
Abstract
In order to quantify the physical impairments associated with different types of headache, 77 subjects belonging to four different groups (postmotor vehicle accident cervicogenic headache subjects, cervicogenic headache subjects nontraumatic, migraine patients and control subjects) were evaluated using the following variables: posture, cervical range of motion, strength of the neck flexors and extensors, endurance of the short neck flexors, manual segmental mobility, proprioception of the neck, and pain (McGill Pain Questionnaire and the skin roll test). The results of this study showed that postmotor vehicle accident cervicogenic patients have significantly limited active cervical range of motion (in flexion/extension and rotations), present decreased strength and endurance of neck flexors and decreased strength of the extensor muscles. Our results suggest that there are enough differences between the postmotor vehicle accident and nontraumatic cervicogenic headache subjects to warrant caution when analysing the data of these two subgroups together, as several studies have done in the past. The onset of headache is therefore an important variable that should be controlled for when attempting to characterize the physical impairments associated with cervicogenic headache.
Introduction
Headache arising from the cervical spine has been named differently by several authors: cervicogenic headache (1), headache of cervical origin (2), cervical headache (3). However, even if there are some controversies on the criteria used to diagnose it (4), the concept of headache arising from the cervical spine seems to have gained acceptance. Despite recent efforts to characterize cervicogenic headache, the clinical diagnosis is still difficult to make because of the overlap of symptoms among different types of headache. Therefore, relying only on the symptoms described by patients may not be a reliable way to accurately diagnose the problem. Few objective tests exist, except for diagnostic blocks that can be helpful for this purpose. Even diagnostic blocks are not practical for clinical use because they are invasive; they require special facilities and have to be done when the patient is in pain (1). The assessment of the presence of physical impairments in the neck has been proposed as an alternative in order to help in the diagnosis of cervicogenic headache (5). The treatment of the musculoskeletal impairments associated with cervicogenic headache has been proposed as an essential part of its overall management (5, 6). As examples of physical impairments associated with cervicogenic headache, Watson and Trott (7) found that cervical headache sufferers disclosed a significantly different head posture, and a reduction in the endurance and the strength of the short neck flexors when compared to nonheadache sufferers. Jull et al. (3) also found a significant decrease of the short neck flexors endurance in comparison with a control group. Alteration of cervical range of motion was also shown to be a distinctive feature in cervicogenic headache patients. Zwart (8) found significantly limited active motion of flexion/extension and rotation for a cervicogenic headache group compared to a migraine, a tension type headache and a control group.
Using manual examination, mobility findings in the craniovertebral spine area have also been shown by Watson and Trott (7) to be different in cervical headache and control subjects. These authors found approximately twice as much positive joint findings in cervical headache sufferers as compared to those without headaches. Proprioception of the neck has recently been the subject of several publications, especially in the case of chronic neck pain (9) and postmotor vehicle accident (MVA) patients (10, 11). Significant proprioception deficits have been found in those two populations. To our knowledge, proprioception of the neck has never been evaluated in cervicogenic headache patients.
The assessment of pain upon palpation has also been investigated in order to differentiate between different types of headache. Bovim (12) found that pressure pain threshold measurements were statistically different in cervicogenic headache compared to migraine, tension type headaches and control groups. The asymmetry in the pressure pain threshold between sides was also a feature present only in cervicogenic headache subjects. Bansevicius and Pareja (13) have used the ‘skin roll’ test (2) to evaluate the pain upon palpation in different types of headache. This test involves pinching an area of the skin and the subcutaneous tissues underneath between the thumb and the other fingers and rolling it in three areas (trapezius, mandibular, supraorbital). According to Bansevicius and Pareja (13), the trapezius area showed asymmetry between sides in terms of pain, as measured by a visual analogue scale (VAS) in the cervicogenic headache group only.
In a previous study by Philips and Jahnshahi (14), the McGill Pain Questionnaire (MPQ) showed a different pattern of pain between tension type headache patients and migraine patients. To our knowledge, this questionnaire has never been used on cervicogenic headache patients.
