both migraine children and their mothers were characterized by relatively frequent depression, where the depression in the mother was an important factor in the child's adjustment and development of emotional and behavioural abnormalities (15). These results were confirmed by Maratos and Wilkinson (16), who found, also based on clinical sample, an association between disturbed family relations and behavioural abnormalities in migraine. The proportion of parents with a marital relationship less than ‘close and positive’ was four times higher among parents of behaviourally disturbed migraine children than among those of non-disturbed migraineurs or healthy children. Migraine children, however, revealed behavioural or psychiatric disorders significantly more often than healthy controls, and the familial atmosphere in migraine families was more destructive. Ehde et al. (17) analysed college students suffering from headache and showed that migraineurs described their families as organized, structured, and controlled, and less likely to encourage emotional expression compared with headache-free controls. No differences in the family environment were found between tension-type headache patients and healthy controls. The authors concluded that there are important differences between migraine and tension-type headache with regard to the family environment and functioning, with a greater effect of the familial atmosphere on the development and exacerbation of migraine. Aromaa et al. (18) recently showed, in a large population of families, that conflicts more often led to open quarreling and sulking in the families of headache children than in control families. The tension-type headache children, however, had poorer family environments than young migraineurs.
All of these investigations demonstrated the important impact of the family on the well-being of young migraine patients and its significant role in development and exacerbation of migraine. Dominance, overprotection, and emotional over-involvement are the most typical characteristics of parental behaviour in migraine families. However, the previous studies did not analyse the familial environment directly. Questionnaire-based studies, especially with retrospective data evaluation, have a limited value compared with microanalytical observation of behaviour (19). Structural analysis of parent–child interactions provides a direct description of parenting and interpersonal context in the family (19, 20).
We employed microanalytical analysis of familial interactions in a previous study and demonstrated that migraine parents tried to exert more control over the child's behaviour during a stressful situation (21, 22). They inhibited the child's independence, gave direct and specific instructions, and punished the migraine child more often than the healthy sibling. Young migraineurs interacted with their parents less actively than healthy children or children with the attention-deficit hyperactivity disorder. These patterns of communication in migraine families were held responsible for the significantly more pronounced achievement motivation in young migraineurs, and especially for the fear of failure, which may underlie the increased sensitivity and psychological vulnerability of migraine children (3, 23, 24). The study showed that dominance is one of the most important features of parental communication with offspring suffering from migraine.
The aim of the present study was the evaluation of the relation between the familial atmosphere and the aetiopathogenesis of migraine by analysis of parent–child interactions in a stressful situation. Based on the results of the Lykaitis study (22), we chose the coding system for the assessment of interactions, which allows a more detailed evaluation of the procedural side of interaction and describes familial relations in terms of the learning theory: The Munich Training Model (MTM), developed by Innerhofer (25), investigates dominant parental behaviour. The construct focuses on parental control of the child's activities either directly or by linking changes in the consequences. A great advantage of the MTM is its practical orientation. Analysis of parent–child interactions in terms of the MTM facilitates practical recommendations on the basis of observations (25).
One of the largest methodological problems in parental interaction research and investigation of the family role in the development of disease is the choice of the control group (20, 26). The choice of the control group should help to answer the question about specificity of parent–child interactions. For this purpose two control groups – families with a healthy child and families with a child suffering from a psychosomatic disorder other than mi-graine – have to be investigated. Asthma seems to be appropriate because: (i) bronchial asthma is, similar to migraine, a paroxysmal disorder with attacks and symptom-free intervals. The quality of life and the severity of the disease usually depend on the frequency and severity of the attacks (27). The courses of the two disorders demonstrate more clinical similarities than differences and make them appropriate control groups for each other; (ii) both migraine and asthma are psychosomatic disorders. The role of psychological factors in the development and exacerbation of asthma, as well as in the precipitation and provocation of asthma attacks, is well described (28, 29). It has been even shown that parent –child interactions are disturbed in asthma families, possibly predisposing some children to development of this disorder (30, 31); (iii) genetic-epidemiological studies showed that migraine and asthma co-segregate in the family, indicating a possible common genetic background (32).
In conclusion, this study investigates parent–child interactions in migraine, asthma and healthy families in a stressful situation in order to characterize specificity of familial atmosphere which may predispose some children to different psychosomatic disorders.
Methods
Subjects
Twenty families with a migraine child, 20 families with an asthma child and 20 healthy families were included in the study. These families were recruited for a project of the German Research Foundation (Ge 500/4-1, 4-2) and took part in neurophysiological investigations described elsewhere (33). The following explicit criteria were used: (i) migraine and asthma families should have both parents and two or three children. Healthy families with both parents but only one child were eligible; (ii) couples should be married for at least 5 years and, in the case of a second marriage, the interaction with the parent-in-law, with whom the child had been living with during the past 5 years, was recorded; (iii) none of the subjects should be undergoing psychiatric or psychological treatment.
