
Abstract
Fatigue is a common symptom frequently reported in many disorders including headaches, but little is known about its nature. The objective was to determine the prevalence of fatigue in chronic migraine (CM) patients, to define its subtypes and its relationship with other conditions comorbid with CM. Sixty-three CM patients were analysed. The Fatigue Severity Scale (FSS), the Chalder fatigue scale and the CDC diagnostic criteria for chronic fatigue syndrome (CFS) were used. Fifty-three (84.1%) patients had FSS scores greater than 27. Forty-two (66.7%) patients met the CDC criteria for CFS. Thirty-two patients (50.8%) met the modified CDC criteria (without headache). Beck depression scores correlated with FSS, mental and physical fatigue scores. Trait anxiety scores also correlated with fatigue scales. Women had higher FSS scores than men, P < 0.05. Physical fatigue was associated with fibromyalgia, P < 0.05. Fatigue as a symptom and CFS as a disorder are both common in CM patients. Therapeutic interventions include a graded aerobic exercise program, cognitive behavioural therapy and antidepressants. Identification of fatigue and its subtypes in headache disorders and recognition of headaches in CFS patients has implications for the pathophysiology, diagnosis and treatment of these disorders.
Introduction
Fatigue is a common symptom (1), but its prior lack of definition and subjective nature made it difficult to study. It is a symptom of many disorders including cancer (2), HIV (3), fibromyalgia (4), depression (5), sleep apnoea (6), multiple sclerosis (7), systemic lupus erythematosus (8) and, by definition, chronic fatigue syndrome (9). Fatigue can be disabling since it interferes with activities of daily living and the patient's quality of life (10) but little is known about its causes and pathophysiology.
In clinical practice, terms such as sleepiness, tiredness, generalized weakness, loss of strength, and loss of interest are often confused, and used to represent fatigue. In an attempt to increase clarity, fatigue has been separated into mental and physical subtypes (11).
Chronic migraine (CM) is one of the chronic daily headaches (12). It is common in the general population(2%) (13) and very common in headache clinics (40–65%) (14, 15). CM is a complex and difficult to treat disorder. It is comorbid with depression, anxiety, acute medication overuse, insomnia and fibromyalgia (16).
Fatigue is common in headache patients (17, 18), but it has never been studied in a CM population. Spierings & van Hoof (18) found fatigue in 70% of headache sufferers, and rated the intensity of their fatigue significantly higher than controls. Little is known about fatigue in headache patients.
The object of our study was to determine the prevalence of fatigue in CM patients, to better define its subtypes and its relationship with conditions comorbid with CM.
Patients and methods
We enrolled 63 CM patients from the Neurological Department, Headache Clinic, Federal University of São Paulo, seen between February and November, 1999. Neuroimaging (CT scans), physical and neurological examinations were normal in all cases. CM was diagnosed according to Silberstein and Lipton's 1996 criteria (Table 1 ; 19); secondary causes of daily headache were excluded. FM was diagnosed according to the 1990 diagnostic criteria established by the American College of Rheumatology (Table 2 ; 20). The Fatigue Severity Scale (FSS) (21) (cut-off of 27 defined fatigue) and the Chalder fatigue scale (11) (Likert scoring) (22) were used. The Chalder fatigue scale has two parts, physical and mental fatigue. Items related to mental fatigue included difficulty concentrating, problems thinking clearly, difficulty finding the correct word and memory problems. Those related to physical fatigue included tiredness, need to rest more, sleepiness, drowsiness, lack of energy, and less strength in muscles or weakness.
Diagnostic criteria for transformed migraine (Silberstein et al. 1996; 19)

The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia (20)

∗Digital palpation should be performed with an approximate force of 4 kg. A tender point has to be painful at palpation, not just ‘tender’.
The CDC diagnostic criteria for chronic fatigue syndrome (CFS) were used. We also applied a modified CDC criteria not considering headache as part of the symptoms. Beck depression inventory (BDI) (23) and the trait and state anxiety inventory (TSAI) (24) were also used. Scores were correlated to the diagnosis of FM, insomnia, presence of disability, age, sex, pain intensity, acute medication overuse, depression and anxiety scores.