Cervicogenic headache can be the result of a traumatic event such as a whiplash injury during a motor vehicle accident (15). However, often no specific trauma is associated with the onset. Poor posture and degenerative joint disease are believed to be associated with an insidious onset (5). Studies on cervicogenic headache usually do not distinguish their subjects in terms of the type of onset. Clinically, however, the magnitude of the musculosketal abnormalities seem to be related to the type of onset. Therefore, it would be important to clarify the difference possibly existing between these two groups: traumatic onset (post-MVA) cervicogenic headache patients compared to cervicogenic headache patients with no associated trauma. Furthermore, it would be of interest, for the present literature to contrast these two groups of subjects with a migraine group in order to appreciate the magnitude of the differences between these clinical groups, relative to a control group.
Thus, the objectives of the present study were to (1): quantify different physical impairments in three types of headaches: post-MVA cervicogenic headaches, nontraumatic cervicogenic and in migraine compared to a control group, and (2) compare the impairments found in these three groups.
Subjects and methods
Subjects
A total of 60 patients with headache and 17 healthy controls were evaluated. Forty-four patients had a diagnosis of cervicogenic headache according to the main criteria of the International Headache Society (I.H.S) (16) and of Sjaastad (1). Those criteria were the presence of neck pain preceded or associated with the headache onset; headache precipitated or aggravated by sustained cervical postures, the presence of abnormal pain on neck palpation and restriction of the range of motion of the neck. Twenty patients had a traumatic onset following a car accident (all types of impact). The trauma was without concussion or amnesia. Twenty-four patients could not relate the onset of their headache to any traumatic event. Sixteen patients had a diagnosis of migraine in accordance to the I.H.S. criteria. All patients with headache were recruited from a headache clinic. Patients who agreed to participate were interviewed by a neurologist or a family physician with an expertise in headache to verify the inclusion and exclusion criteria. A second neurologist had to confirm the diagnosis for the patients to be included in the study. Subjects were excluded if they had any systemic or central nervous system diseases. Subjects in the migraine and control groups were also excluded if they had a history of neck pain that had interfered with their normal daily activities within the last five years.
Control subjects were recruited from the local community in order to age and sex-match the headache groups. All subjects signed an informed consent form. Ethical approval was obtained from the Medical Ethics Committee of the Montreal Rehabilitation Institute. Data on the subject's characteristics are presented in Table 1.