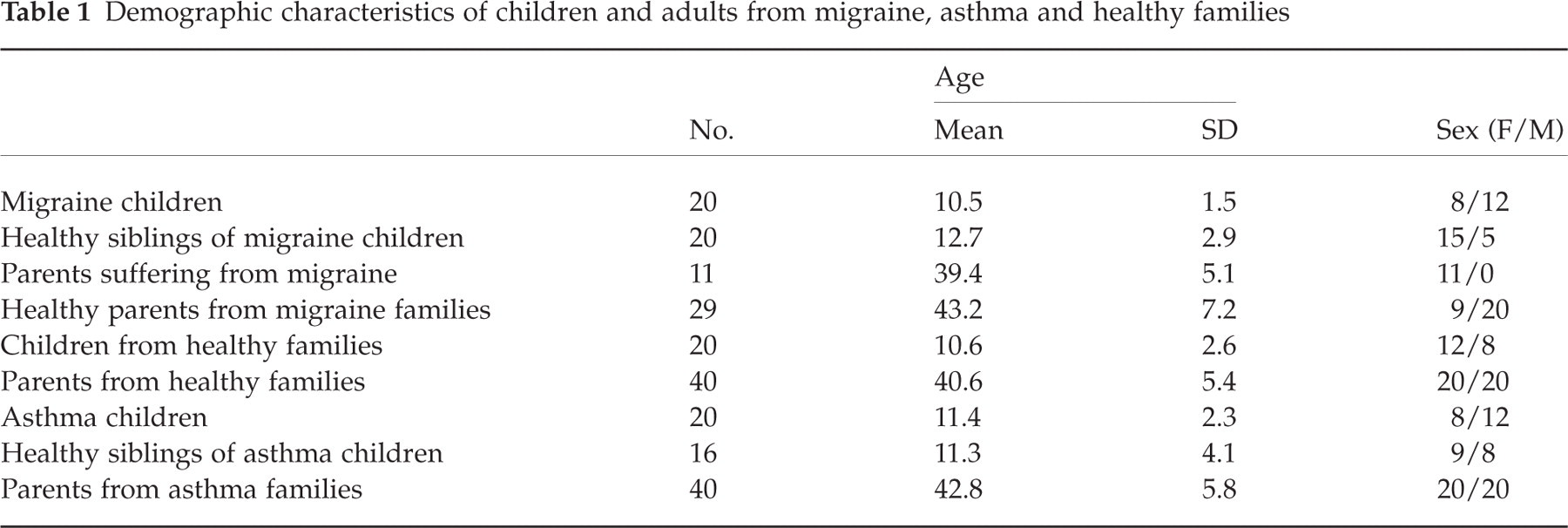
Table 1 represents demographic characteristics of the participants. Migraine, asthma children and children from healthy families as well as groups of parents did not differ significantly according to age (one-way ANOVA for children: F (2, 57) = 0.91; P = 0.408; and for adults: F (2, 76) = 0.752; P = 0.297). Healthy siblings of young migraineurs, however, were significantly older than the migraine children (t (19) = −3.716, P = 0.001). In 17 (85%) migraine families the healthy sibling was older than the migraine child. The difference between families with an older healthy sibling and younger healthy sibling was significant (χ2 = 6.036, P = 0.014). The family structure of a younger child suffering from migraine or asthma with an older healthy sibling was preferred since the older siblings had passed the critical age of illness onset and could be regarded as ‘really healthy’ and not ‘potentially ill’. Seventeen (85%) of the migraine families had such a structure. The distribution of asthma between the oldest and youngest siblings was equal (the number of asthma families with an older healthy sibling and a younger ill child was nine (52.9%)). We were not able to apply the family structure of older healthy siblings in asthma families because of recruitment problems. There was no difference between asthma children and their healthy siblings according to age (t (15) = 0.152, P = 0.881). In migraine families 60% of the migraine children, but only 25% of the healthy siblings were boys (χ2 = 6.036, P = 0.014). In asthma families 60% of children with asthma and 47.1% of their healthy siblings were boys (χ2 non-significant). There were no significant differences between migraine, asthma and healthy families in relation to the number of children in the family, socio-economic and educational status of parents, parental employment during the last 5 years, or the frequency of previous divorce. All participants were Caucasian and native German speakers. The families were paid for participation in the study.
Demographic characteristics of children and adults from migraine, asthma and healthy families
Children suffering from migraine were recruited from the Out-patient Department of the Clinic of Neuropaediatrics (University of Kiel). They were referred there by general paediatricians for consultation by a neurologist experienced in headache treatment. Headache diagnoses were made in accordance with the criteria of the International Headache Society (34). Both migraine children and adults suffered from migraine without aura (IHS code 1.1). Because of the poor reliability of the IHS criteria in paediatric migraine (35, 36), care was taken that all migraine children were characterized by (i) vomiting during migraine attacks, (ii) a family history of migraine, and (iii) severe headache with pronounced disability (inability to play or watch TV) subjectively evaluated on the visual-analogue scale (from 0, none to 10, extremely severe) between 7 and 10. Children were first diagnosed by a paediatric neurologist from the Clinic of Neuropaediatrics and then by a neurologist from the Department of Medical Psychology. Parents suffering from migraine (11 mothers) were diagnosed by a neurologist from the Department of Medical Psychology. All migraineurs were asked to keep a headache diary during the month prior to investigation. The children, and their parents, had suffered from migraine for at least 2 years. Migraine children (n = 5) and adults (n = 6) and their healthy siblings (n = 4) and parents (n = 14) suffered from episodic tension-type headache on no more than 5 days/month. They did not have any type of daily headache. Clinical characteristics and history of migraine were documented in a questionnaire completed by the migraine child and the parents. None of the migraine children or parents used prophylactic medication for at least 3 months prior to investigation.
