
Abstract
The aim was to assess the prevalence ('life-time') and manifestations of exertional headache and to validate some of the clinical diagnostic criteria. This study is part of the Vågå headache epidemiology study, where 1838 18-65-year-old dalesmen were personally examined in a ‘semistructured’ interview. With the criteria used, the prevalence was 12.3%. There was a slight but significant female preponderance (F/M ratio 1.38). There was a mixture of short- and more long-lasting attacks. Attacks followed long-lasting and strenuous effort/exhaustion. The precipitation mechanisms differed essentially from the cough/sneezing type of provocation. Blinded recheck of records (n = 100) as well as recheck of dalesmen (n = 41) showed high k values. The clinical manifestations differed essentially from Rooke's (1968) description (that mainly dealt with the ‘cough headache’-type). The present findings were similar to those in Pascual's description of exertional headache from 1996.
Keywords
Introduction
Benign exertional headache (EH) seems to be one of the neglectfully treated headaches. This, to some extent, pertains to the characteristics of the headache: EH typically occurs with rather long intervals, has a self-limited course, and is generally a benign headache of moderate intensity. Even after a few episodes the cause of the single episodes will usually be obvious to most sufferers. As a consequence, the consultation rate is low. Even headache physicians are probably only rarely consulted by sufferers. Unless specific questions are being asked, headache of this type probably mostly escapes detection, even in population studies. Descriptions of this headache have been given, some decades ago (1). The attacks have generally been supposed to be rather short-lasting (1, 2). However, also a ‘prolonged’ variety has been described (3, 4).
EH has also been part of epidemiological studies (5, 6), using International Headache Society (IHS) guidelines (7) and with direct patient contact, not only questionnaires.
The Vågå study of headache epidemiology also addresses the prevalence of EH (for an outline of the design, see (8)). Various clinical manifestations, in particular the precipitation mechanisms, will be dealt with, as will the results of control studies.
Materials and methods
The study was conducted in the commune of Vågå in the mountainous heartland of southern Norway, during a 2-year period ending in October 1997. The topography and population of the commune, as well as an outline of the design of the study, have recently been described (8). Of the target group, 1838, or 88.6%, went through the programme (Table 1). In 79.3% of the target group questions about EH were asked. Of those questioned about EH, 840 were females and 806 males; the ratio between females and males was similar to that in the total cohort (9) (Table 1).
Study population – demographic data
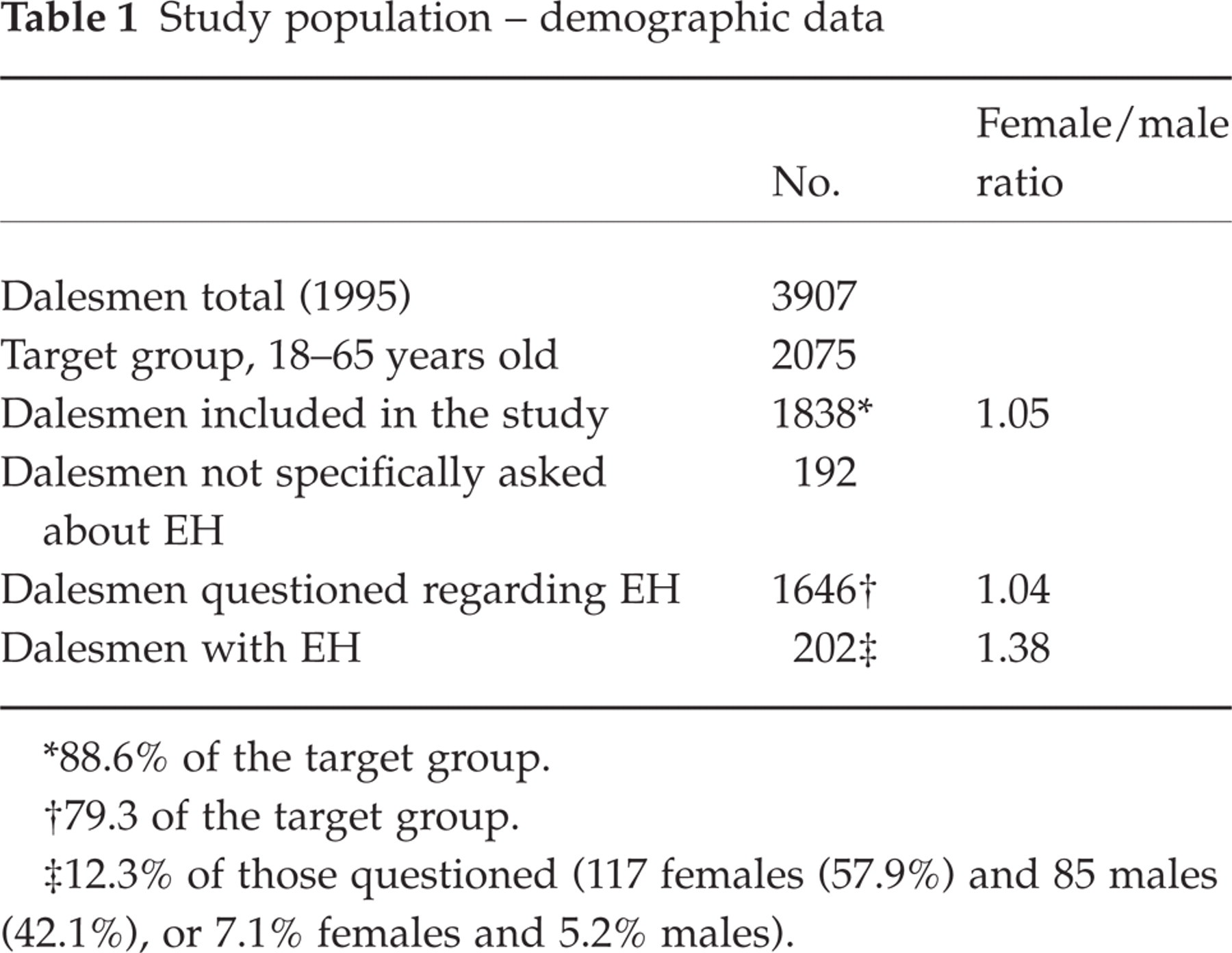
∗88.6% of the target group.
†79.3 of the target group.
‡12.3% of those questioned (117 females (57.9%) and 85 males (42.1%), or 7.1% females and 5.2% males).
Only dalesmen with definite EH were included and not those with a probable/questionable EH. The principal author was particularly careful in exploring whether genuine head pain was present, and not just a pounding sensation or neck pain. The examination was based on a questionnaire, and the questioning was carried out by the principal investigator (O.S.). The dalesmen were not even allowed to see the questionnaire (8, 9). However, deviations from the main procedure occasionally had to be allowed. The study can therefore probably best be characterized as a ‘semistructured interview’. A thorough clinical examination of head/neck and a short-version neurological examination were included. If medically indicated, a long-version neurological examination was carried out (8).