Group characteristics according to age, sex, and number of headaches per month in days reported (Mean±SD)
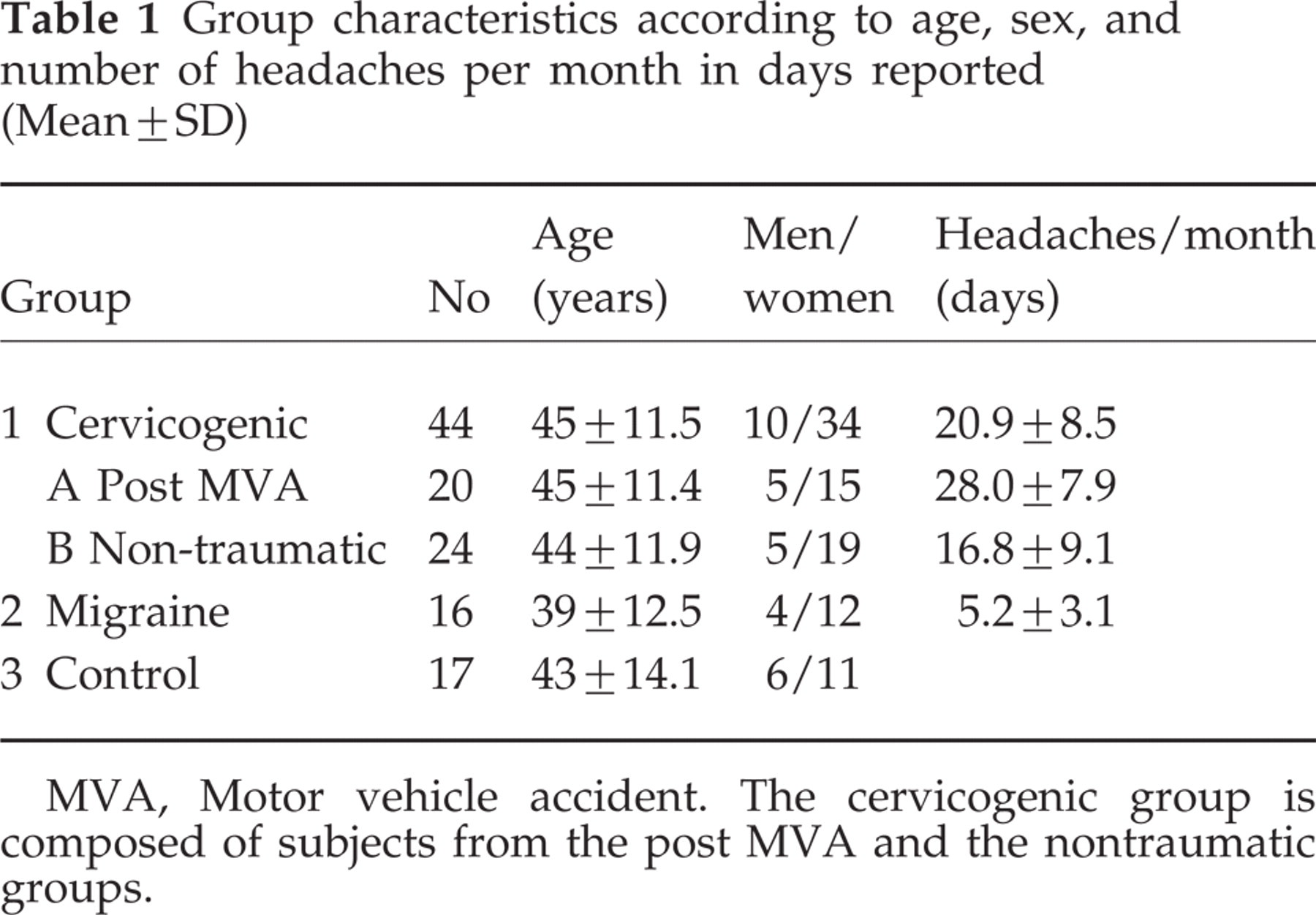
MVA, Motor vehicle accident. The cervicogenic group is composed of subjects from the post MVA and the nontraumatic groups.
All subjects in the headache groups presented symptoms for at least six months. The patients in the nontraumatic cervicogenic headache group had an average of 16.8 ± 13.1 years of symptoms, while the patients in the post-MVA group had their accident, on average, within 5.8 ± 5.2 years. Nine out of 11 subjects in the post-MVA group responded positively to a blockade (more than 50% decrease in their pain) of the greater occipital nerve, while 18 out of 23 subjects in the nontraumatic group presented the same response. The subjects were evaluated by one of the authors (JPD) who was not aware of the diagnosis of the majority (75%) of the subjects.
Evaluations were done in the following order: neck mobility, proprioception, posture, strength, manual segmental motion evaluation, short neck flexors endurance, skin roll test, and pain. All subjects were evaluated once and an evaluation session lasted for about an hour.
Neck mobility and proprioception
Neck active range of motion (AROM) was measured with the cervical range of motion (CROM) goniometer (Performance Attainment Associates, Roseville, Minnesota), a device that has been shown to be reliable (17, 18). Measurements were made with the subjects in the sitting position, with their feet resting flat on the floor, the thoracic spine being in contact with the chair's backrest and the lumbar spine positioned in neutral. Each movement of flexion, extension, lateral bending, and rotation was measured twice bilaterally. The sum of movements to both sides for the transverse and frontal plane and flexion combined with extension for the sagittal plane was averaged and used for statistical analysis as has been done previously (8).
Evaluation of the neck proprioception was done according to the protocol developed by Loudon et al. (10), where a CROM goniometer was used. With the CROM on the subject's head and their eyes closed, the head was positioned by the examiner at a 30° right rotation and then returned passively to 0°. The subject was then asked to reproduce this head position three times and each measurement was recorded. The procedure was repeated in five other test positions (left rotation 30°, right lateral bending 20°, left lateral bending 20°, right rotation 50°, left rotation 50°). The absolute difference between the recorded measures and the targeted angle was calculated and the mean of the three trials, for each angle, was retained for the statistical analysis.