Children suffering from bronchial asthma were either out-patients of the Clinic of Childhood Diseases (University of Kiel) or were referred to the Department of Medical Psychology by pulmonologists and general paediatricians for scientific purposes. The diagnosis of asthma was made by the referring physician and confirmed by the neurologist of the Department of Medical Psychology. Inclusion criterion was bronchial asthma for ≥ 2 years, in the absence of other chronic diseases. Clinical characteristics and history of asthma were documented in a questionnaire. None of the asthma patients used prophylactic medication for at least 3 months prior to investigation. Asthma patients (three children), their siblings (four children) and parents from asthma families (10 adults) suffered from episodic tension-type headache on no more than 5 days/month. None from the asthma families had migrainous headaches.
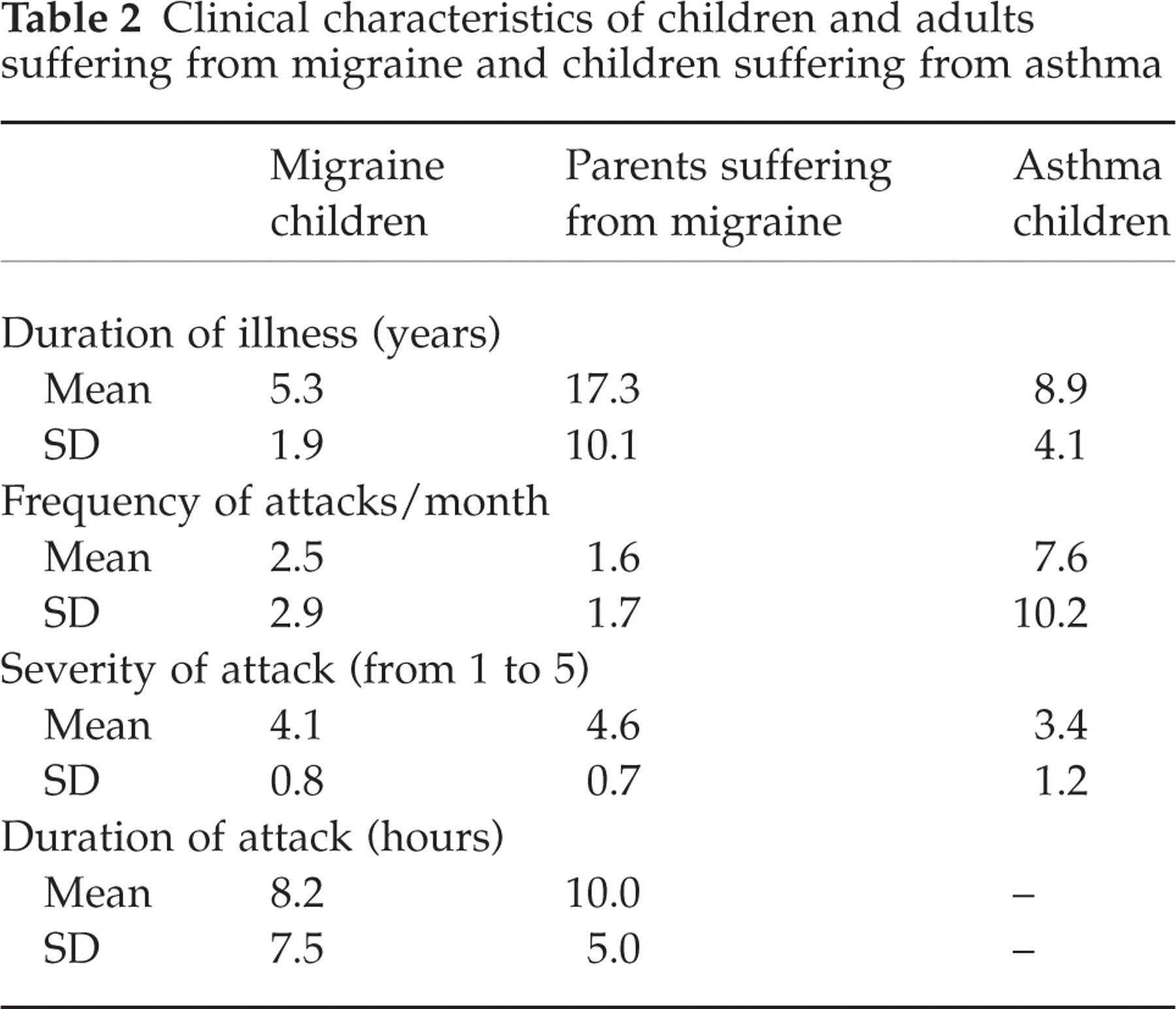
Table 2 shows clinical characteristics of the participants. The significant differences (one-way ANOVA) in clinical parameters were found between migraine and asthma children and adult migraineurs according to duration of illness (Scheffe test: P < 0.01 and P < 0.05, respectively) and between asthma children and both groups of migraine patients according to attack frequency (Scheffe test: P < 0.05 for both comparisons).
Clinical characteristics of children and adults suffering from migraine and children suffering from asthma
Healthy children and their parents were recruited from two local schools. These families were examined for neurological, psychiatric and internal disorders not only in the participants, but also in at least the past two generations. These families fulfilled the Research Diagnostic Criteria for ‘never mentally ill’ and did not suffer from migraine, neurological disorders, drug or alcohol abuse, asthma or atopic diseases in any of the analysed generations. Only three children and eight parents from healthy families suffered from episodic tension-type headache on no more than 5 days/month. The healthy families were matched for age and sex to the migraine and asthma families as far as possible.