In general, the diagnostic guidelines of the IHS were followed. In this study, short-lasting and long-lasting attacks of EH will be treated as a whole, because no distinction has been made between these subgroups by the IHS (7). (At the end of this study, some guidelines will be mentioned briefly (Table 7).
Clinical characteristics of EH, ‘benign exertional headache’ (1), vs. cough headache

∗To be reported elsewhere.
†Uni/bilaterality is difficult to extract from Rooke's report (1). What seems certain is that unilaterality specifically is mentioned in 35% of the cases.
Cough headache and headache associated with sexual activity
It was planned to include cough headache in this study, on line with EH. It was soon decided, however, that this headache may not be suitable for study in a retrospective way in this setting. Cough headache was found probably to have been an integral part of coryza/flu/sinusitis episodes in several dalesmen. To discover, occasionally decades afterwards, whether in addition it had appeared outside such episodes was hardly worthwhile. This field was therefore not explored any further. Those who spontaneously reported cough headache will be mentioned in this study.
Headache associated with sexual activity was also to be asked for routinely, according to the study protocol; this headache was, however, systematically asked about only in a few dalesmen. The main reason for the decision to discontinue this search was the sensitive nature of the item. In a small society, a negatively loaded focusing on intimate, sensitive matters could have a repercussions on the whole study. In the rest of the study, only occasional dalesmen confided such information spontaneously. These cases will be mentioned in this study.
Results
Prevalence of EH and gender ratio
EH was present in 12.3% of the interviewed dalesmen (Table 1). EH thus seems to be a frequently occurring headache. This figure should be regarded as a lifetime prevalence, but memory deficiency may have influenced the result. A cross-sectional estimate will be relatively meaningless, since frequently relatively few episodes had been experienced, during a limited period, and in the distant past. There was a moderate but clear female preponderance among those having EH (Table 1), the female/male sex ratio being 1.38. This sex ratio differs significantly from unity (P = 0.03, binominal test exact) and from the sex ratio among those not having EH (P = 0.04, Fisher exact test) (Table 1).
Duration of pain episodes
The prevalence of EH naturally depends heavily on the definition of duration of such episodes, whether, for example, adopting the definition of Rooke (1) or that of the IHS (7), in other words ‘minutes’ (1) or up to 24 h (7). A total of 174 dalesmen gave information on this. In the present study, there was a spectrum from ‘short-lasting’ to ‘long-lasting’ attacks. Virtually all present cases, nevertheless, seemed to fall within the boundaries of 5 min to 24 h, in accordance with the IHS guidelines. These limits were therefore used in the present study. (The upper border may actually be a little hazy.)