Posture
The postural measure used was the craniovertebral angle (19), which is the angle formed by a horizontal line passing through the spinous process of C7 and a line passing through the tragus of the ear and also the spinous process of C7. A lateral photograph obtained with a digital camera (Kodak DC-120) was taken with the subjects in the sitting position. The photo was taken after the subjects performed large amplitude movements of flexion and extension and gradually decreased the amplitude of the movements until the subject's head rested in a comfortable position (20). Vertical lines from the background were visible on the photograph. The angle was measured in degrees using a photo edition software (CorelDRAW 8.0). This technique was compared to the manual protractor technique used by Watson and Trott (7) on a sample of 20 subjects and showed excellent concordance (Pearson's correlation coefficient of r=0.98).
Strength and endurance of the neck flexors and strength of the neck extensors
Clinical measurements of the cervical flexors and extensors strength were made with a MicroFet hand-held dynamometer (Hogan Health Industries) using a similar protocol to that used by Silvermann (21) who measured cervical flexor strength in chronic neck pain patients. Reliability of this technique has been shown to be good (21) (ICC > 0.74). For measurements of neck flexors strength, the subjects were positioned supine, the chin retracted. With the dynamometer placed on the centre of the forehead and the head being slightly off the bed, the subjects were asked to maximally push against the dynamometer while the examiner held the device still (isometric hold).
Cervical extensors strength was tested in a similar way with the subjects lying in the prone position and with the dynamometer placed in the back of the head. Contractions performed against the dynamometer held by the examiner lasted 3–5 s and were repeated twice with a 60-second rest period between trials. The mean of both repetitions was used for statistical analysis. The dynamometer was calibrated prior to data collection.
The protocol developed by Grimmer (22) was used to measure the endurance of the short neck flexors. Subjects were supine with no pillow. Their head was passively positioned 2 cm away from the plinth with their chin retracted. They were asked to hold their head still for as long as possible. The length of time until the chin began to thrust was measured using a stopwatch. This protocol has previously been shown (22) to present a high level of reliability (ICC > 0.92) when used with normal subjects.
Manual segmental motion
Six techniques of passive accessory intervertebral movement (PAIVM) and six techniques of passive physiological intervertebral movement testing (PPIVM) were used to evaluate segmental mobility of the cervical spine. These techniques are commonly used by physiotherapists and have been described elsewhere (23). A nominal 3-point scale (normal, slight hypomobility, severe hypomobility) was used to estimate the segmental mobility of the cervical spine. Each technique was performed once.
Skin roll test and pain
A ‘skin roll’ test (13) was performed in two areas (1), trapezius—halfway between C6 spinous process and the acromion and (2), mandibular, at the angle of the jaw. The procedure was performed once on each side of the body. Upon completion of each maneuver, the subjects were asked to mark the pain level provoked by the skin roll test on a 100-mm visual analogue scale (VAS). The asymmetry was calculated using the absolute difference between the scores obtained, respectively, on the right and left side.
Pain
At the end of the evaluation session, subjects were asked to complete a McGill Pain Questionnaire Short Form (MPQSF) (24). This test includes a Present Pain Intensity score (0–5) and a Pain Rating Index for the affective and sensory component of the pain. The individuals were asked, if they did not have a headache at the time of the evaluation, to try to remember the most common type of headache they usually have, while completing the questionnaire.
The data were analysed using SPSS 8.0 for Windows. One-way analysis of variance (
A Pearson correlation coefficient (r) was calculated to test the concordance between two clinical methods to measure the craniovertebral angle. A χ2 test for a contingency table was used to test if there was any difference in the distribution of the frequencies of the ratings (3-point nominal scale) among the four groups for the manual segmental mobility tests.
Results
Cervical range of motion and proprioception
Table 2 shows the results of the cervical AROM obtained in the different groups. The movement (total rotation) in the transverse plane (F = 18.1, P< 0.001), the movement (total flexion and extension) in the sagittal plane (F = 16.4, P< 0.001) and the movement (total lateral bending) performed in the frontal plane (F = 4.2, P< 0.001) differed significantly between the groups. Post-hoc Tukey tests indicated that the post MVA group present significantly different movements compared to all other groups. The only exception found was the movement performed in the frontal plane where the difference was significant only between the post-MVA and the migraine group (P = 0.006). The asymmetry of movement (difference between the right and left) was significantly higher in the post-MVA as compared to the control group for the rotation (P = 0.050) while no difference was found for lateral bending (P = 0.592).