We ascertained age, sex, previous migraine history, number of years with daily headaches, pain intensity, acute medication overuse, insomnia and disability. Pain intensity was evaluated on a scale of 0–10. Acute medication overuse was defined according to Silberstein's diagnostic criteria (19). Disability was evaluated based upon the patient's judgement of whether or not the headache interfered with routine daily activities.
The one-way
Results
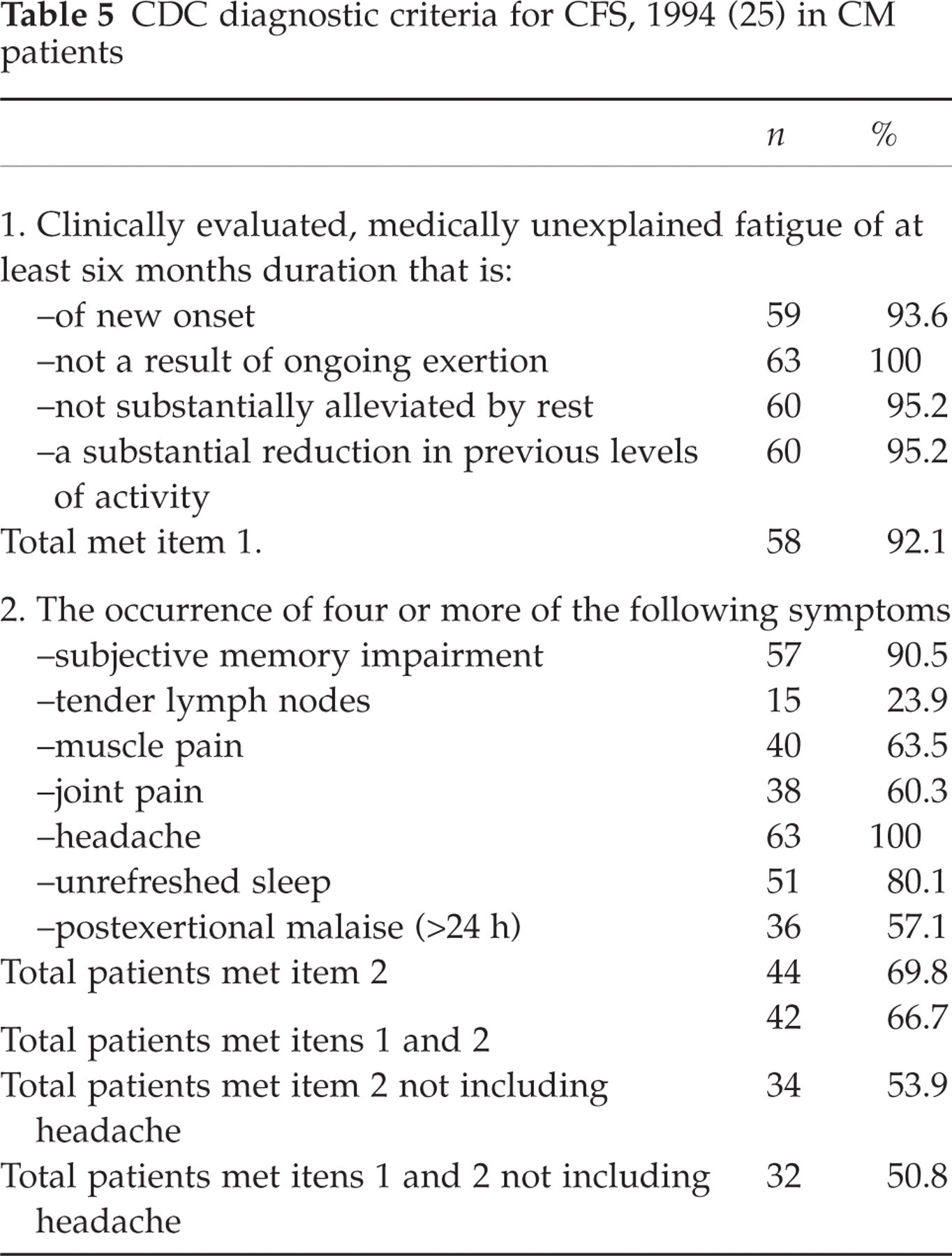
Fifty-three of the 63 (84.1%) patients had FSS scores greater than 27. Forty-two (66.7%) patients met the CDC criteria for chronic fatigue syndrome, but only 32 (50.8%) met the modified CDC criteria when headaches were not considered. Table 3 shows the correlations between the fatigue scales and the scores for depression and anxiety. Table 4 shows the relationship between insomnia, fibromyalgia, disability and gender with fatigue. Age, pain intensity and acute medication overuse did not correlate with any of the fatigue scales. Table 5 represents the CDC diagnostic criteria for CFS applied to TM patients.
