
Abstract
The objective of this study was to compare the exteroceptive suppression patterns of masseter and temporalis muscles in patients with primary and secondary headache disorders originating from peripheral joint dysfunction. We accomplished the temporalis and masseter exteroceptive suppression in 28 patients with migraine, 25 patients with chronic tension-type headache (CTH), 22 patients with temporomandibular joint (TMJ) dysfunction and 18 healthy controls. The onset latencies and duration of the first suppression period (S1) was not significantly different between the patients and controls. The duration of the second suppression period (S2) was shorter in patients with CTH, migraine (analysed during attack) and TMJ dysfunction than those obtained from controls. A distinctive finding was significantly prolonged onset latency in patients with TMJ over those obtained from patients with CTH and migraine. We concluded that the onset latency of the S2 period is a useful parameter in the differential diagnosis of primary and peripheral headache disorders.
Introduction
Electrophysiological techniques have been used to obtain additional data concerning pathophysiological aspects of the headache rather than diagnosis of pain disorders (1–3). Exteroceptive suppression of the masseter and temporalis muscles by the electrical stimulation of trigeminal nerve has been studied many times by different authors in patients with headache (4, 5). There are two different suppression periods after electrical stimulation of trigeminal nerve (S1 and S2) (6). The first period (S1) begins at about 10–12 ms and the second period (S2) begins at about 45–55 ms. The variations of the duration of the S2 period have been observed in patients with primary headache such as migraine and chronic tension-type headache (CTH) (7, 8).
There is some confusion in the literature about the methodology of recording and assessing exteroceptive suppression of jaw-closing muscles (9, 10). Additionally, there are contradictory results about the alterations of S2 duration in both controls and patients with headache (9–13). These discrepancies may result from the fact that S2 duration is influenced from many factors such as psychopathology, arousal, anxiety and some drugs (9, 10, 13, 14).
Temporomandibular joint (TMJ) dysfunction causes myofascial pain syndrome. This dysfunction may cause headache, especially during chewing and talking (15, 16). The headache due to TMJ dysfunction is a pattern of peripheral pain syndrome. However, the alterations in the central pain modulation have been discussed as a central mechanism of pain in patients with TMJ dysfunction (17). In this clinical entity, the suppression patterns of chewing muscles may contribute to the clinical diagnosis (18, 19). It is reported that absence of the S2 silent period was observed in patients with TMJ dysfunction (19).
This study was designed to compare the exteroceptive suppression patterns of the masseter and the temporalis muscles in patients with primary neurogenic (by means of migraine and CTH) and secondary headache disorders (by means of myofascial pain syndrome due to TMJ dysfunction).
Subjects and methods
Subjects
We studied 28 patients with migraine, six of whom (21.4%) were male, 22 (78.6%) female, and whose average age was 34.1±10.4 years. Mean disease duration was 9.1±6.1 years. Only four patients were classified as migraine with aura. Twenty-four were classified as migraine without aura. We did not consider the patients with aura as a different patient group and we analysed the data obtained from patients with migraine with and without aura together. Patients with migraine had no history related to other types of headache and evident psychopathology. The specific medication for migraine was prescribed after the electrophysiological investigations. The anti-depressants were discontinued at least 24 h before electrophysiological investigation. Thirteen were evaluated during both migraine attacks and painless periods. Five out of 13 patients evaluated during attack were analysed just after attack treatment with simple analgesics. Eight of them were analysed before their attack treatment. Five of them had holocranial headache, eight had unilateral located headache. Seven were recruited from our hospital staff. All of the patients with migraine had nausea and phono–photophobia during headache.
Twenty-five patients with CTH participated in the study. Three (12%) were male and 22 (88%) were female; the average age was 38.5±10.5 years. Mean disease duration was 7.3±6.6 years. All of the patients with CTH had headache during their electrophysiological investigations. The patients who had a history of migraine-type headache and the patients who had analgesic overuse were excluded. Patients with evident psychiatric disorders were also excluded. Fourteen of them had already used anti-depressant medication during clinical evaluation. The medication for headache such as analgesics and anti-depressants was discontinued for the last 24 h before electrophysiological investigation. All of the patients had holocranial headache activity. Nausea was not a constant accompaniment of headache in any of the patients with CTH.