Cervical range of motion (Mean±SD). Asymmetry refers to the difference of the scores obtained on each side
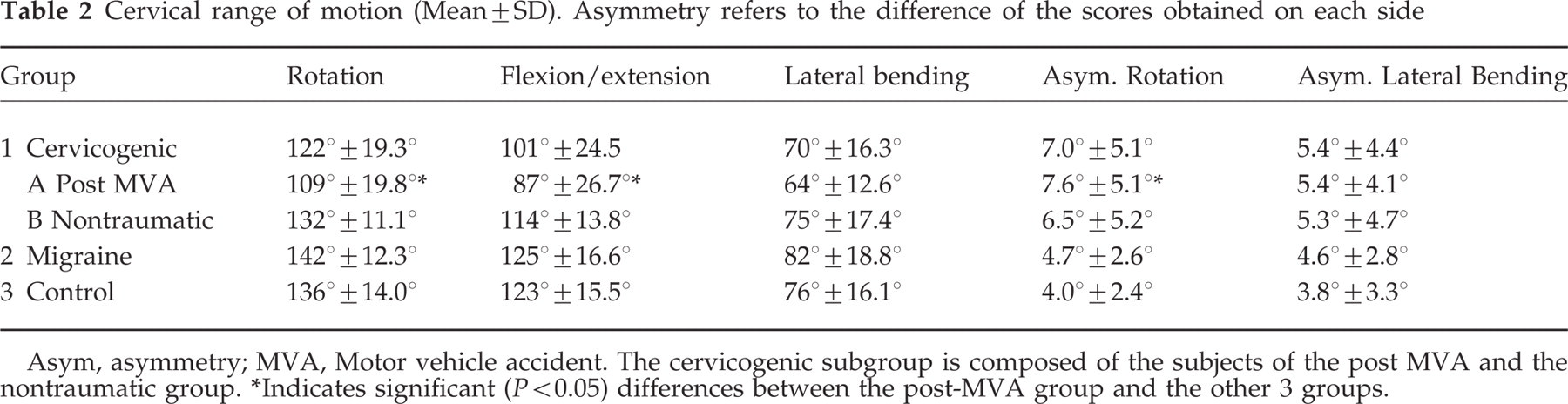
Asym, asymmetry; MVA, Motor vehicle accident. The cervicogenic subgroup is composed of the subjects of the post MVA and the nontraumatic group.
∗Indicates significant (P < 0.05) differences between the post-MVA group and the other 3 groups.
The results of the proprioception test are displayed in Table 3. No significant difference (F = 0.690; P=0.561) was found between the four groups.
Mean error (± SD) in repositioning of the head (proprioception) for head rotation, lateral bending on both right and left sides

Rot., rotation; Lat. B, lateral bending; R, right; L, left. The cervicogenic subgroup is composed of the subjects from the post MVA and the nontraumatic group.
Posture (craniovertebral angle), endurance of the neck flexors and strength of the neck flexors and extensors
The results are displayed in Table 4. For the neck flexors endurance, there was a significant difference (F = 3.9, P=0.007) found between the groups. A post-hoc Tukey test showed that the post-MVA group and the control group were significantly different (P = 0.007).
Craniovertebral angle, endurance and strength in Newton (N) of neck muscles (Mean±SD)

cv angle, craniovertebral angle; MVA, Motor vehicle accident; The cervicogenic subgroup is composed of the subjects of the post MVA and the nontraumatic group. Indicates significant (P < 0.02) differences with the control group.
A one-way
Manual segmental motion
Figures 1 and 2 illustrate the relative frequencies of the different ratings of manual segmental mobility using PAIVM and PPIVM tests. The results of the Chi-square tests (Table 5) indicated the presence of a significant difference (P < 0.05) in the distribution of the frequencies of the different ratings between the groups. This was so, for 5 out of 6 techniques for the PAIVM and for 2 out of 6 techniques for the PPVIM.
Results of χ2 tests performed on the data of each of the manual mobility techniques

Ext., Extension; Side Fl., Side Flexion; Unil., Unilateral; Ipsi., Ipsilateral; P/A, Postero-anterior pressure.

The relative frequencies of passive accessory intervertebral mobility (PAIVM) ratings in the different groups. ▪ Severe hypomobility; () Slight hypomobility; □ Normal. Post MVA, post motor vehicle accident.