Correlations between scores for depression, and for anxiety, FSS, mental fatigue and physical fatigue scores (Pearson's correlation test)

∗ P < 0.05,
∗∗ P < 0.01.
Association between Insomnia, fibromyalgia, disability, gender and FSS, mental fatigue and physical fatigue scores (One way

∗ P < 0.05.
CDC diagnostic criteria for CFS, 1994 (25) in CM patients
Discussion
Fatigue is a symptom of many disorders and is a disorder unto itself (CFS). Its subjective nature makes it difficult to study. We used a general fatigue scale (FSS), and a scale which separates mental and physical fatigue symptoms (Chalder), and the CDC criteria for CFS in order to quatify it. We also applied a modified CDC criteria eliminating headaches as one of the criteria. Fatigue as a symptom and CFS as a disorder are common in CM patients; 84.1% of patients had fatigue (defined by a FSS scale score higher than 27), and 66.7% met the CDC criteria for CFS. Fatigue has been reported in 52%−70% (17, 18) of CDH patients. It is uncertain if fatigue is just an associated symptom of CM, or CFS is a disorder comorbid with CM.
The diagnosis of CFS in patients with other psychiatric or medical disorders is controversial (9). Headache is one of the symptoms in the CDC diagnostic criteria for CFS, and is present in 59% of patients with CFS (26). Despite its high prevalence, the headache type in CFS has never been diagnosed according to the International Headache Society classification. Some of the patients with CFS diagnosis might have episodic or chronic migraine. The CDC diagnostic criteria for CFS are less specific in a headache population since, by definition, all patients have headache. When we applied a modified CDC criteria without considering headaches as part of the symptoms the percentage of patients who met the criteria drop from 66.7 to 50.8%. A reappraisal on the CFS case definition in the light of the headache diagnosis may change our understanding of fatigue and CFS.
Peripheral and central mechanisms have been implicated in the pathopysiology of fatigue. Hypothalamic involvement is suggested by an impairment of central CRH synthesis and release (27); altered serotoninergic (28) and noradrenaline function have also been implicated. Cytokines may be involved; elevated levels of interleukin-1beta (IL-1Beta) and IL-6 (29) have been reported.
Depression and fatigue are intimately related. In cancer patients, fatigue was related to depression and anxiety (2). In multiple sclerosis, fatigue correlated to depression (7). In our CM patients, fatigue correlated to depression. Fatigue is one of the symptoms of depression, and CFS is comorbid with depression. However, guilt, lack of self-esteem, and self-blame, which are core features of major depression, are less common in CFS patients (30). Fatigue in a CM patient should lead to a suspicion of depression. It is unknown whether fatigue improves with relief of depression and headache in CM patients.
Although Spierings & van Hoof (18) found headache patients slept significantly shorter than controls, insomnia was not associated with FSS, mental or physical fatigue scores in our study. This suggests that sleepiness, resulting from sleep deprivation might be a different condition in CM patients. Other sleep disorders, also associated with daytime sleepiness, still need to be considered in the evaluation of a headache patient with fatigue.
Fibromyalgia was related to the physical fatigue scale but not the mental and FSS scales. This suggest that recognizing the subtypes of fatigue may help understanding their underlying cause. Women had higher FSS scores than men in our patients. However, mental and physical fatigue scales were not associated with gender.
Prior to treatment of the CM patient with fatigue one must exclude hypothyroidism, electrolyte imbalance, infections, anaemia, renal failure, and diabetes (10). Therapeutic interventions include a graded aerobic exercise program, cognitive behavioural therapy, and antidepressants.
Future research is needed to better understand the role of fatigue in headache patients. Fatigue in other headache types might be studied, as the relationship of fatigue, excessive daytime sleepiness, and other sleep disorders in headache patients.
Identification of fatigue and its subtypes in headache disorders and recognition of headache in CFS patients has implications for the pathophysiology, diagnosis and treatment of these disorders.