Twenty-two patients with TMJ dysfunction and myofascial pain attended this study. One of these patients was male (4.5%), 21 were female (95.5%), and the average age was 37.1±13.7 years. Mean disease duration was 3.7±2.1 years. Five patients had bilateral, 17 patients had unilateral TMJ dysfunction. All patients complained of pain hypersensitivity to touch on the periauricular region during their electrophysiological registering. The patients with TMJ dysfunction had no history of migraine or CTH or any finding concerning neurological dysfunction. Headache frequency was very variable in patients with TMJ dysfunction. Most of them stated that their headache frequency was many times a day.
The data obtained from patients were compared with data obtained from 18 healthy subjects. Four (22.2%) were male, 14 (77.8%) were female. Average age was 38.6±12.2 years. Ages of controls and patient groups did not show statistical difference (P=0.6 CTH and controls, P=0.09 migraine and controls, P=0.23 TMJ dysfunction and controls). Control subjects were chosen from among our clinical staff. These subjects had not suffered from headache for at least 2 weeks before study and they had no history of migraine-type headache or CTH. Headaches were classified according to the criteria of the IHS Headache Classification Committee (1988) (20). The severity of the headache was documented with a visual analogue scale (VAS) of all of the patient groups. Informed consent was obtained from all of the subjects included in this study.
Electrophysiological methods
The exteroceptive suppression of masseter and temporalis muscles
Subjects were requested to be in a supine and relaxed position. During the electrophysiological investigation, subjects were instructed to clench their teeth forcefully. The stimuli were applied during this contraction period. The stimulating electrode was placed over the midline of the jaw. Both of the mental nerves were stimulated simultaneously from the jaw with an electrical impulse. The active recording electrode was placed over the belly of the masseter and temporalis muscles. For the temporalis muscle, the active electrode was placed over the anterior belly of the temporalis muscle. This point fits in front of the temporal hair line. Reference electrodes were placed on the arcus of the zygomatic bone. For recording, 1 cm diameter AgCl surface electrodes were used. Initially the suppression patterns of both masseter muscles were recorded. Thereafter, both temporalis muscles were investigated. Both sides of the face were recorded simultaneously. The oscilloscope sweep time was 200 ms.
First, exteroceptive suppression of masseter and temporalis were tested in control subjects. To determine the appropriate stimulation parameters which form consistent exteroceptive suppression, different stimulus intensities and different levels of tooth clenching were used in the control subjects. Initially, sensorial threshold intensity was determined. Each patient was asked when he felt the electrical stimulation. Thereafter, 1.5, two and three-fold sensorial threshold intensities were used for stimulation. Each stimulation intensity was applied with two strength levels of tooth clenching (submaximal and maximal). First, subjects were requested to clench their teeth with about half of their maximal strength (partial strength). Thereafter, maximal tooth clenching was used with each level of stimulus intensity. The most consistent suppression patterns were obtained by stimulation with two-fold sensorial threshold intensity and tooth clenching with maximal strength. When 1.5-fold stimulation intensity and partial muscle strength were used, S1 was absent in nine subjects, S2 could not be evoked in 12 subjects. With maximal tooth clenching and 1.5-fold sensorial threshold stimulation intensity, S1 and S2 could not be evoked in nine subjects. S1 could be evoked in all subjects when two-fold intensity was used. S2 period could not be evoked in two subjects during partial muscle strength when two-fold of sensorial threshold stimulation intensity was used. On the other hand, onset and end points of S2 period were not clear during partial muscle strength. Intermediate EMG activity was not evident when three-fold stimulus intensity was used. This EMG activity was absent in six subjects, so S1 and S2 periods could not be distinguished from each other when three-fold sensorial threshold was used. Therefore stimulus intensity was selected as about two-fold of the threshold intensity for the present study (Fig. 1). This level of stimulation intensity was not too painful and subjects were relaxed. At least five successive responses were recorded and superimposed. When onset and end points of S2 suppression periods were equivocal, 10–20 stimuli were recorded and averaged. Stimulus duration was 0.1 ms and amplifier filters were between 10 Hz and 10 kHz. To avoid habituation, the minimal time interval between the two stimuli was 10 ms. The duration of S1 and S2 periods and onset latencies of the S1 and S2 periods were calculated.