The relative frequencies of the passive physiological intervertebral mobility (PPIVM) ratings in the different groups. ▪ Severe hypomobility; () Slight hypomobility; □ Normal. Post MVA, post motor vehicle accident.
Skin roll test and McGill Pain Questionnaire Short Form
The results of the Skin roll test showed that the post-MVA group reported higher tenderness on the VAS (on all areas tested) as compared to the control group (Table 6). One-way
Results (Mean±SD) of the visual analogue scale (VAS, 100 mm) completed following the skin roll tests. The asymmetry between right and left, that is the differences obtained on the VAS, is also reported

VAS, Visual Analogue Scale. The cervicogenic subgroup is composed of the subjects of the post MVA and the nontraumatic group.
∗Indicates significant (P < 0.01) differences with the control group.
The nontraumatic cervicogenic group scored higher on the VAS in the trapezius area as compared to the control group (P < 0.002). The asymmetry, however, was not significantly different between these 2 groups (P = 0.43).
One-way
Results of the short form McGill Pain Questionnaire obtained for the Pain Rating Indexes (PRI)

The cervicogenic group is composed of the subjects of the post MVA and the nontraumatic groups.
∗Indicates significant differences (P = 0.001) between the control group and the other 3 groups.
Comparison between the post-MVA group and the nontraumatic cervicogenic group
The results of the post-hoc Tukey analyses indicate that three variables were found to be significantly different between the post-MVA group and the nontraumatic cervicogenic group. These variables are the combined motion of flexion and extension (P < 0.001), rotations (P < 0.001), and asymmetry in the VAS of the trapezius muscles (P = 0.003). Other statistical analyses performed with the subjects of the two cervicogenic groups being pooled (post-MVA and nontraumatic) have been conducted using a one-way
A summary of the analyses done with the cervicogenic headache subgroups pooled together or taken separately are displayed in Table 8. Results indicate that most of the differences found in the pooled cervicogenic group compared to the control group can be attributed to the post-MVA traumatic group.
Comparison of the control group with the cervicogenic group (n = 44) as a whole or separately: post-MVA (n = 20) and nontraumatic (n = 24)

MVA, Motor vehicle accident; VAS, Visual Analogue Scale.
Discussion
Neck mobility and proprioception
The variable that seems to distinguish the post-MVA group the most from the others is the cervical AROM. This is especially so for the movement in the transverse plane (rotations) and in the sagittal plane (flexion/extension). The AROM in these planes is significantly different when compared to the other groups. However, the AROM in the nontraumatic group is not different from the migraine or the control groups. These results are similar to those of Zwart (8) for the cervicogenic group (onset not specified). The range of motion of the control and migraine groups are in agreement with the normative data published by Youdas et al. (25) using the CROM goniometer.
The asymmetry of movement is a clinical finding that is believed to be associated with spinal dysfunction, however, to our knowledge; no studies have specifically addressed this question. Our findings seem to provide preliminary support for these empirical observations, at least for the rotation. Moreover, the higher asymmetry found in rotation in both cervicogenic groups could have been higher if the passive range of motion had been used instead of the active range of motion as demonstrated by Wong and Nansel (26).
Contrary to previous reports (10, 11), our results did not show the presence of any significant difference in terms of cervical proprioception in the post-MVA group. Tested only on 2 groups of 11 subjects, the protocol developed by Loudon et al. (10) was probably not sensitive enough to highlight any potential group differences. Results might have been different if the Revel et al. (9) protocol had been used.
Posture
Contrary to what has been shown by Watson and Trott (7), the craniovertebral angle as a postural measure could not depict any differences between the groups. However, the values found in the migraine and control groups were similar to those found by Watson and Trott (7) in their asymptomatic sample. As previously discussed elsewhere (27), this finding might highlight the need to redefine more meaningful postural measures that would reflect more adequately the complexity of human posture.
Strength of the neck flexors and extensors and endurance of the short neck flexors
Strength of the neck flexors and endurance of the short neck flexors showed a similar tendency. Interestingly, the values obtained from the post-traumatic and the nontraumatic subjects are very similar for these two variables and both significantly different to those of the control group (Table 4).
Other studies (7, 28) using laboratory equipment, found a similar deficit of endurance and strength of the short neck flexors in headache of cervical origin. The strength of the cervical extensors, which has never been, to our knowledge, tested on cervicogenic headache patients, may also bring valuable clinical information. The deficit in extensors strength in cervicogenic cases is similar to what has been found by Jordan et al. (29) in a study on chronic neck pain patients.
