
Abstract
In recent decades whiplash injuries, being a major reason for compensation claims, have become increasingly important in forensic medicine. In view of this, a reliable diagnostic method of assessing cervical range of motion (ROM) is needed. The aim of the present study was to evaluate neck function with a 3D kinematic method compared with clinical evaluation in whiplash injury. Seventy consecutive patients (M/F = 18/52) with a history of whiplash injury (WH) and 46 healthy volunteers (M/F = 24/22), mean age, respectively 33 ± 9 and 28 ± 6 years (mean ± SD) entered the study. Patients suffered from neck pain and/or unilateral headache. A computerized kinematic analysis of the ROM (Elite system) using passive markers and two infrared TV cameras was used. Clinical evaluation of active ROM was also performed both in patients and in 61 controls (M/F = 23/38; mean age 47 ± 18 years). Thirty out of 70 patients were tested at the time of their first consultation (T0) and 6 months later (T6), and 12 were also followed up after a year (T12). All neck movements, except extension, were significantly reduced in WH subjects compared with controls, in particular lateral bending. Comparing ROM at T0, T6 and T12, no significant differences were found. A global index of motion (GIM), obtained by calculating the sum of ROM in absolute value for all the movements acquired, was significantly reduced in WH compared with control subjects. The interobserver reliability of the clinical evaluation was globally acceptable. On the basis of the clinical evaluation, a significantly reduced ROM was found in all movements in WH subjects compared with an age-matched population. Computing the number of impaired cervical movements (ICMs), a significantly higher number was observed in WH patients than in controls, showing a decreasing trend at T6 and T12, with a significant improvement at T6 vs. T0. The computerized study of neck ROM may constitute a useful tool in the evaluation of WH at baseline and follow-up.
Introduction
In recent decades, many attempts have been made to obtain an objective method of assessing cervical spine mobility (1–9). Indeed, because of the complexity of the cervical joint apparatus, clinical evaluation alone may not be adequate in all situations. Furthermore, cervical spine mobility is thought to be influenced by ageing, biomechanical factors and degenerative processes. Thus, neck movement analysis is of clear clinical importance and requires a technique that is neither invasive nor complex to perform, and that provides reliable parameters. While for routine evaluation a rough clinical assessment based upon pure subjective evaluation may be sufficient, in case of cervical anaesthetics procedure or evaluation of certain treatment, a much higher degree of resolution should be used.
The function of the cervical spine has been kinematically examined in the past, using sequences of lateral X-rays, usually of the flexion-extension range of motion (ROM) (2–4, 8), and cineradiography (5). However, given the considerable difficulty involved in obtaining diagnostically and clinically useful information from the vast amount of data produced by the computerized reconstruction and elaboration of neck movements (2–4, 8), these techniques were progressively discarded.
Thus, several instruments such as goniometers (1, 7, 9–13) and inclinometers/cybex (14–16) have been developed for the non-invasive evaluation of cervical spine movement. Although these devices are easy to use, not expensive and some of them have also shown reliability (9–13), they have proven to be cumbersome for patients (11), and to require the intervention of skilled examiners. Inclinometers, in particular, although easy to use, quick and inexpensive, have shown a relatively low level of intraobserver reliability (1, 15).
Recently, different studies (17–20) have been conducted to obtain a 3D kinematic analysis model of the anatomical head–neck structure by means of opto-electronic scanners. Such instruments were developed to quantify ROM and analyse qualitatively other parameters like the pattern of curvature, centre of rotation, etc. Furthermore, 3D kinematic evaluation of cervical ROM has been shown to be useful in assessing the coupled joint motion (17) that occurs at different levels in the cervical spine, in order to identify ‘abnormal’ mobility and thereby to improve the accuracy of motion analysis.
The method used in the present study allows the measurement of the active ROM during the execution of head flexion-extension, lateral bending and axial rotation movements by means of an ad hoc 3D anatomical model (21).
Since the pathogenic substrate of neck sprain is still far from being known, it is a demanding task to unravel putative and subtle abnormalities using more sophisticated 3D studies.