Age of onset
Information regarding age of onset was provided by approximately 25% of the affected individuals. Among these, onset seemed to be significantly more frequent prior to 30 years (n = 40) than after 30 years of age (n = 15) (Table 2). The mean age of onset would be somewhere in the 20s, but there was justification for pinpointing it more exactly, given the rather imprecise nature of the available data.
Age of onset

Intensity of pain
Intensity of pain was found to be within the categories ‘mild’, ‘mild–moderate’, ‘moderate’, and ‘moderate–severe’. Approximately half fell within the categories ‘mild’ and ‘mild–moderate’. Only approximately 1/5 claimed to have ‘moderate–severe’ headache. A few dalesmen made a comparison with coexistent headache, or described the situation in other terms, as detailed in Table 3. This description tends to show that in exceptional cases EH may be intense. Some dalesmen were forced to give up sports activities because of these complaints (Table 3). Only a couple had consulted their physician because of EH.
Intensity of head pain – comparisons with other headaches, etc.

Four had to give up participation in athletics due to EH.
Precipitating factors
EH had in general been experienced after various types of hard, strenuous, and protracted physical activity. The common denominator seemed to be considerable effort over extended time. The headache then announces it presence gradually and insidiously in the late part/end of the exercise. Most of those affected had apparently experienced a multiplicity of precipitation mechanisms. However, a number of dalesmen (n = 26) spoke convincingly about one specific precipitating event, depending upon individual habits/hobbies. These activities involved various types of competition and other types of exhaustion (Table 4). Avoiding such activities would discontinue the tendency to attacks of this type. It is noteworthy that none of the generally mentioned precipitation mechanisms, nor the specified mechanisms in Table 4, necessarily had anything to do with the Valsalva manoeuvre or awkward neck movements – at least at face value. There were a couple of exceptions to this; vide infra. Headache associated with sexual activity and swimming might have a faint or more overt relationship with Valsalva manoeuvres.
Specified provocation mechanisms
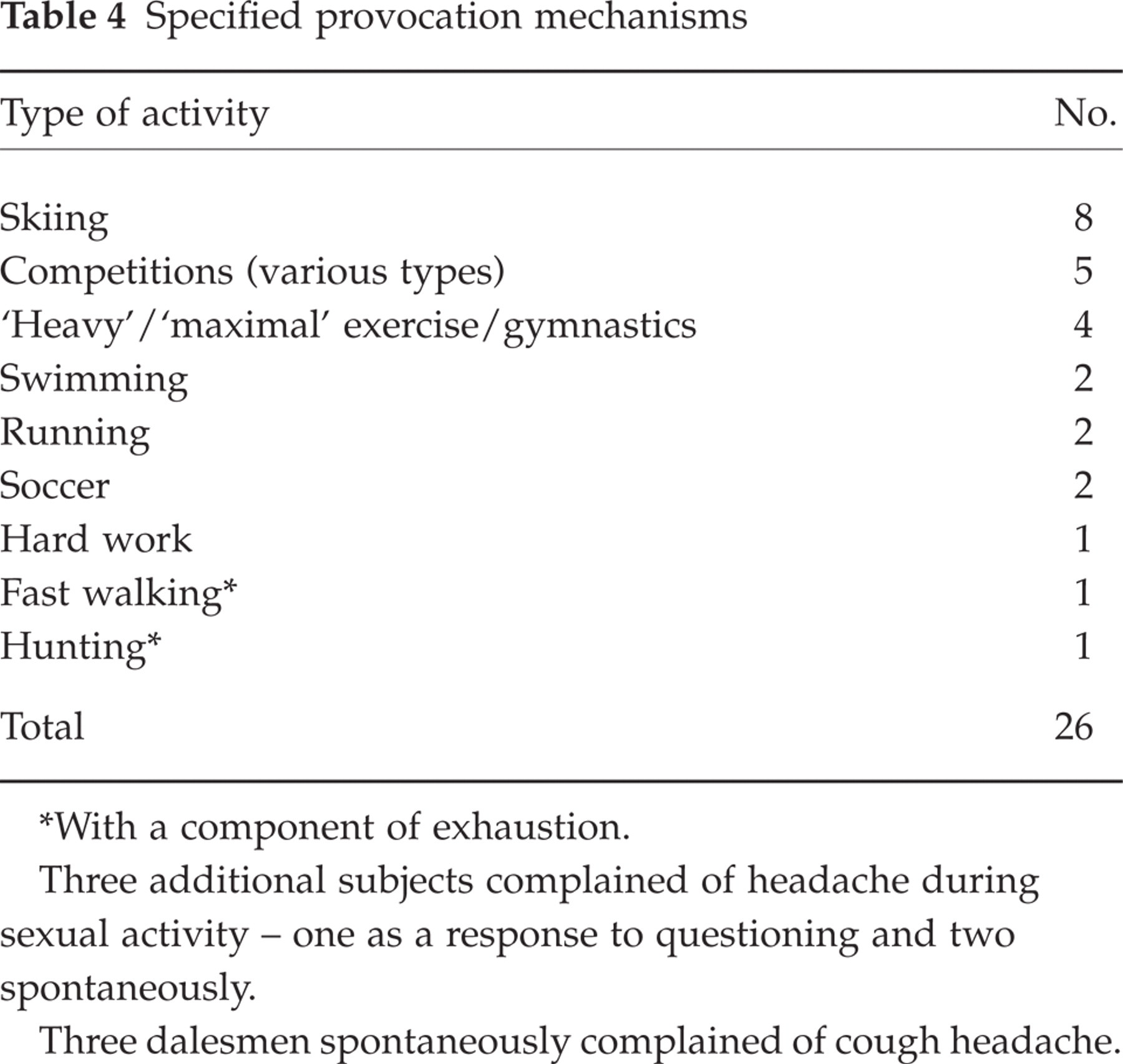
∗With a component of exhaustion.
Three additional subjects complained of headache during sexual activity – one as a response to questioning and two spontaneously.