Manual segmental motion
Manual segmental mobility is believed to play an important role in the clinical identification of cervicogenic headache (5). However, the interater reliability of manual segmental motion is usually considered poor (30, 31).
One of the reasons that has been identified, is the fact that raters develop idiosyncratic interpretation of their perception of motion, which makes it hard to compare their findings with others. However, it has been shown (7, 32) that the intrarater reliability of the manual segmental motion of the craniovertebral spine is good to excellent (0.67<Kappa<1.0). Visual analysis of the segmental motion results (Figs 1 and 2) suggests less segmental motion in the two cervicogenic groups (post MVA and nontraumatic cervicogenic) especially for the PAIVM techniques.
Skin roll test and pain
As previously shown by other authors (13) cervicogenic patients reported more pain on the skin roll test, especially at the trapezius area. Our results also suggest that asymmetry between the symptomatic (more pain being on this side) and non symptomatic sides in the response to that test may be indicative of cervical dysfunction. Future studies should investigate the reliability of the skin roll test and its concomitant validity with pressure-pain threshold algometry.
Contrary to our expectation, the McGill Pain Questionnaire Short Form was not able to discriminate between the three headache groups. Even if it has been shown that the reliability for the memory of pain is fair (33), the fact that we relied on the patient's recall of the patient's pain could have been a factor that did influence the present results. Notwithstanding the fact that no clear clinical pattern was found, the use of the McGill Pain Questionnaire Short Form could, nevertheless, be of interest in depicting high affective pain component in individuals with headache (14).
When analysing our data, we found that there was a tendency for the score obtained on many of the variables evaluated in the migraine group, to be between that of the cervicogenic (nontraumatic) and of the control groups. Although, if care was taken in choosing subjects without neck pain, there were more musculoskeletal abnormalities in the migraine group compared to the control group. This finding was also demonstrated by Marcus et al. (34). Consequently, the hypothesis that cervical musculoskeletal abnormalities could be secondary to the migraine pathological process needs further investigation (35).
Even if those physical tests taken individually can probably not distinguish accurately the different headache populations, some of those tests could still be considered as potential outcome measures for the cervicogenic headache patient of traumatic or nontraumatic origin.
Most of the comparative studies that have looked at the impairments of cervicogenic headache did not specify the number of subjects that presented a traumatic onset. The results of our study suggest that the type of onset affects the magnitude of the musculoskeletal impairments associated with cervicogenic headache. If our data had been analysed using the nontraumatic and the post-MVA subjects pooled together, as is often done (8, 12, 13, 36), then the differences would have reached a statistically significant level for most of the variables. However, the present results demonstrated that most of the differences found can be attributed to the post-MVA group (Table 8). The differences encountered in the nontraumatic group, except on a few variables, are thus less obvious when compared to the migraine and to the control groups.
Conclusion
The results of this study showed significant limitations in cervical AROM (in flexion/extension and rotations), strength and endurance of neck flexors and in strength of the neck extensor muscles in post-MVA cervicogenic headache patients. Other variables including the asymmetry in the cervical rotation and in the pain reported during the skin roll tests showed higher results in the post-MVA group. However, in the nontraumatic cervicogenic group, only the strength of the neck flexor muscles was significantly different to that of the control group.
Our data suggest that there are enough differences between the cervicogenic post-MVA cervicogenic headache subjects and the nontraumatic cervicogenic headache subjects to warrant caution when analysing the combined data of these two subgroups together. The onset of the headache is therefore a potentially important variable that should be controlled when attempting to characterize the physical impairments associated with cervicogenic headache.
Footnotes
Acknowledgements
We would like to acknowledge the contribution of Dr Jacques Meloche (in memoriam), Dr Ruxandra Badescu and the other physicians at the Clinique de la Migraine de Montréal. We would like to thank also Dr Bonnie Swaine for her help with editing this manuscript.
This project was supported by a research grant from the Réseau Provincial de Recherche en Adaptation et Réadaptation (REPAR) of the Fonds de Recherche en Santé du Québec (FRSQ) and a grant from l'Ordre Professionnelle des Physiothérapeutes du Québec.