The aim of the present work was to evaluate the usefulness of a 3D kinematic method, compared with the clinical evaluation, in the study of neck function in whiplash injury, in order to quantify any impairment of cervical spine mobility (21) and the outcome of the disease.
Patients and methods
Patients
Seventy consecutive patients (M/F=18/52), referred to the ‘C. Mondino Foundation’, with a history of whiplash injury and 46 healthy volunteers (M/F=24/22), mean age, respectively 33±9 and 28±6 years, entered the study. Patients included were required to have sustained a whiplash injury more than 1 month earlier. The illness duration was ≤1 year in 42 patients (5±3 months; ≤6 months in 26 of these) and >1 year in 28 (49±30 months). In accordance with the Quebec Task Force (QTF) Classification of Whiplash Associated Disorders (WADs) (1995) (22), 56 patients were diagnosed as grade 2 and 14 as grade 3. All of them suffered from neck pain and/or unilateral headache (if bilateral, the pain was predominant on the same side).
Thirty-eight subjects had been involved in a rear-end collision and 6 in a frontal collision; in 14 patients neck sprain resulted from a lateral impact, while in 12 a mixed mechanism was described.
All patients were tested with the Elite at the time of their first consultation (T0). Thirty of them were re-examined 6 months later (T6) and 12 of these 30 patients were also followed-up at 12 months (T12).
A pure clinical evaluation of active ROM was also performed both in the 70 whiplash injury (WH) patients (M/F=18/52) and in 61 historical controls (M/F=23/38; mean age 47±17.9 years). An age-matched group of 45 subjects (M/F=9/36; mean age 37.5±11.6 years), selected from the historical control group, was compared with the WH patients. The series of controls denied any head/neck trauma and/or any history of headache (migraine, episodic tension-type headache (TTH) >1 day/month) or neck pain.
Methods
Patients were evaluated using a structured interview and screened by means of a questionnaire applying the diagnostic criteria for cervicogenic headache (CEH) (23, 24), migraine without aura (M) (IHS) and headache associated with neck disorders (HN) (IHS Classification Committee, 1988) (25). On the basis of IHS diagnostic criteria, after a 3-month well-documented retrospective history recording, patients with TTH were excluded. At the time of the first consultation the litigation was still open while at 6-months follow-up any claims were resolved.
Neck movement assessment
In order to assess cervical spine movements, computerized kinematic analysis (Elite system) was performed by means of passive markers and two infrared TV cameras working at a sampling rate of 50 Hz. The Elite system (B|T|S, Milan, Italy), a TV image processing system, supplies the 3D co-ordinates of all visible markers, evaluating cervical spine ROM with respect to the trunk (degrees) (Fig. 1). The kinematic model developed required the reconstruction of six anatomical points, three of them describing the head and the other three describing the trunk. The selected points are shown in Fig. 1. The reliability of this system has been demonstrated in a previous study (21).

(a) Basic marker set-up on head and trunk while the subject is still. The markers are as follows: (LH) left and (RH) right sides of the head (located 4 cm either side of head vertex); EOP, external occipital protuberance; C7, seventh cervical vertebra; (LS) left and (RS) right shoulders on the acromion protuberance. (b) Technical markers (T1–T3) and anatomical markers (A1…A6) during the anatomical calibration procedure.
The subject was comfortably seated and looking straight ahead before performing each recording session, with shoulders and thorax kept in a fixed position to guarantee the selective measurement of the cervical spine movement.
To avoid disturbances on acquired data because of hair movement, the subjects were wearing special elastic cotton caps fixing and hiding their hair.
The subjects were asked to perform, in sequence, the following active movements: head flexion-extension, lateral bending and axial rotation. Each movement was repeated five times with no pauses in between. The sequences had to be performed at natural cadence, aiming to obtain the maximum ROM. The mean of three movements (excluding the highest and lowest ones) was taken as the real ROM value. Further details on the apparatus and the mathematical reconstruction of marker co-ordinates have been provided by Bulgheroni et al. (21). Zero degree was taken as the neutral position and the ROM was calculated as an absolute value (21).
In the present study, we also calculated a global index of motion (GIM), as the sum (in degrees) of the ROM in absolute value for all the movements acquired. Moreover, the percent variation, compared with baseline (T0), of each movement at T6 and T12, respectively, was also calculated.