The study was permitted by the ethics committee of The Faculty of Medicine, University of Kiel, Germany. All subjects were informed about the course of the experiment and gave written informed consent according to the Helsinki convention.
Procedure
The study was performed under laboratory conditions. All recordings were made in quiet soundproof rooms, isolated from outside disturbances. The achievement-orientated task was used for evaluation of parent–child interactions (22). Only dyadic interactions were recorded. The child had to solve a puzzle containing 75 pieces during a limited period of time with one of the parents. The following instructions were given: (i) only the child was permitted to touch the puzzle pieces and solve the task. However, the child was not aware of the puzzle picture and had to rely on the parent for information; (ii) the parent had a picture of the complete puzzle and was told to verbally help the child without showing the picture or individual pieces; (iii) the child was allowed to ask about the picture; (iv) the parent was told that the aim was not evaluation of the child's abilities, but assessment of which parent – father or mother – was able to give more effective instructions, allowing the child to solve the puzzle more quickly. The puzzles were all of identical complexity. Care was taken to randomize the sequence of participation of different family members in the task and the puzzle tasks offered. After instruction had been given, the investigator turned on a video camera and left the room for 15 min so that the conversation could be conducted in private. After this period the camera was switched off, regardless of the result of the puzzle test.
Measures
In order to measure the extent of control over problem-solving behaviour in a stressful situation, the coding system elaborated for behavioural marital therapy (Munich Training Model (MTM), Münchener Trainingsmodell, Innerhofer, 1977) was used. As described above, the verbal and non-verbal behaviour of a subject is evaluated in terms of support or suppression of the activities of the partner. Only puzzle-relevant activities were evaluated. This study concentrates only on the verbal behaviour of parents and children during the puzzle task. Non-verbal behaviour was excluded from the analysis because of poor inter-rater reliability for non-verbal codes.
Based on both the classic behavioural concept and systems theory, the coding system involves the following categories:
Goal (G)-dimension
A direct instrumental purpose-related control. This dimension includes codes requiring an immediate change of behaviour. It includes:
Specific instructions. These can be defined as commu nication sequences in which the child does what is requested, without independent behaviour. It manifests in all commands, instructions, comments and questions which provide a detailed description of expected behaviour. In the puzzle task, these instructions concern specific manipulations with particular puzzle pieces or parts of the puzzle. For example ‘Put the blue piece into the upper right corner’, ‘Turn this piece to the left’. This behaviour also means specific questions from the child (allow control): ‘This piece here?’ or ‘Does this belong to the boy?’.
Blocking of the partner's activity. Observation sequences consisting of a blockage of the partner, regardless of the success. It includes direct obstruction (‘That is completely wrong! Look at the other side’), active ignoring of an instruction (‘I don’t have to do everything you say’), active, deliberate interruption (‘Stop it! Look, it's fallen off the table again!’) or refusal of a suggestion (‘You do as I say, OK?!’).
Consequence (C)-dimension
An indirect emotional or attentional consequence-related control. Codes not requiring a change in behaviour but increasing or decreasing the probability of such behaviour in the future. This dimension can be explained in terms of operant conditioning and contains:
Positive reinforcement. Compliments, eulogy, expression of positive emotions, support through comments such as ‘Super!’, ‘You are very good at this’.
Negative reinforcement. Criticism, threats, expression of negative emotions, sarcasm, hectic, and disappointment: ‘Why don’t you understand what I mean?’, ‘Hurry up!’.
Inattention or ignorance of instruction. Comments and verbal reactions different from those required or appropriate.
Help (H)-dimension
Attempts to improve the quality of communication or understanding. It includes descriptions of the picture and general remarks on the task-solving process, or comments without detailed description of the expected behaviour (‘There are children in the left corner and various animals across the whole picture.’).
Solution (S)-dimension
An instrumental realization:
Positive or negative realization. Verbal feedback such as ‘Yes, that's right!’ and ‘No, that's wrong’.
Self-comments. Verbalizations and comments which are task-relevant, but not directed at the partner.
Directiveness (D)-dimension
Each command was either direct or indirect: ‘You have to put this piece there’ (direct command) or ‘These pieces have to be turned around’ (indirect command).
Other codes
Interruptions of the partner.
Ten minutes of each parent–child interaction were coded. This time period was chosen because some families solved the puzzle in less than 15 min.
Inter-rater reliability
The observational coders were three advanced graduate students in clinical psychology. They received > 50 h of training, feedback, and booster sessions while coding, to prevent criterion drift. Each coder used a specially written code manual developed for the process of coding. Questions concerning difficult interactions were solved together with the criterion rater (first author), after the training was finished. The raters were unaware of family status and diagnoses. Verbatim transcripts were not used during evaluation. To establish reliability, we compared the coders’ ratings with those of a criterion rater. Eight randomly selected videotapes were coded at the beginning of the study, and three tapes during the 4 months to the end of assessment (5% of the 217 tapes). Percentage agreement among the three coders was 88% at the beginning and 91% at the end of assessment for the G- and H-dimensions, 97% at the beginning and 98% at the end for the S-dimension, and 52% and 69% for the C-dimension. Fixed effect intraclass correlation coefficients (ICCs) between the raters, according to the relative frequencies of different categories, ranged from 0.87 at the beginning to 0.93 at the end of evaluation. In addition, Cohen's κ coefficients were computed, yielding a κ 0.78 (P < 0.0001) for the entire coding. For individual codes, κs ranged from 0.57 to 0.82.