S2 periods obtained from control subjects recorded by different stimulus intensities during tooth clenching with maximal strength. (1.5 (a), two (b) and three (c)-fold sensorial threshold intensity.)
Data analysis
The determination of onset and the end of the S2 period was sometimes difficult because only slight muscle activity was seen frequently during the S2 period. We measured the silent interval from the end of the intermediate EMG activity to the beginning of former EMG activity as the S2 period. The EMG activity exceeding 20% of maximal amplitude of EMG signal was not considered as silent period. Additionally, absolute S2 durations (when S2 period was defined as any reduction of EMG activity) were analysed. The determination of S1 period was relatively easier than S2 because S1 period was more stable than S2 and S1 period did not include any electromyographic activity. To determine the S2 duration, mean durations of five responses were calculated. In addition, the duration and onset latency of S1 duration and onset latency of S2 duration were analysed. We obtained these data from both the temporalis and the masseter muscles. The interside differences of the duration and the onset latencies of the S2 period were calculated in healthy controls. Increased interside difference of S2 period was considered when the S2 duration difference between right and left side exceeded +2 SD. In addition, peak-to-peak amplitude of muscle responses between S1 and S2 periods (intermediate EMG activity) was analysed. For this analysis, a signal which had the greatest electromyographic activity was used.
Statistical analysis
SPSS 10.0 statistical package was used for statistical analysis. Data were summarized as mean (±SD). Multivariate analysis of variance and Tukey post hoc test were used to compare headache groups. Age was accepted as coefficient factor in these tests. In each headache group correlation analysis was performed to examine the linear relationship between the duration of S1 and S2 periods and onset latencies of the S1 and S2 periods. The maximum type I error rate level was accepted as %5. The correlation between electrophysiological data obtained from masseter and temporalis muscles was analysed with Spearman correlation analysis.
Results
The headache frequency was between 17 and 30 days per month (mean 24.3±4.3) in patients with CTH. The attack frequencies were between 2 and 10 per month (mean 5.0±1.9) in patients with migraine. The number of headache days in patients with migraine was 6.2±2.2 days (2–12) per month. The headache frequency was higher in patients with CTH (P<0.001). Headache intensity VAS score was 6.6±1.4 in patients with CTH, 7.8±1.2 in patients with migraine. Headache severity was higher in patients with migraine (P<0.0001). Headache severity was not correlated with S1 and S2 durations in patients with CTH and migraine during attack (r=0.23 and 0.16, respectively). In patients with TMJ, headache frequency was variable. All patients with TMJ dysfunction had daily headaches. VAS score was 6.5±1.2 in patients with TMJ dysfunction. There was no correlation between clinical characteristics (severity and frequency) and the duration of S1 and S2 periods (P>0.05).
The duration of S2 period was correlated with stimulus intensity in control subjects (r=0.55, P=0.001). S1 duration was not changed with stimulus intensity (P>0.05).
The duration of S2 period obtained from masseter muscle was 47.1 ms (±7.1) and onset latency of S2 period obtained from masseter muscle was 48.5 ms (±5.7) in the control group. Table 1 shows the onset latencies and the durations of S1 and S2 periods in patients with headache and normal controls. Figures 2 and 3 demonstrate the durations and the onset latencies of S2 periods. Absolute S2 durations were 49.4±8.4 (for controls), 43.1±8.5 (for CTH), 43.5±8.2 (for migraine), 38.4±9.2 (for TMJ dysfunction). Absolute values of S2 period were not compared with each other additionally.