Two experienced examiners performed clinical evaluation, assessing right and left flexion, right and left extension-rotation, right and left flexion-rotation, right and left lateral flexion, right and left rotation. ROM was clinically assessed as follows: 0=100% dysfunction, 1=75% dysfunction, 2=50% dysfunction, 3=25% dysfunction, 4=no dysfunction, where dysfunction stays for reduced functionality of neck movement. Furthermore, the number of impaired cervical movements (ICMs) was also computed as the sum of movements with a score ranging from 0 to 3, i.e. with a decreased ROM.
Statistical analysis
The data were analysed using the statistical program SPSS for Windows (version 6.3).
One-way
The intraclass correlation coefficient (ICC) was, as described by Fleiss (26), calculated for each movement assessed by clinical evaluation. The ICC is the fraction of variance calculated by the variation between subjects. Thus, if the variance between tests (or examiners) is small compared with the variance between subjects, then the ICC is close to 1. According to Fleiss (26), ICC values >0.75 generally mean ‘excellent’. Paired Student's t-test was applied to assess whether the mean differences between examiners were significantly different from zero. A two-sided P-value of 0.05 was regarded as significant.
The non-parametric Mann–Whitney u-test was performed to assess possible differences in the clinical evaluation of cervical ROM between WH patients and healthy subjects (n=46), while the non-parametric Kruskal–Wallis test was applied between groups of patients with different illness durations.
Results
On the basis of the relevant criteria, the following diagnoses were obtained: CEH (Sjaastad et al. 1990) (n=24) 34.3%; M (IHS) (n=8) 11.4%; HN (IHS) (n=10) 14.3%; CEH + M (n=8) 11.4%; CEH + HN (n=6) 8.6%; non-classifiable (n=14) 20%. The relation between headache and whiplash has not been the object of the present study.
Kinematic analysis
All neck movements, with the exception of extension, were significantly reduced in WH patients with whiplash injury compared with controls (n=46) (P<0.05), in particular right and left bending (P<0.005) and left rotation (P<0.005) (Fig. 2). Grouping patients according to the QTF scoring system, no significant differences in ROM were found when CEH patients were compared with those with no CEH.

Cervical range of motion (ROM) assessed by 3D kinematic analysis in whiplash patients (WH) and in controls (Co). E, Extension; F, flexion; LR, left rotation; RR, right rotation; LB, left bending; RB, right bending. One-way
WH patients with a recent whiplash (≤1 year) showed a somewhat reduced ROM (in particular left rotation) when compared with those with an illness duration >1 year. Furthermore, subjects with a neck sprain within the previous 6 months showed significantly reduced neck extension in comparison with patients with a longer illness duration (>6 months) (P<0.05) (Fig. 3).

Cervical range of motion (ROM) assessed by 3D kinematic analysis in patients with a recent whiplash (WH≤6 months) and in those with a longer illness duration (WH>6 months). E, Extension; F, flexion; LR, left rotation; RR, right rotation; LB, left bending; RB, right bending. ▪, WH≤6 months (n=26); □, WH>6 months (n=44). ∗P<0.05, Kruskal–Wallis.
The GIM, calculated as the sum of the ROM of all the movements acquired, was significantly reduced (P<0.005,
Global index of motion (GIM) in whiplash patients at T0, grouped as whiplash (WH) ≤6 months and >6 months, at T6, at T12 and controls (Co)

∗
P<0.005;
No significant correlation was found between ROM and WAD score (QTF Classification) (22), and, respectively, headache diagnosis, type of collision and pain side.
Comparing ROM at 12-month follow-up with T0 and T6, no significant differences emerged, even though for some variable cervical spine mobility showed a trend towards improvement. When comparing T6 vs T0 only left rotation was significantly improved (Table 2).
Cervical range of motion (ROM) assessed by 3D kinematic analysis at the first consultation (T0) and at the 6-month follow-up (T6) in whiplash patients (n=30)

Values are expressed in degrees.
∗ P<0.05; Student's paired t-test.