Statistical analysis
There was great variation in the number of codable behaviours observed (mean number of coding units pro interaction 186.8 + 78.4, variation 112.5, minimum 32 and maximum 348). It was necessary to correct the raw frequency of each coding category by the total number of codable behaviours shown by a particular person. Therefore, the score for each code MTM was expressed as a proportion of codable units for that person. All interactional categories revealed normal distributions (non-significant Kolmogorov–Smirnov tests) and homogeneity of variables (F-test). The data variances were analysed using either the one-way ANOVA, with following post hoc Scheffe tests, or the General Lineal Model (GLM) with repeated measures. For differentiated comparisons between family members, paired samples two-tailed t-tests were performed. Multiple comparisons were adjusted according to Bonferroni.
Results
Base rate analysis
The means and standard deviations for all of the MTM codes are shown in Tables 3, 4 and 5. Since most of the variables were interrelated, a multivariate analysis of variance with the repeated measure Parents (mother vs. father) and a between-subjects group factor Diagnosis in the family (migraine vs. asthma vs. healthy) for the relative frequency of each category was performed. Neither Parents nor Diagnosis in the family exerted any influence on the codes analysed, except for the directiveness of the instructions. The following post hoc Scheffe tests with α adjustment demonstrated that parents of migraine families controlled their children more often with directly formulated sentences (such as ‘You have to put this piece …’ rather than ‘This piece may belong …’) than parents of healthy and asthma families (P = 0.002 for mothers and P = 0.004 for fathers).
Means and standard deviations of different codes in migraine families

Means and standard deviations of different codes in asthma families

Means and standard deviations of different codes in healthy families
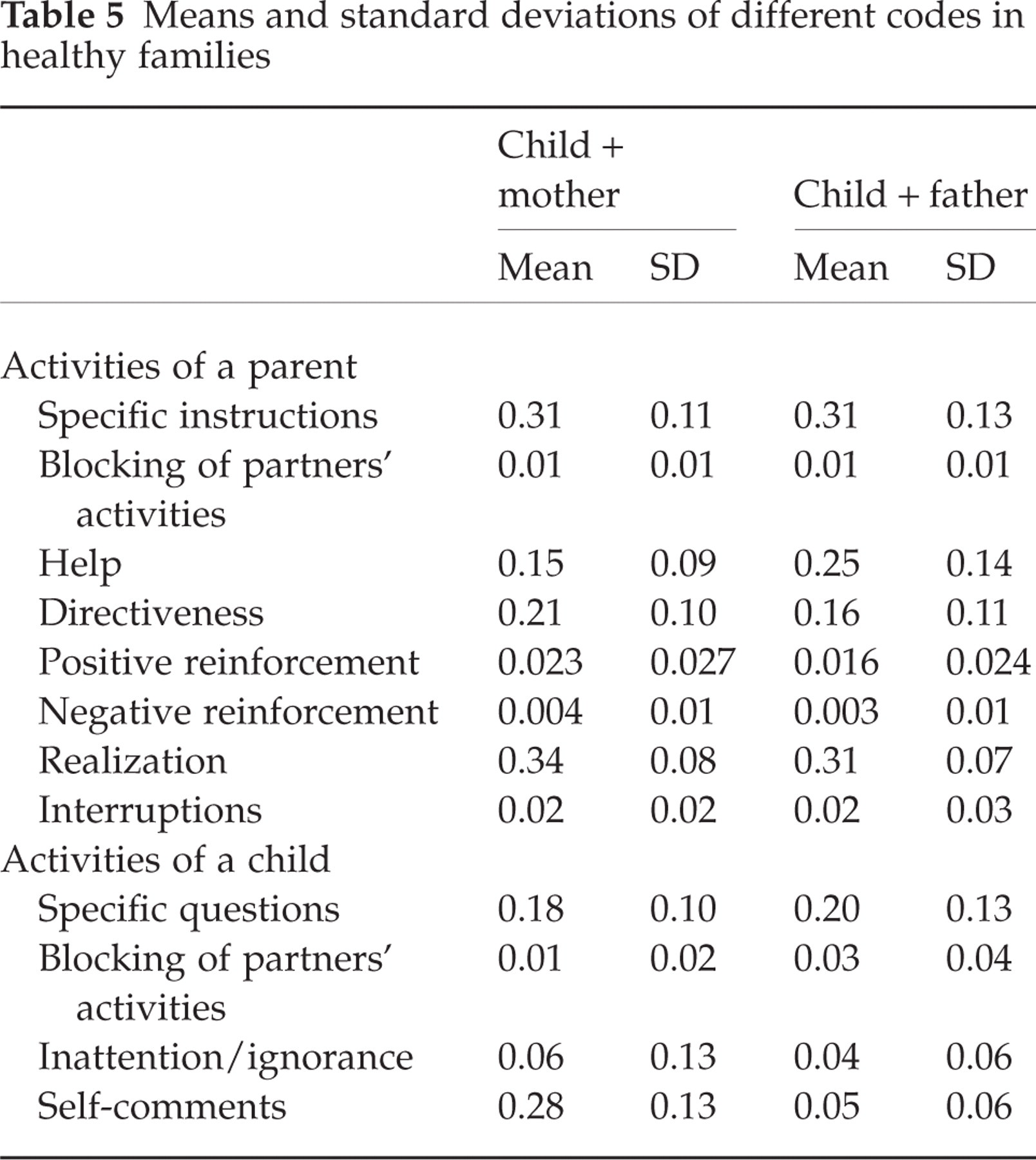
In order to evaluate asymmetry in parent–child interactions in migraine and asthma families, a multivariate analysis of variance with the within-subjects factors Siblings (interaction with an ill child vs. interaction with his/her healthy brother or sister) and Parents (mother vs. father) was performed. Parents interacted differently with the ill child compared with the healthy sibling (Tables 4, 5 and 6). Moreover, the patterns of asymmetry in parent–child interactions in migraine and asthma families differed. In migraine families there was significantly more directiveness in communication with the child (effect Siblings: F (1, 19) = 18.211; P < 0.001), as well as more specific instruction (effect Siblings: F (1, 19) = 6.418; P = 0.02), and less help (effect Siblings: F (1, 19) = 21.628; P < 0.001) towards migraineurs, compared with healthy siblings. Mothers of migraine children gave less spatial and content-related orientation than the fathers (effect Parents for help: F (1, 19) = 5.894; P = 0.025, but non–significant interaction Siblings × Parents). Moreover, migraine children often asked more specific questions about what they should do than their healthy siblings (effect Siblings: F (1, 19) = 8.610; P = 0.009). No significant differences between the interactions with a migraine and healthy child within the family were found for other parameters. No differences between interactions with the mother or father were seen (effect: Parents and interaction Siblings × Parents, non-significant for all parameters except help).
Control ratio (CR) and independence ratio (IR) calculated for parent–child interactions in migraine, asthma and healthy families