The duration and onset latencies of S2 periods obtained from patients and controls

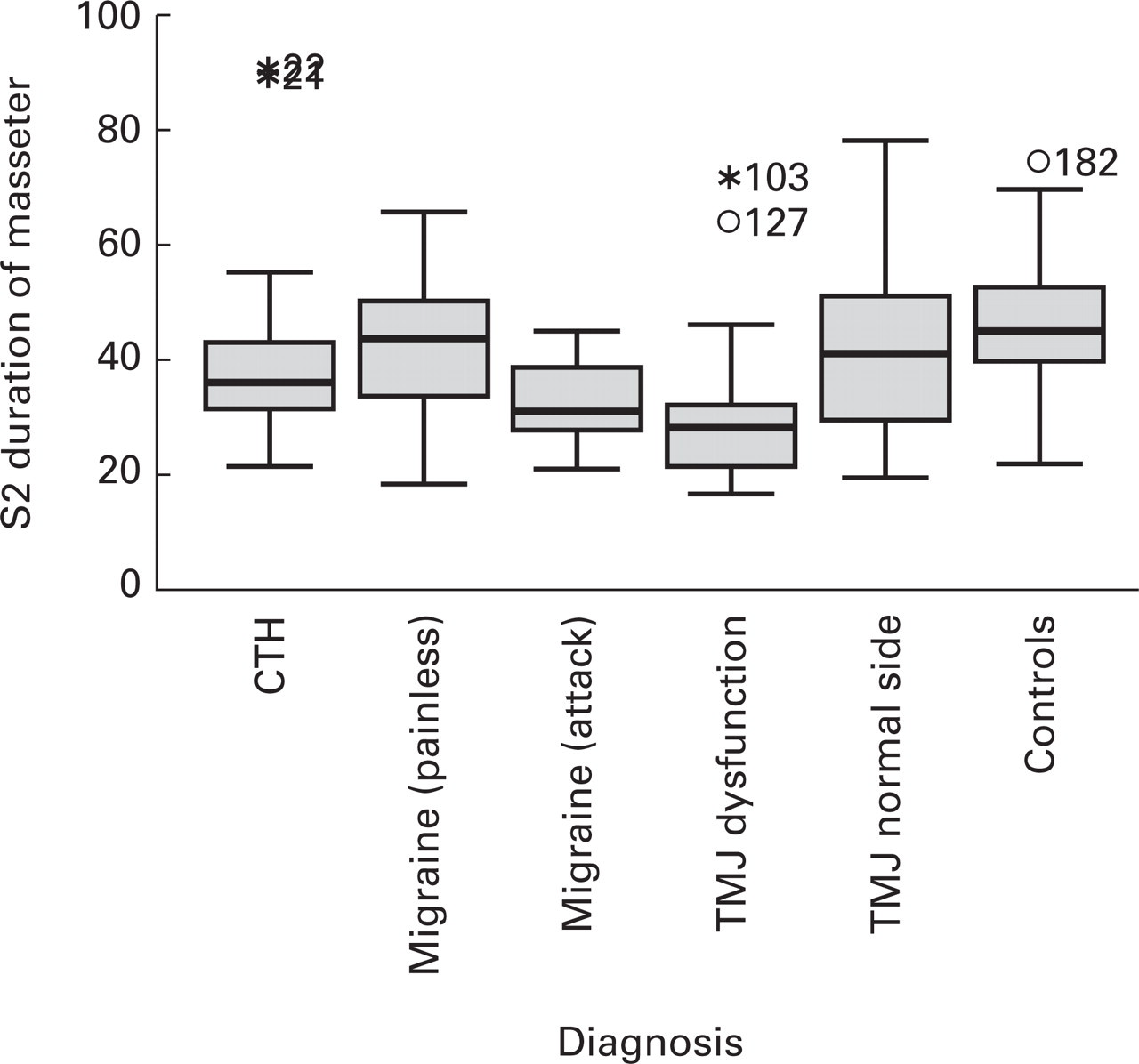
The durations of S2 periods of controls and patients with different kind of headache disorders.