The mean percent variation of cervical ROM for each movement was also calculated (Table 3); at T6 a relatively small increase (<30%) was noticed but, due to the large standard deviation, no relevance was attached to the finding.
Percent variation of range of motion (ROM) evaluated with 3D kinematic analysis in whiplash patients

When T12 was compared with T0 a large percent increase (>50%) was recorded in right and left lateral bending, with a significant improvement emerging in right lateral bending when comparing T0 with T6 and with T12 data (P<0.05,
No significant difference in GIM emerged when data from the time of the first consultation were compared with those at the T6 and at the T12 follow-up.
Clinical evaluation
The interobserver reliability of the clinical evaluation, computed according to Fleiss (26), was good for all movements (0.68–0.86) with the exception of left lateral flexion (ICC=0.47) (Table 4).
Intraclass correlation coefficient (ICC) values for cervical movements assessed by clinical examination to compare mean differences between the two examiners

At clinical evaluation, WH patients showed a decreased ROM compared with age-matched controls, as shown in Table 5. Up to 80% of healthy subjects showed no dysfunction (score 4) in any cervical movement, the only exception being lateral flexion (impaired in 47% of controls). On the other hand, 63–91% of WH patients showed a dysfunction ranging from 100% to 25% (score=0–3), lateral flexion being the movement most frequently reduced (Table 5).
Clinical evaluation in whiplash patients (n=70) and in an aged matched population (n=30)

For statistical significance see text.
When WH patients were compared with an age-matched population (Table 5), a significantly reduced ROM was found in all movements (P<0.05 in right flexion-rotation and right rotation, P<0.005 in extension-rotation, flexion, left flexion-rotation, left lateral flexion and left rotation; Mann–Whitney u-test), in particular in right lateral flexion (P<0.001). The significance of ROM impairment increased when matching WH patients vs. controls both with a decreased ROM (score 0–3) (Table 5).
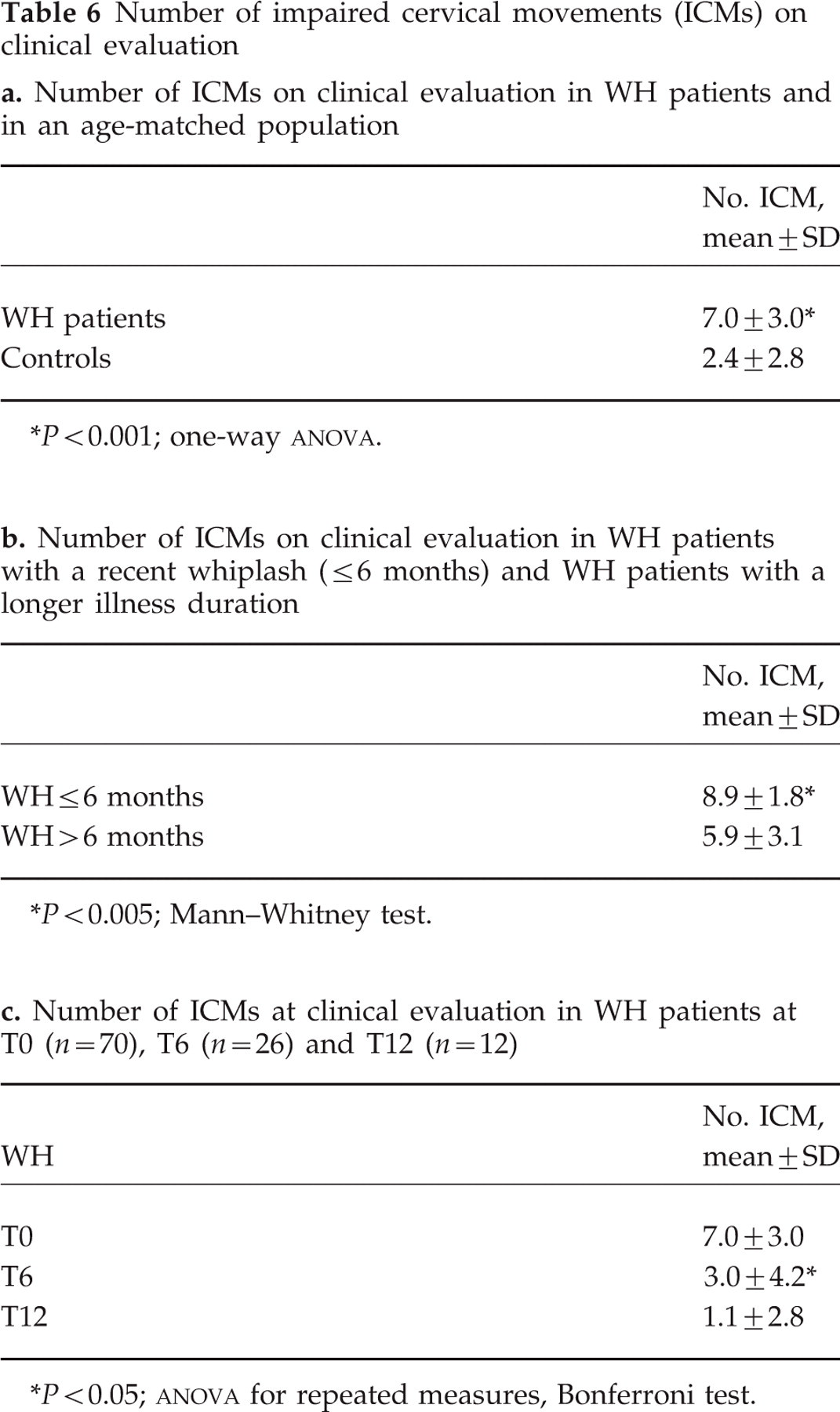
Computing the number of ICMs, a significantly higher number was found in WH patients than in controls (P<0.001) (Table 6a). Since 74% of WH patients showed more than five reduced movements, and in 87% of controls four or less movements were reduced, we took impairment of more than five cervical movements as a reliable ‘cut-off’ point to distinguish reduced ROM (>5) from normal ROM (≤5) (Fig. 4). Moreover, the number of ICMs was significantly higher in WH patients with a recent whiplash injury (≤6 months) than in those with a longer illness duration (Table 6b), and when comparing T0 vs. T6 and vs. T12 (Fig. 5), a significant reduction in ICMs was found at T6 vs. T0 (P<0.05,