In contrast, there were no differences in directiveness, specific instruction, help or specific questions in the interactions in asthma families. However, parents of asthma families tried to block activities of their ill children and interrupted them significantly more often than the healthy offspring (effect Siblings: F (1, 14) = 10.433; P = 0.006 and F (1, 14) = 7.041; P = 0.019, respectively). Asthma children blocked active control through their parents more frequently than their healthy siblings (effect Siblings: F (1, 14) = 4.735; P = 0.047). None of the other comparisons in asthma families was significant. Moreover, the effect Parents and interaction Siblings × Parents was not significant in any of the comparisons.
In the discriminant analysis for differentiation between migraine and healthy families, using the codes as independents, the χ2 test for the first discriminate function was significant (χ2 = 23.1, P = 0.002). The first canonical correlation was 0.69. The only variables (canonical coefficient, canonical loading) discriminating between the diagnostic groups were the specific instructions of parents (0.73, 0.80) and specific questions of children (0.55, 0.52), substantially greater in migraine families. The only variable discriminating between asthma and healthy families was the blocking of partner activity by the child (0.69, 0.63). However, the χ2 test for the first discriminate function was nearly significant (χ2 = 12.84, P = 0.06) and the first canonical correlation not very strong (0.58).
In order to evaluate the extent of parent control and child independence, two ratios were computed. The ratio of control of the child's behaviour was calculated as a summation of variables representing an overwhelming dominance (imperative specific instructions, blocking of the partner's activity, interruptions) divided by the help. The ratio of child independence was assessed by the frequency of specific questions (reflecting the attempt to initiate dominant parent behaviour and give up responsibility) divided by puzzle-relevant comments of the child. Table 6 shows the control and independence ratios for all of the families with regard to a possible asymmetry of parent–child interactions. A multivariate analysis of variance with the repeated measure Parents (mother vs. father) and the between-subjects factor Diagnosis in the family (migraine vs. asthma vs. healthy) revealed a significant effect Parents (F (1, 56) = 7.715; P = 0.01) and interaction Parents × Diagnosis in the family (F (1, 56) = 3.588; P = 0.034) for the ratio of parent control. The following Scheffe tests demonstrated that the most pronounced difference appeared in comparison of the ratios from the migraine group with the healthy group for the interactions with the mother (P = 0.031).
For assessment of interaction asymmetry a multivariate analysis with the within-subjects factors Parents (mother vs. father) and Siblings (ill child vs. healthy child) and the described ratios as dependent variables was conducted separately for migraine and asthma families. It demonstrated significant effects only in migraine families, supporting the previously shown findings that dominance is a specific feature of interactions in these families. For the ratio of parent control both the effects Siblings (F (1, 19) = 10.837; P = 0.004) and Parents (F (1, 19) = 5.229; P = 0.034), as well as the interaction between these factors (F (1, 19) = 4.335; P = 0.051), were significant. The asymmetry in interaction with the mother was more pronounced (paired sample two-tailed t-test for comparison between interaction with an ill child and with a healthy child: t (19) = 2.657; P = 0.016) than with the father (t (19) = 0.821; P = 0.422). No significant differences were found for the ratio of child independence.