Three dalesmen spontaneously complained of cough headache.
Three dalesmen complained of headache associated with sexual activity. One belonged to those asked regarding headache associated with sexual activity (see Materials and methods), and two complained spontaneously (Table 4). Although this figure clearly is a minimum one, headache associated with sexual activity may seem to be markedly less frequent than EH.
One dalesman had to give up swimming in his youth because he suffered from headache whenever he came into contact with water of swimming pool temperature. Later in life this tendency totally disappeared. However, he suffered from rather marked headache associated with sexual activity in late adulthood, causing some anxiety as to underlying disease. He also had EH with rather heavy attacks, lasting several minutes, and he suffered from cervicogenic headache.
Cough headache was spontaneously mentioned by three dalesmen (Table 4). This should be regarded as a minimum figure.
In connection with precipitation, it should be mentioned that two dalesmen claimed that as teenagers they had experienced that there was one specific movement that would bring about an aggravation of an already ongoing attack of EH – bending forwards: one woman at present (i.e. at 35 years) has a mild tension-type headache. The other, a male of 31 years, a classic migraineur, had had much worse migraine attacks when young than now. The EH was also more severe as a youngster, and he did not feel completely recovered even the day after an attack (Table 3).
EH among latecomers
Two months after the study another 29 dalesmen were included. Among these, there were four (>13%) with EH. The prevalence of EH among the latecomers accordingly seemed to be of the same order of magnitude as in the entire cohort. The prevalence would therefore probably not have changed appreciably had the study been extended.
Validation of the criteria for EH
In the present context, there was no limitation as regards duration. When based on the previously specified premises (7), the following results were obtained.
Recheck of records
Records of 100 dalesmen were checked in an entirely blinded fashion by one of the authors (O.S.). The questionnaires were blinded as regards name, sex, family history, and occupation (8, 9). There was a complete concurrence between the results in those questioned at the two examinations, as detailed in Table 5.