Number of impaired cervical movements (ICMs) on clinical evaluation
∗
P<0.001; one-way
∗ P<0.005; Mann–Whitney test.
∗
P<0.05;
Clinical evaluation in patients with a recent whiplash (≤6 months) (n=26) and in those with a longer illness duration (>6 months) (n=44)


Number of impaired cervical movements (ICMs) in whiplash patients (WH) and in controls (Co). □, Co (n=30); hatched, WH (n=70).

Number of impaired cervical movements in whiplash patients (WH) at time of first consultation, at 6-month (T6) and 12-month (T12) follow-up. ○, WH T0; □, WH T6; ▵, WH T12.
A higher percentage of recent whiplash injury subjects (77–100%) than patients with longer disease duration (50–86%) showed a reduced ROM, the most frequently reduced movements being extension-rotation, left flexion-rotation and lateral flexion (Table 7). Lateral flexion was also the most frequently reduced movement in WH sufferers with a longer disease duration. No significant differences were found at clinical evaluation of neck movement when comparing patients at T0, T6 and T12.
Patients with a whiplash occurring between 6 months and 1 year and those who had sustained a whiplash injury within the previous 6 months showed a significant clinical impairment of flexion-rotation and extension-rotation movements (respectively: P<0.05 and P<0.001, Kruskal–Wallis test) when compared with subjects with a longer disease duration.
No significant differences emerged among WH patients when comparing clinical evaluation at T0 with T6 and T12 (Friedman's test), although a trend towards improvement was seen.
Discussion
Many different opto-electronic devices have been conceived to obtain non-invasive, three-dimensional dynamic measurements of neck mobility (17–20).
3D kinematic analysis allows cervical spine function to be investigated, detecting ROM impairment not only due to organic lesions, as in the case of simple X-rays, but also due to neck dysfunction.
Dynamic radiographs, in fact, although useful for examining kinematic function of the cervical spine, necessitate a considerably high and lengthy exposure to radiation, which increases as (in order to obtain a more detailed examination) the number of X-rays is increased.