Influencing factors and parent–child interactions
Influence of the age of the children and the age structure of the families was analysed using Pearson's product-moment correlations (all correlations are given for interactions with the mother, the described parameters correlated in the same manner with the father). We found significant positive correlations between age and help (r = 0.35, P = 0.006 for ill child and r = 0.56, P < 0.0001 for the healthy sibling), as well as a negative correlation between age and directiveness (r = −0.270, P = 0.038 and r = −0.367, P = 0.02, respectively), and negative reinforcement (r = −0.316, P = 0.038 and r = −0.385, P = 0.014, respectively). Migraine, asthma and healthy children (from healthy families) did not differ significantly according to age (one-way ANOVA F (2, 57) = 0.91; P = 0.408). Healthy siblings of young migraineurs, however, were significantly older than the migraine children (t (19) = −3.716; P = 0.001). This was a recruitment bias. The age of the siblings was considered as an assurance for a low probability of migraine development. The use of age as a covariant in all of the variance analyses described above revealed no significant effects of age for migraine. No effect of age as a covariant was observed in asthma families.
The influence of migraine or asthma in parents was analysed using one-way analysis of variance with the factor ‘disease in the parent’ and codes as dependent variables. We were unable to compare ill and healthy parents in relation to their interaction with the children in asthma families since only one of the parents suffered from asthma. In the migraine families only mothers were affected by migraine. The analysis showed that these mothers often gave more direct and specific instruction (F (1, 18) = 6.676; P = 0.019 and F (1, 18) = 3.304; P = 0.05, respectively), and interrupted their children more frequently (F (1, 18) = 3.983; P = 0.061) than healthy mothers. This was supported by the analysis of variance with the repeated measure Siblings (migraine vs. healthy) and independent factor Disease in the parent. A significant influence on asymmetry of parent–child interaction was found for directiveness and specific instruction (effect Sibling × Disease in the parent: F (1, 18) = 9.103; P = 0.007 and F (1, 18) = 4.896; P = 0.048, respectively).
Clinical course of migraine or asthma may be related to the parent–child interaction. This was evaluated using Pearson's product-moment correlations for different codes and the clinical parameters of migraine and asthma listed in Table 2. Significant negative correlations between duration of disease and help (r = −0.547; P = 0.013 in interaction with the mother and r = −0.521; P = 0.018 in interaction with the father) and between intensity of headache and the blocking of partner activity (r = −0.501; P = 0.024 and r = −0.55; P = 0.012, respectively) were found in migraine families. In asthma families, only a negative correlation between the blocking of partner activity and duration of disease (r = −0.668; P = 0.005 in interaction with the mother and r = −0.681; P = 0.004 in interaction with the father) was observed.
Discussion
Findings of the study
The study investigated parent–child interactions in migraine, asthma, and healthy families during a stressful situation. There were no differences between the families according to features of parent–child interactions. Within the families, however, marked asymmetry between interactions with the affected child and the healthy sibling was seen.
Migraine families were characterized by strong dominance and control in interaction with the ill child. Parents of migraine children, especially mothers also suffering from migraine, limited migraine child independence by giving direct and specific instructions, rather than trying to help them to understand the puzzle with collaborative communication. Migraine children were characterized by submissive behaviour, asking specific questions and giving up responsibility for the success of the task. The interactions between migraine child and their parent were complementary, with excessive activity of the parents and passivity of the children. Communication with the healthy sibling was different: there was significantly more help and fewer specific instructions. Healthy siblings were more active, puzzled independently and asked fewer specific questions. These results confirm those of a previous study (21, 22), demonstrating dominance of parents and activities limiting child independence as specific characteristics of migraine families. Lykaitis (22) also showed asymmetry in interaction with ill and healthy siblings within migraine families, with more control and dominance toward young migraineurs. It seems likely that the relationships and role definitions within the family were very important. The migraine child enabled the parent to express dominance by being passive. It was obvious that the parent used the child for the realization of their own ideas to solve the task.
Our results support those of Guidetti et al. (13) and Santucci et al. (14), that mothers of migraine children tend to restrict the child's autonomy. Ehde et al. (17) emphasized that a rigid structure, strong organization and control were the main characteristics of migraine families. Disturbed familial atmospheres in families of migraine patients were described (16, 18). There was even a relationship between interfamilial transactions and increased achievement motivation of migraine children (22). It was proposed that the pronounced dominance and overprotection of parents in migraine families may cause passivity and fear of failure in children suffering from migraine (22). The abnormal familial atmosphere and parent–child interactions may be responsible for psychological abnormalities seen in migraine children (2, 3, 23). Excessive dominance and control in interfamilial transactions cause low self-confidence and disturbed self-esteem in family members (20). Anxiety, depression, internalizing and externalizing behavioural abnormalities are the result. We suggest that abnormal parent–child interactions contribute to the increased stress vulnerability and sensitivity of young migraine patients.
Is this pattern of parent–child interactions specific to migraine families? The analysis of asthma families also showed asymmetry, although quite different. The interaction of parents with an asthma child was more conflicting and oppositional than with the healthy sibling. There were significantly more blocking activities and interruptions towards the asthma child. Asthma children reacted with blocking to defend their independence and autonomy. The interactions with the healthy sibling were more harmonious and less conflicting. It should be emphasized that abnormal patterns of interaction were only found by comparison of ill children with healthy siblings. It seems likely that the expression of asymmetric asthma-specific familial interactions is, as in migraine families, more important for the manifestation of the disease than the individual interaction with the asthma child alone.