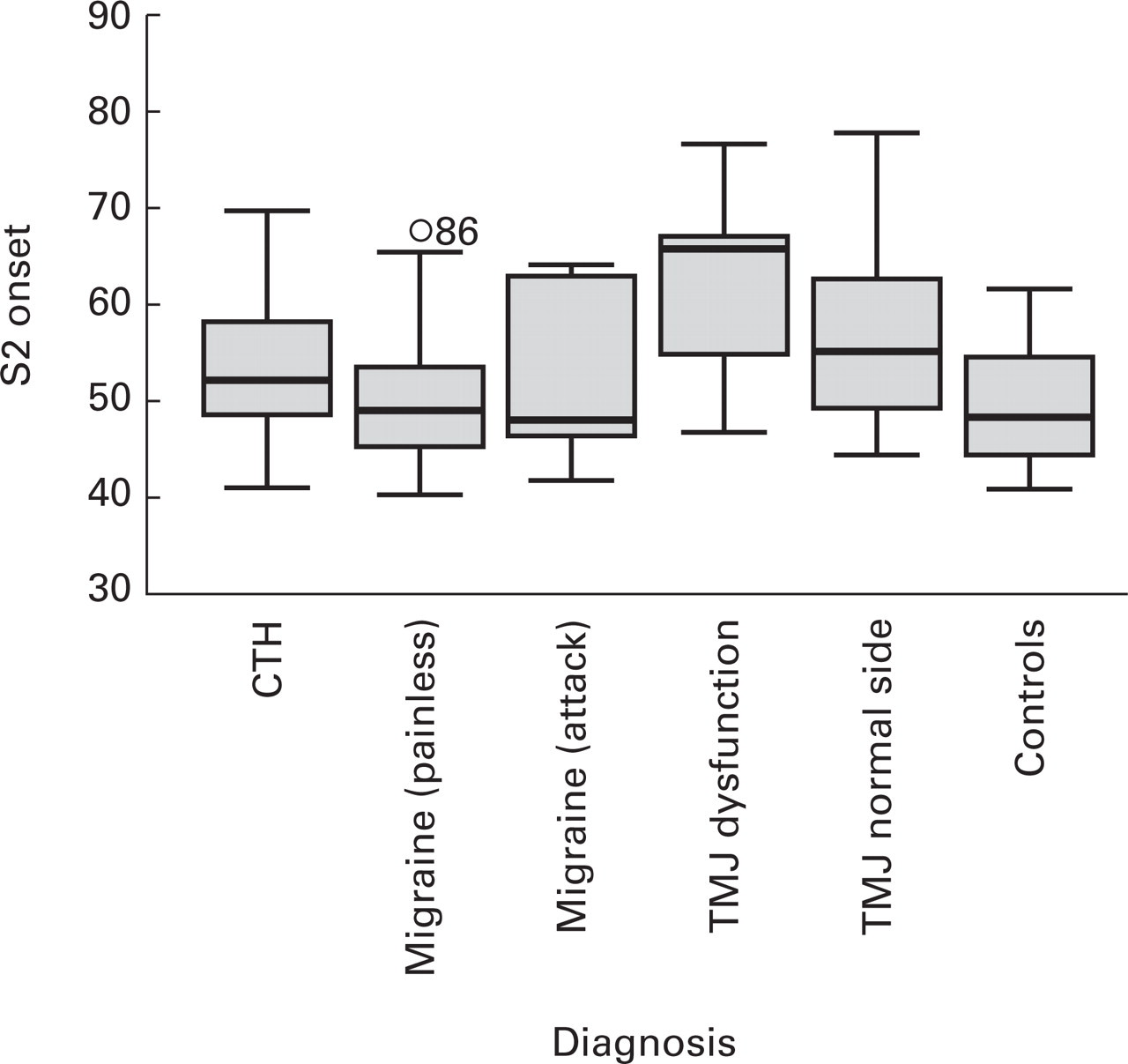
The onset latencies of S2 periods of controls and patients with different kinds of headache disorders.