Recheck of records (n = 100)
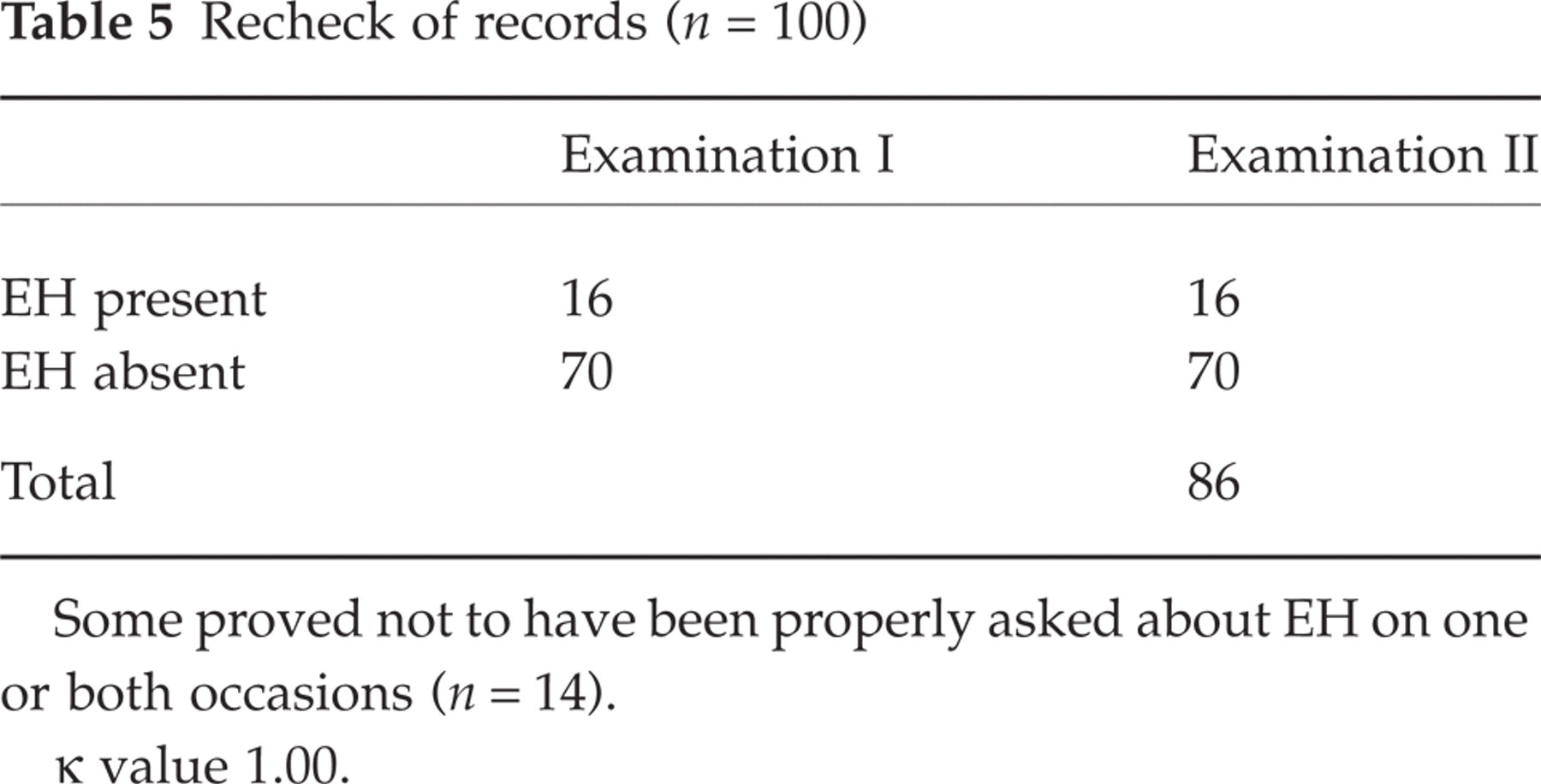
Some proved not to have been properly asked about EH on one or both occasions (n = 14).
κvalue 1.00.
Re-check of dalesmen
In a second, separate study, 41 dalesmen were re-checked (by O.S.) in an entirely blinded way. The selection of individuals for this part of the study and other details have been described elsewhere (8). The two examinations were many months apart, so that the investigator had no possibility of remembering any details of the case history. The concurrence between the results was adequate (Table 6). Unfortunately, there were few dalesmen with EH in this selected group.
Recheck of dalesmen (n = 41)
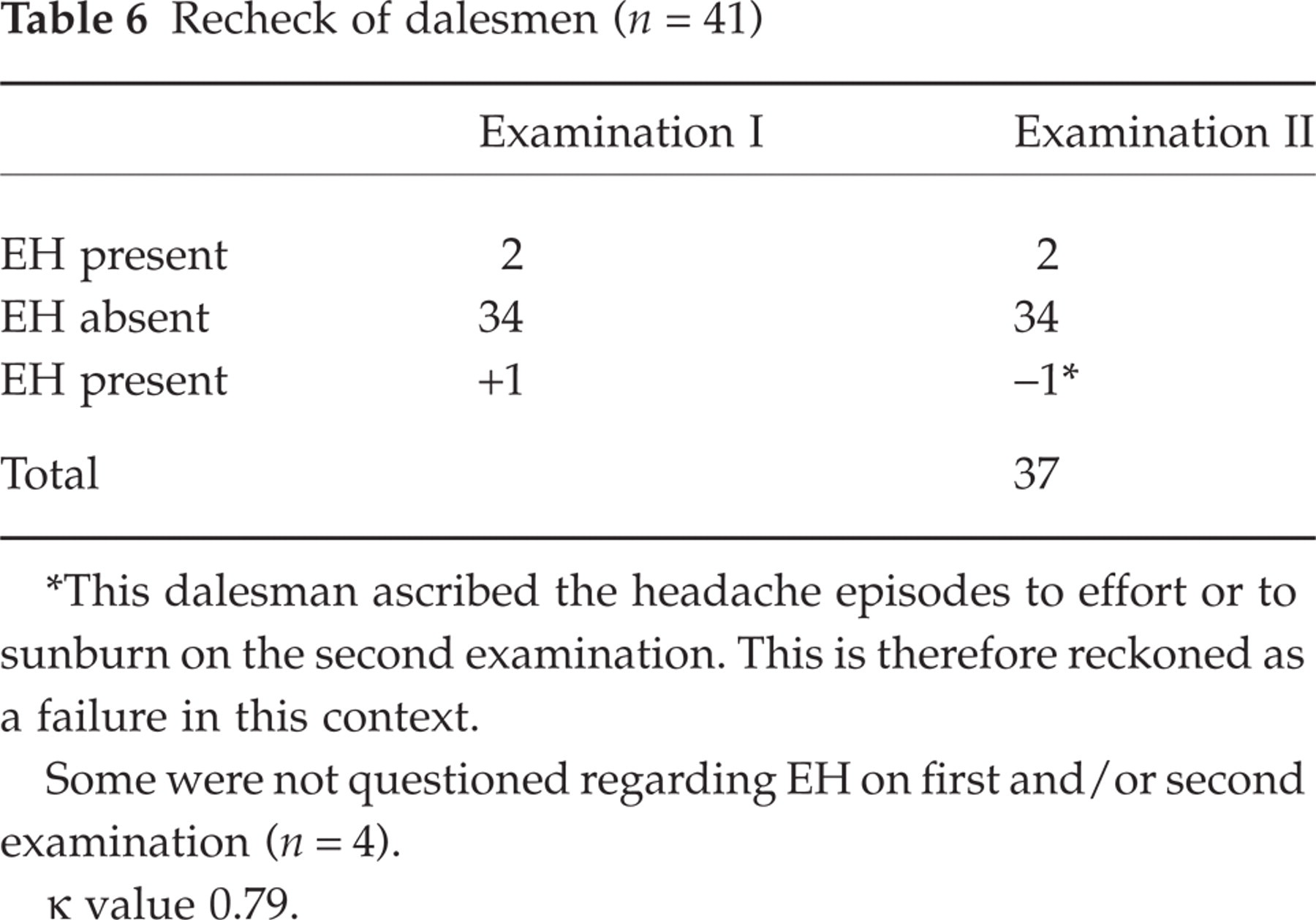
∗This dalesman ascribed the headache episodes to effort or to sunburn on the second examination. This is therefore reckoned as a failure in this context.
Some were not questioned regarding EH on first and/or second examination (n = 4).
κvalue 0.79.
Discussion
The prevalence of EH
In the present study, EH was found in 12.3% of cases. EH has previously been considered a ‘relatively rare condition’. Rooke found seven cases per year in a hospital setting (1). The fact that Rooke's study was carried out prior to introduction of the IHS criteria hampers a direct comparison with our data. The strictness of his criteria, with, for example, brief duration, may by itself have led to some limitation in sensitivity. Proper epidemiological studies of EH are scanty: a direct questioning technique was used in the Porto and Copenhagen studies (5, 6). The Copenhagen study (6), in keeping with the guidelines of the IHS (7), distinguished between benign EH, cough headache, and headache associated with sexual activity (with lifetime prevalence 1% in all three). The Porto study showed an EH prevalence of 0.2%. It does not mention cough headache, but mentions headache associated with sexual activity (apparently no cases found, quadro III, 3a (5)).
These figures are in glaring contrast to the present results with a lifetime prevalence of 12.3%. All three studies have been based on IHS criteria. The discrepancy between the two previous results and the present one is so prominent that it can hardly be ascribed to chance alone: it is most likely brought about by methodological differences.
A similar discrepancy was recently documented for ‘jabs and jolts’ syndrome/idiopathic stabbing headache; the findings in the previous studies, i.e. 2% (6) and 0.2% (5), respectively, contrasted with that of 35.2% in our study (9). The latter discrepancy can probably be ascribed to differences in design/questioning techniques. Unless specific questions are being asked, information about such relatively unimportant headaches will probably be swamped by the information load concerning the major headaches. It is suspected that such circumstances may underlie the discrepancies concerning the EH findings: the emphasis in the two other epidemiological studies (5, 6) has probably been on major headaches, possibly with less attention paid to EH. In the present study, specific questions concerning EH were asked. However, the validation studies represent no absolute guarantee against a systematic misconception of some of the factors that make up such a diagnosis. What is mainly tested in the control studies is the consistency with which the investigator uses his own criteria, but then these criteria should preferably be in congruity with the ‘official’ ones.