Although an emotion-deficient task was used for the evaluation of parent–child interaction, our results complement those from previous research on familial atmosphere and interpersonal transactions in asthma families. A number of studies demonstrated that parents of asthma children made significantly more critical remarks and offered more negative solutions than parents of healthy children (30, 31). In addition, significantly more negative verbal communication occurred with an asthmatic child than in the controls (37). The negative parental behaviour was related to the medical compliance of the asthma child and the level of IgE (37). No relationship between parent–child interactions and the severity of asthma was found (30). We suppose that criticism and blocking activities during task solving underline the conflicting atmosphere in asthma families. Stress is an important provoking agent in asthma (28, 29). Conflicting parent–child interactions, which enhance stress in the family, may contribute to the development and exacerbation of bronchial asthma in predisposed children.
It is unlikely that the extremely dominant and oppositional behaviour towards the ill child in the family occurs only following development of the disease. We can not interpret the described patterns of interactions as overprotection or emotional over-involvement as suggested by some studies (26). This, however, is only speculation since cross-sectional studies provide limited possibilities to establish causal relationships between observational phenomena. Dominance in migraine families and opposition and conflict in asthma families seem to be closely associated with these diseases. Further investigations, however, are required to study the questions about specificity and predictive value of the described behavioural patterns.
Limitations of the study and proposals for future research
The study from Lykaitis (22) and the present examination are the first investigations of parent–child interactions in migraine families using structural analysis of directly obtained observational data. We wanted to stimulate interest in the psychological evaluation of the familial atmosphere of migraine patients. This is only the first step towards empirical family-orientated therapeutic interventions by migraine. Critical analysis of the present study can help to improve the quality of further investigations in the field of interactional research.
The age of the children has a significant influence on parent–child interactions. The greater the age, the less dominance and control exerted by the parents, independent of diagnosis. This may be due to the increasing socialization and development of autonomy in adolescence (9). The role of parents decreases with increasing age of children, and the effectiveness of parental control tends to diminish in interaction with teenagers. The use of age as a covariant, however, did nor alter the results. We presume that the effect of age is not pronounced. Increased dominance was also seen in families with adolescent migraineurs. The patient and control groups should be matched for age in future studies, despite the possibility that healthy offspring may develop the disease later. Further studies of the age effect are needed, and it should always be considered.
The structure of the task was very specific. The parents had to give information and guide the child's behaviour. The children had to rely on parent information and instruction. The parents spoke and the children acted accordingly. The evaluation was based upon the quality and quantity of communication during a particular interaction. The most significant results were therefore described for the parents. The task also predisposed the parents to dominant and the children to defensive behaviour. The main feature of such an interaction is instruction (>60% of all the codes). Emotional contents were rare. This may explain why only variables related to dominance and control revealed significant results. Finally, the task represented a stressful situation. Time and achievement pressure may have artificially turned familial interactions into conflicts. A ‘video-induced’ tendency towards socially acceptable behaviour may have affected the results. More natural tasks, where parents and children are equally verbally and non-verbally active, would be of great value.
The coding system was based on the dimension of dominance and described the procedural (problem-solving) side of interaction (25). The MTM system is not appropriate for the analysis of the quality of interpersonal relationship. None of the sentences, including critical and emotionally negative, irrelevant to the process of problem solving were evaluated. According to our observations, however, the interactions with migraine and asthma children were emotionally overloaded with verbal and non-verbal expressions of the interpersonal relationship. Other systems for the analysis of interpersonal conflicts and assessment of marital and parental satisfaction have to be used (20, 38). We did not assess non-verbal behaviour, known to be more important for the definition of a relationship than the verbal content of a communication (39). Future studies should integrate a wide spectrum of non-verbal expressions in the evaluation of the familial atmosphere and their meaning for migraine and asthma.
A possible causal relationship between parent–child interactions and manifestation of a disease is a very important question and could not be answered by our study. Investigation of the efficiency of systemic therapy and consultation would help here. In case of drug treatment, abnormal familial interactions may cause resistance to the therapy and relapse following discontinuation of treatment (40). In contrast, if abnormal parent–child interactions first appear following manifestation of the disease, drug treatment would improve the familial atmosphere (26). However, longitudinal studies are the most informative for the causal relationship between family interactions and disease (7). A cross-sectional study, as presented in this paper, can only indicate the problem and initiate the search for causal relationships.
The lack of complex studies involving analysis of relationships using psychological parameters, neurophysiological changes and parent–child interactions makes the definition of the role of the familial atmosphere in aetiopathogenesis difficult. Ideally all connecting links in the sequence ‘Parent–child interaction’–‘(Neuro)Psychological features (Traits)’–‘disease -specific (Neuro)Physiological abnormalities’ have to be described in order to assess the impact and significance of interpersonal transactions in the pathogenesis.
In conclusion, the present study demonstrated specific asymmetric parent–child interactions in migraine and asthma families, providing evidence for an abnormal interpersonal context in these families. These abnormal patterns of interaction may represent one of a number of factors contributing to the disposition to migraine and asthma. Despite the inevitable constraints in clinical research within families, and the limitations, the present study suggests promising future investigations of the role of familial environment and interactions in the pathogenesis of migraine and asthma. Moreover, the results of the study show that the family-orientated interventions may reduce frequency and severity of migraine or asthma attacks and help family dynamics, and that the efficacy of systemic approaches has to be investigated in the future. The causal relationships between familial atmosphere, genetic milieu, as well as psychosocial consequences of migraine in the family have to be clarified in further studies.