The onset latencies and durations of S1 and S2 periods obtained from masseter and temporalis muscles were correlated with each other in both controls and patient groups (r=0.62 and 0.72, respectively). The durations and onset latencies of S1 period obtained from masseter and temporalis muscles were also correlated (r=0.74 and 0.58, respectively). The upper limit of interside difference of the duration of S2 period was 3.8 ms (95% confidence) in normal controls. In addition, the upper limit of interside difference of the S2 onset latency was 5.5 ms (95% confidence).
In patients with CTH, the S2 period was significantly shorter than that obtained from controls (P=0.0009). In addition, the suppression of masseter and temporalis muscles was not total in eight patients with CTH. The onset latencies of S1 and S2 periods and duration of S1 periods did not show significant differences between patients with CTH and controls (P>0.05). In eight patients with CTH, interside differences of the duration of S2 period were increased. On the other hand, only one patient with CTH showed increased interside difference in onset latency of S2 duration.
In patients with migraine (during the painless period), no statistical difference was observed in the electrophysiological parameters compared with electrophysiological data obtained from controls (P=0.64). Thirteen patients with migraine were investigated electrophysiologically again during their headache period. The S2 duration obtained during the attack period of patients with migraine was significantly shorter than that obtained from controls and from patients with migraine during the painless period (P=0.001 and P=0.035). During the attack, five patients with migraine showed increased interside differences in the duration of the S2 period. During the painless period, three patients showed increased interside differences in the duration of the S2 period. Only one patient, who was investigated during the attack, showed prolonged interside difference in the onset latency of S2 period.
There was no difference between patients with migraine (investigated during the painful period) and CTH in terms of electrophysiological data. The duration of the S2 period obtained from patients with migraine during attack was shorter than that obtained from patients with CTH, but this difference did not reach the level of statistical significance (P=0.09).
On the other hand, S2 period was significantly shorter in patients with TMJ dysfunction than that obtained from controls (P<0.0001). The durations of S2 period obtained from patients with TMJ dysfunction were similar to those obtained from patients with migraine (during painful period) and CTH (P>0.05) (Fig. 2).
In patients with myofascial pain syndrome due to TMJ dysfunction, the onset latency of S2 period was significantly prolonged when compared with controls (P<0.0001), patients with migraine (P<0.0001) and patients with CTH (P<0.0001). In addition, the onset latency of S2 period obtained from the painful side was also more prolonged than that obtained from the other side in patients with TMJ dysfunction (P=0.009). All of the patients with unilateral TMJ dysfunction showed increased interside differences in the duration and the onset latency of the S2 period. Four of five patients with bilateral TMJ dysfunction showed increased interside difference in the duration of S2 period. Two of the five patients with bilateral TMJ dysfunction showed increased interside differences in the onset latency of S2 duration (Figs 3 and 4).

Exteroceptive suppression patterns obtained from a patient with migraine (a,b). The potentials on the right were recorded during attack (b). Prolonged onset latency of S2 period were seen in patients with bilateral temporomandibular joint (TMJ) dysfunction (c) and in a patient with right-sided TMJ dysfunction (d). Upper potentials are from right side, bottom potentials are from left side.
There was no statistical difference in the amplitude of muscle response, appearing just after S1 period, between controls and patients with migraine, CTH and TMJ dysfunction.
Discussion
There are many studies evaluating the brain-stem reflexes in patients with different kinds of headache disorders (1–5, 7, 8, 18, 19). There are a few studies comparing exteroceptive suppression periods in patients with different types (primary and peripheral) of headache (5, 8). However, to our knowledge, suppression periods in patients with primary headaches and patients with TMJ dysfunction have not previously been compared. In this study our primary aim was to compare these electrophysiological techniques in primary and peripheral type headache disorders.
In the current study, our results demonstrate that the shortening of S2 period has been observed in both the peripheral and primary headache disorders. There was no correlation between clinical characteristics (severity and frequency) and suppression periods. The onset latency of S2 period may provide useful information in the differential diagnosis of these headache disorders. Prolonged onset latency of S2 period observed in patients with TMJ dysfunction was considered an important finding.