The specifics of EH according to Rooke's contribution (1), compared with the present reported picture
It is readily seen that for the first five points there is a clear discrepancy between the Rooke picture (1) and the present one (Table 7). In our series, the onset occurred insidiously after protracted effort, whilst Rooke (1) emphasized the abruptness of the onset. This difference seems crucial (Table 7). The differences between Rooke's and the present picture as to gender ratio and duration of attacks also seem crucial. It is also striking that the precipitating events seem to differ in the two pictures. Moreover, the discrepancy as to age of onset between the present figures, as presented in Table 2, and Rooke's findings (1) is striking. Rooke found a doubling of cases with age of onset> 40 years, compared with < 40 years vs. 5 of 55 > 40 years in the present senes (P < 0.0001, binomial exact test).
EH in principle seems to be a bilateral headache. Also Pascual et al. (11) state that it is bilateral. Unilaterality may seem to be one of the causes why EH cases are reported separately (12).
The difference between Rooke's picture and the present one all in all seems fundamental. Have we been studying the same clientele?
Nature of exertional headache
The nature of the provocation mechanism is probably fundamental. What Rooke and Tinel (13) understood by exertion is listed in Table 8. It cannot be disputed that all the specified, solitary conditions (1) represent some type of physical activity – a movement away from the position/state prevailing at the moment. But are the factors otherwise homogeneous? In terms of physical energy spent totally, as well as per time unit, they seem to differ widely.
Provoking factors in various EH studies
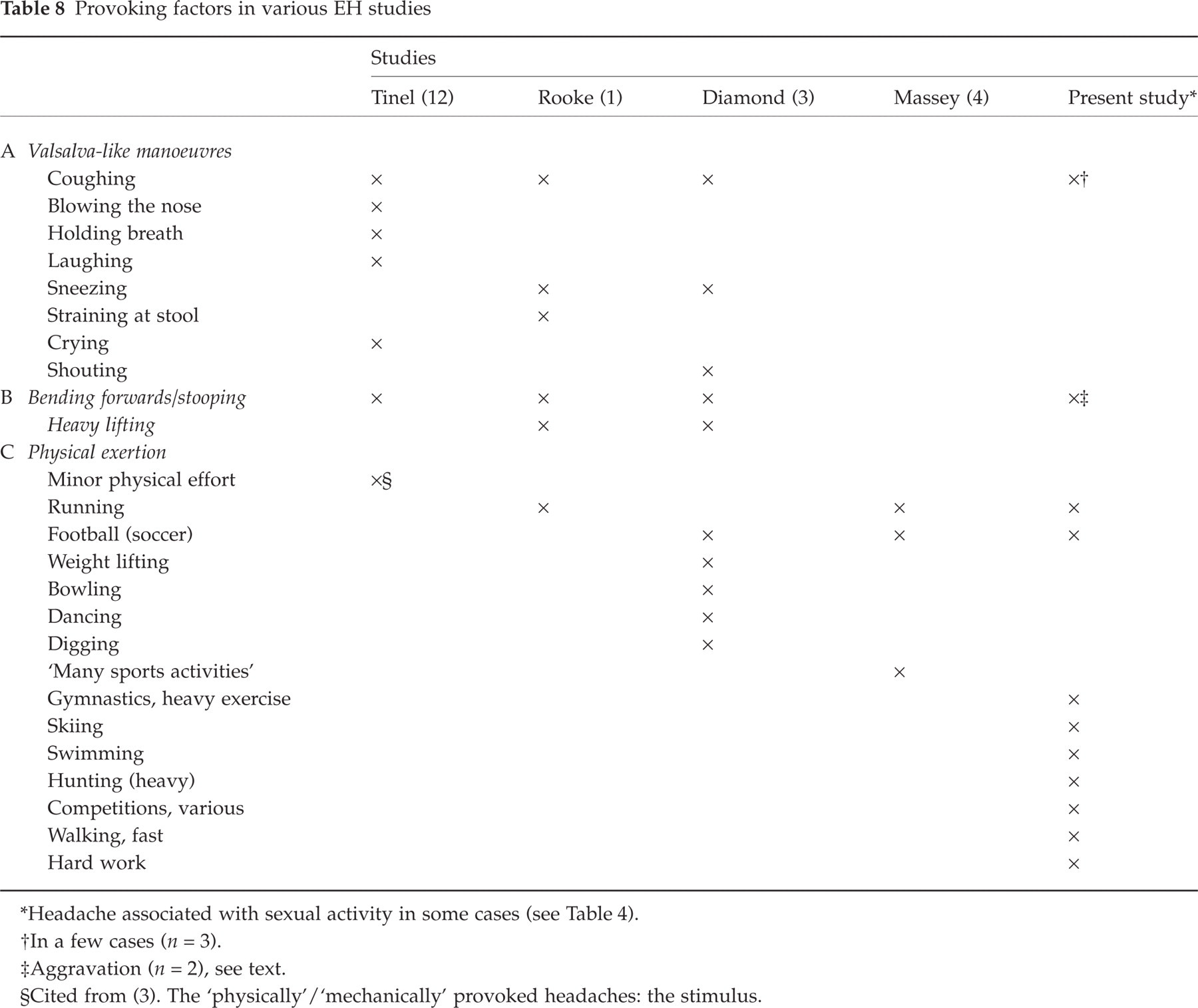
∗Headache associated with sexual activity in some cases (see Table 4).