Despite its sophisticated software, the Elite system is reliable and relatively easy to use (17). Based on a simplified kinematic model of the anatomical head–neck structure, it evaluates the head and trunk as two rigid bodies able to move freely in space, without the need to restrict the subject's movement. The direct acquisition of markers positioned over selected points and/or of the so-called ‘technical markers’ (see Methods) eliminates the errors associated with marker positioning and detection that occur during X-ray elaboration, in particular when two radiographic projections are superimposed, and homologous landmarks have to be detected in both of them (2). However, even in the case of 3D kinematic analysis, specific staff training is necessary and the equipment used is expensive. While it is true, however, that goniometers and inclinometers (5, 7, 9–13) are inexpensive, quick, easy to use, and can show an acceptable, and in some cases even good, level of reproducibility, the intervention of an experienced examiner is nevertheless needed to increase the accuracy of the measurement. Inclinometers, in particular, have been shown to have rather poor resolution (15°), and not to be good tools for follow-up evaluation over a long period of time (15).
The first device conceived by Roozmon et al. (19, 20), the Cervicoscope (a variation of the Spinescope, albeit improved by the addition of a display to describe coupled joint motion) (20), requires sophisticated software engineering techniques to present the required information to clinicians efficiently and accurately. In fact, while the Elite system evaluates the position of the anatomical segments by measuring the angle between the head and the laboratory co-ordinate system, the Cervicoscope software is based on the movement of vectors calculated from the 3D spatial co-ordinates of the infrared emitting diodes (IREDs) placed on the head, neck, and shoulders. This procedure is based on the development of three algorithms to deduce the relative direction angles between vectors normal to the different groups of IREDs and with respect to the absolute reference frame. Therefore, the method used in the present study extrapolates biomechanical parameters of real clinical relevance.
Moreover, the Elite kinematic model, based on the reconstruction of six anatomical points, is, unlike the one based on 3D facial morphometry applied by Ferrario et al. (17), able to supply a complete description of head/neck mobility. This latter method, in fact, using the same digital image analyser, assessed alterations in the pattern of movement, calculating instantaneous centre of rotation and radius curvature only for flexion-extension movement, without considering lateral bending and rotation.
In contrast, the 3D anatomical model used in the present study made it possible to compute (in degrees of motion) the active cervical ROM for each movement evaluated, without any mechanical constraint, and, calculating velocity and acceleration of all visible markers, to obtain a more in-depth investigation.
A more complex 3D kinematic analysis method was used by Osterbauer et al. (18) in a relatively recent study, in which instantaneous helical axis (IHA) and a total biomechanical score were computed to characterize qualitatively movements of the head relative to the trunk. This method, based on a complex mathematical reconstruction of neck movements, describes alterations in the estimation of IHA during flexion-extension and oblique tracking tasks.
In our setting, all neck movements, with the exception of extension, were significantly reduced in whiplash patients. Osterbauer et al. (18), too, found a significant impairment of neck mobility in patients with whiplash injury. In order to find a biomechanical parameter that describes the total motion of the cervical spine, a GIM was calculated. This appeared to be useful as a first approach to neck impairment, as whiplash patients, compared with controls, showed a significantly reduced GIM, even though we were unable to detect any significant differences between patients grouped according to the WAD classification, between different types of headache or between patients at T6 and T12
Dvorak et al. (4) found hypermobility in the upper segments in patients with cervical trauma. As often occurs in whiplash injury, a muscular restraint can result in a decrease in the muscular force needed to limit motion at upper and middle cervical spine level where, because of the less stable gliding motion of the cervical spine at these levels, considerable muscular force is required. In the present study, in contrast, whiplash patients showed normal ROM as regards extension, while all the other movements were reduced as in hypomobility of the lower cervical spine, probably due to soft tissue damage and/or muscle restraint. Extension proved to be significantly impaired in patients with a recent whiplash injury (≤6 months), improving in a shorter time than other neck movements.