There is some confusion in the literature about the methodology of recording and assessing suppression patterns (9, 10). Additionally, different results have been obtained from different studies (8–10, 13). This confusion may originate from many factors effecting the duration of S2 period, such as psychiatric disorders, anxiety and some drugs (9, 13). It seems that relaxation of subjects is important during the test. Therefore, we planned to set a methodology which caused minimal patient discomfort and good patient adaptation. At the beginning of the study, we evaluated different stimulation and recording procedures at the different levels of tooth clenching in normal subjects. Altered sensorial thresholds were previously reported in patients with TMJ dysfunction (21). Determination of stimulus intensity using sensorial thresholds may diminish the individual variabilities effecting S2 duration. When we used two-fold sensorial threshold intensity to evoke suppression periods during maximal tooth clenching, the suppression patterns were more consistent and clear than those obtained by other methods (Fig. 1; Table 2). In this study, we averaged at least five successive (consistent) responses, but this number was increased if responses were not consistent. Paulus et al. also averaged five traces and analysed artefact-free responses (8). Nevertheless, the durations of S1 and S2 periods obtained from our healthy controls were similar to some previous studies (9, 11). However, the duration of S2 period was shorter than ours in normal subjects in some studies (5, 10, 22). The normal values of S2 duration obtained from some studies were within a broad spectrum (between 12.1 and 47 ms) (13). Our stimulation parameters caused minimal discomfort in all subjects. Lower stimulation intensities and distant stimulation points may provide more clear suppression patterns. Additionally, it seems that our procedure was time saving. In the present study, blinded analysis of suppression periods could not be accomplished. This is a limitation. Simultaneous recording of both masseter and temporalis, distant stimulation points and different stimulation parameters were major methodological differences in our work.
S1 and S2 suppression periods obtained by different stimulation intensities during tooth clenching with different strength levels

∗The level of tooth clenching strength.
Paulus et al. observed a low degree of exteroceptive suppression in patients with CTH, but this abnormality was not observed in patients with other types of headache (such as postlumbar puncture headache and headache due to meningitis) (8). The shortening or abolition of S2 period have been reported by many investigators (1, 9, 11). Wang et al. concluded that the abnormalities of S2 period can contribute to the diagnosis of CTH (4). On the other hand, Zwart and Sand reported normal S2 suppression periods in patients with CTH (5). However, their patient group was small (11 patients). There are also some studies concluding that there was no alteration in S2 duration in patients with CTH (10, 22, 23). Neufeld et al. also used the same procedure. However, S2 duration was shorter in patients with CTH than that obtained from controls in their study. These discrepancies can be encountered in different studies when different and even similar methodologies are used. Additionally, the duration of the suppression periods could be influenced by different factors such as psychiatric disorders and medication (9). The studies accomplished with blinded methods demonstrate that there was no difference in S2 duration in patients with CTH. Therefore, we suggest that blinded methods should be used in further studies to test our results. We also observed significant shortening of S2 duration in our patients with primary headaches and TMJ dysfunction. Our additional observation was the alterations of S2 onset latencies in patients with primary and peripheral type headache disorders.
The results obtained from some electrophysiological studies concerning patients with migraine are also equivocal (1, 5, 7, 8). Zwart et al. observed that the durations of S1 and S2 periods were within normal limits (5). Protracted S2 period was also observed in patients with migraine (1). On the other hand, there are some studies detecting abnormal shortening of S2 suppression period in patients with migraine (1, 7). Nakashima et al. observed a low degree of exteroceptive suppression in patients with migraine (11). We analysed the electrophysiological data during the attack and the painless period in 13 patients with migraine. Our findings may reflect the hyperexcitability of trigeminal motor nucleus and altered activity of bulbar inhibitory interneurones in patients with chronic primary headache. The observation of the existence of similar suppression patterns of S2 period in patients with CTH and migraine suggests that these clinical entities have similar pathophysiological mechanisms. Nakashima and Takahashi also stated that their electrophysiological findings could be evidence for a pathophysiological relationship between CTH and migraine (11).