†In a few cases (n = 3).
‡Aggravation (n = 2), see text.
§Cited from (3). The ‘physically’/‘mechanically’ provoked headaches: the stimulus.
The stimuli mentioned by Rooke (1), may seem to fall into various categories (Table 8): (i) changes in intrathoracic pressure/Valsalva-like mechanisms; (ii) mechanical factors related to the cervical spine – bending forward/stooping; (iii) general physical effort.
Three of the specific factors mentioned by Rooke (perhaps more) (1) may seem to involve Valsalva manoeuvre features (Table 8). In terms of energy spent, ‘running’ and ‘heavy lifting’ (1) may, if continued, be in a separate class. The bending forwards is most difficult: it may have to do with Valsalva-like mechanisms and with changes in intracranial pressure and abnormalities around the foramen magnum. But it may have to do with cervical spine mechanisms as well. Bending forwards or stooping are well known provoking mechanisms, not only in cervicogenic headache, but also in the variety of chronic paroxysmal hemicrania that is characterized by mechanical precipitation of attacks (14).
Diamond (3) split his patients into two groups with regard to provoking factors: those with physical effort/excessive exercise (1/3) and those with a combination of the latter and a Valsalva manoeuvre (2/3). In Massey's cases (4), the provoking factor undoubtedly was physical effort (Table 8). In our study, coughing was not specifically searched for as a precipitating mechanism.
For the cases of Massey (4) and the present ones and to a large extent for those of Diamond (3), the term ‘exertional headache’ would therefore probably be a well-chosen, valid term. Long-lasting exhaustion/physical hardship was the decisive factor. The same cannot be said about the content that Rooke (1) gave the term. Most of the exposures were brief (e.g. sneezing, coughing). The common denominator in his cases generally seems to have been Valsalva manoeuvre-like activities, leading to abrupt responses – the cough headache type of disorder. It is striking to what extent the studies of Tinel and Rooke are coupled with the ‘upper part’ of Table 8, while in particular the present study is linked with the ‘lower part’. What Rooke depicted generally seems to be very similar to what is now covered by the designation ‘cough headache’, as outlined by Pascual et al. (10), for example. There is apparently an almost complete consistency between the two pictures described by Rooke as exertional headache and Pascual et al.'s cough headache (Table 7). The conclusion therefore seems inescapable that what Rooke in all probability mainly described was ‘cough headache-type’ and not ‘effort/exhaustion headache’.
The vast difference between Rooke's series (1) and our own is therefore probably not only due to a difference in the basic populations from where the individuals are drawn – hospital population vs. grassroots level population. To a large extent, probably the selection process as such is to be blamed: the extraction criteria probably have been at variance. If this assumption is correct, then one cannot a priori expect variables like sex ratio, duration of the single attack, localization of attacks, and age of onset to be congruent in the two series.
Unfortunately, this failure to define EH properly in the early stage may in fact have delayed – if not directly obstructed – further progress in this field. Pascual and co-workers (11) apparently had the same opinion, since they stated that Rooke has created enormous confusion in this field by not distinguishing between headache provoked by short-lasting exertion, like cough, and long-lasting ones, like running (11). One can probably not expect a long-lasting headache, whether ‘migrainoid’ or not, regularly to follow coughing. In all probability, cough headache differs essentially from EH, as claimed by the IHS (7). It was only after we had reached our own conclusion on the Rooke provocation mechanisms that we became aware of Pascual et al.'s work (in Spanish) (11).
The stimulus in the provoked headaches will in future probably have to be defined in a given context. We will return to the symptomatology of EH after having dealt with so-called ‘prolonged’ EH (elsewhere).
Footnotes
Acknowledgements
We are indebted to GlaxoSmithKline of Norway for generous support in all phases of the investigation. The authors are also grateful to the personnel at the Vågå Health Centre at Vågåmo for their aid. Last, but not least, we thank the inhabitants of the Vågå commune for their collaboration.