Although clinical evaluation showed a globally acceptable level of interobserver reliability, only flexion-rotation and rotation movements gave good ICC values, while left lateral flexion was shown to be unreliable, probably due to an extreme intra- and interindividual variability in its amplitude or, possibly, to weakness towards the end of the examination, when lateral flexion was usually evaluated. Moreover, it has to be said that the amplitude of lateral flexion varies greatly from subject to subject and, without producing great discomfort, is reduced by age and by degenerative pathologies, such as arthrosis. Similarly, in a previous study by Fjellner et al. (27), six of the eight cervical movements clinically investigated by two experienced physiotherapists, in particular rotation, showed an acceptable level of reliability.
The 3D kinematic analysis, in contrast, showed a good–excellent reproducibility for all movements (21) and proved to be an objective method that is more reliable and sensitive than clinical examination. Nevertheless, clinical evaluation proved to be useful, as a basal screening, in distinguishing whiplash patients from asymptomatic controls.
Computing the number of ICMs, in order to select a ‘clinical’ biomechanical parameter that describes the total amount of neck motion, we noticed that 74% of patients showed impairment of more than five movements; whereas four or fewer movements were found to be reduced in 87% of controls. Thus, we took impairment of more than five cervical movements as a ‘cut-off’ point to distinguish neck dysfunction (with a reduced ROM) from normal cervical spine mobility. This ‘cut-off’ point, and the ICMs themselves, were shown to constitute a good and useful ‘marker’ of neck impairment, as revealed by the significant differences both between WH patients and controls and between patients with a recent whiplash injury and those with a longer respite since the whiplash. Furthermore, the ICMs, showing a trend towards decrease (i.e. towards improved ROM), also proved to be quite useful not only in the diagnosis, but also in the follow-up of cervical spine dysfunctions (in particular whiplash injury). In our setting extension-rotation, left flexion-rotation and lateral flexion were the movements most frequently impaired in patients with a recent whiplash injury (and lateral flexion the most frequently reduced also in those with a longer disease duration). Moreover, flexion-rotation and extension-rotation were significantly reduced in patients with a recent whiplash injury (≤1 year and ≤6 months), these two movements apparently being the most reliable and useful ‘clinical markers’, at ‘first screening’, for the diagnosis and follow-up of neck dysfunction. It should also be noted that lateral movements, such as flexion-rotation and rotation, showed good reproducibility (ICC values).
The results of clinical evaluation seem to show a marked agreement with those of 3D kinematic analysis, and clinical evaluation seems to be reliable as a first examination tool, identifying cases of neck dysfunction that have a high probability of being confirmed by an objective evaluation such as the 3D kinematic analysis. These results partially agree with those obtained in the study by Fjellner et al. (27), indicating a difference in reliability between symptomatic and asymptomatic subjects (greater in the former).
Moreover, as regards percent variation, whiplash patients showed a tendency towards an improvement in cervical ROM impairment over time. Thus, 3D kinematic analysis proved to be a useful tool for follow-up evaluations in neck disorders. The large SD recorded in flexion-extension movements when comparing T6 and T12 with T0 data are due to some patients showing, at T0, a strongly reduced ROM, which is increased two to three-fold at T6 and/or T12 follow-up. The relative high drop-out rate in our patient series may be due to the fact that cases with a clinical improvement and solved compensation claim may be less prone to undergo a new assessment of neck function. Further follow-up studies may reveal a higher sensitivity by analysing 3D methods with passive and active clinical evaluation.
In conclusion, the method for the 3D kinematic analysis of cervical movements used in this study proved to be reliable, easily applicable in difficult clinical cases and, most of all, useful in whiplash injury diagnosis and follow-up evaluation. Clinical evaluation, on the other hand, was shown to be useful as a ‘first screening’ tool correlating with data obtained using the 3D kinematic analysis method. However, the Elite system remains a ‘sophisticated’ method of spine movement evaluation, and due to its cost is not designed for routine use but mainly for difficult clinical cases in forensic medicine and for research purpose.
Footnotes
Acknowledgements
This study was supported by a grant from the Ministry of Public Health no. 57.2/RF93.28. The authors are indebted to Professor Ottar Sjaastad for fruitful criticism. Appreciation is expressed to Miss Paola Castellotti for laboratory assistance.