The differential diagnosis of various types of headache may sometimes be difficult. Myofascial pain syndrome is a good example of a peripheral headache disorder which originates from the musculoskeletal system (15, 16). Nevertheless, there are some reports concluding that the alterations in the central pain mechanism have a potential role in patients with TMJ dysfunction (17, 21). This clinical condition has sometimes been confused with primary headache disorder in the clinical evaluation of patients with headache. In this study, we observed a significantly shortening of S2 period in patients with TMJ dysfunction. On the other hand, the onset latencies of S2 period were significantly prolonged when compared with both controls and patients suffering from CTH and migraine. Increased interside differences in the duration of S2 period and the latencies of S2 onset were more common in patients with TMJ dysfunction than in those obtained from patients with migraine and CTH disorders. The increased interside differences can result from frequently asymmetric disease activity in TMJ dysfunction. This finding suggests that the onset latency of the S2 period may be an important electrophysiological parameter in differential diagnosis of peripheral and central headache disorders. The absence or shortening of the S2 period is a frequent finding in patients with TMJ dysfunction (19, 24, 25). Hussein and McCall reported longer suppression periods in patients with TMJ dysfunction compared with controls (19, 26). However, their results were not corrected for clenching level. They observed that suppression periods after electrical stimulation appeared to be shorter at maximal tooth clenching than at 50% of tooth clenching (19). Nonetheless, different methodologies and results were reported in the literature which dealing mainly with TMJ dysfunction (19). These alterations are probably due to instability of S2 duration, which may be influenced by a variety of many factors mentioned above. De Laat et al. concluded that S2 duration can not be used as a diagnostic tool because of high variability, and the studies evaluating the exteroceptive suppression pattern in experimentally induced muscle pain could provide better insight into the synaptic circuitry and the afferent fibres involved in the facial reflexes (19). We are not insistent about S2 suppression pattern as a diagnostic tool in patients with TMJ dysfunction. However, it can be used as a supplementary tool in differential diagnosis of equivocal patients. On the other hand, the shortening of S2 period in TMJ dysfunction may support the role of central pain mechanisms in myofascial pain syndrome.
There are many reports concerning the mechanism of the generation of S1 and S2 periods. According to these studies the S1 and S2 periods elicited from jaw-closing muscles have the same afferent and efferent pathways (9, 27). These studies conclude that S1 and S2 periods are produced by the activation of inhibitory interneurones located in the brain-stem. The exact mechanism and the location of responsible interneurones in the generation of the S2 period are not yet certain. These interneurones are probably located at the bulbar reticular formation (9, 28). Since the onset and the duration of S1 period did not show any difference between patients and controls, the prolongation of the onset latency of S2 period in patients with TMJ dysfunction probably results from an altered activity of inhibitory interneurones located at the bulbar reticular formation. This altered activity may be due to modulation of central pain mechanism. A possible explanation for the prolongation of S2 onset latency observed in patients with TMJ dysfunction may be related to a deficiency in small diameter thinly myelinated and unmyelinated trigeminal afferent fibres (C and Aδ fibres) which may be responsible for pain sensation in patients with TMJ dysfunction. Abnormalities in muscle strength observed in TMJ dysfunction may cause altered excitability in the afferent nerve fibres or interneurones located at the bulbar reticular formation responsible for pain sensation.
In conclusion, our data support the concept that migraine and tension-type headache share similar pathophysiological mechanisms, since we found similar suppression patterns in both disorders. The mechanisms of pain probably have some differences in TMJ dysfunction; nevertheless, it seems that altered activity of bulbar inhibitory interneurones plays some role in both the myofascial pain syndrome due to TMJ dysfunction and primary headaches. Additionally, peripheral mechanisms, which probably result from prolonged latency in S2 period, may have a role in myofascial pain syndrome. The onset latency of S2 period may be helpful in the differential diagnosis of peripheral and primary headache disorders.
Footnotes
Acknowledgements
This study was presented as an oral presentation at the 5th International Symposium of Clinical Neurophysiology and 18th National Congress of Clinical Neurophysiology.