
Abstract
The purpose of the present study was to evaluate neuropsychological performance and regional cerebral blood flow in migraine patients, and to investigate whether possible abnormalities in any of these fields could be related to the chronicity of the disease. The sample included 60 patients and 30 healthy control subjects; all of them were subjected to a complete neuropsychological assessment, including emotional variables. In addition an interictal 99Tc-HMPAO SPECT was performed in 56 patients and 15 controls. Disturbances in memory, attention and visuomotor speed processing were observed among migraineurs experiencing higher frequency of attacks and in those with a long history of migraine. Anxiety levels were higher in patients than in controls and were positively correlated with attack frequency, but not with cognitive test scores. Brain perfusion abnormalities, mostly hypoperfusion areas, were found in the 43% of patients; poorer performance in two tests, measuring verbal and visual memory, respectively, was found in these patients.
Introduction
In our clinical practice we have frequently found migraine patients who complain of some degree of memory impairment in relation to their previous performance; common statements of this kind include inability to remember telephone numbers or addresses, forgetting what they were going to do or say in a specified moment and inability to recall the name of a specific object, i.e. anomia. As these assertions are usually expressed by people otherwise healthy, we thought that possible memory deficits could be related to their migraine process. This clinical finding led us to review literature concerning potential cognitive deficiencies in migraine and was the starting point of the present study.
On reviewing medical literature we found that articles dealing with the neuropsychological performance of patients with migraine during interictal periods were relatively scarce and showed discrepant findings, as while some authors found alterations in cognitive performance in migraine patients, others did not.
Among investigators who found deficiencies in the cognitive processing of migraineurs, Zeitlin and Oddy (1) were the first who carried out a controlled comparison between 19 migraine patients and 19 healthy subjects, and concluded that migraineurs showed lower scores in memory and information-processing tests than subjects in the control group. Two years later, Hooker and Raskin (2) evaluated the neuropsychological performance of 16 patients experiencing migraine with aura, 15 patients experiencing migraine without aura and 15 control subjects; migraine patients exhibited poorer performance than controls. D'Andrea et al. (3) studied memory function in 20 children suffering common migraine and in 20 healthy children, observing that the former experienced impairment both in short-term and in long-term memory in relation to the latter. Messa et al. (4) examined verbal and visual memory in 25 patients with common migraine and in 10 control subjects, finding that patients scored lower than controls in several administered tests. Finally, Le Pira et al. (5) examined cognitive abilities in 15 patients suffering migraine with aura, 16 patients suffering migraine without aura and 14 healthy controls, detecting defects both in verbal and visual memory in both groups of patients.
Burker et al. (6) published the first study with negative results in a sample of 47 female patients, 20 of them with classic migraine and 27 with common migraine, who were compared with 24 female controls. Later, Leijdekkers et al. (7) studied the neuropsychological functioning of 37 female migraine patients, 11 of them with aura and 26 without aura, who were compared with 34 female controls without finding any evidence of deterioration. Likewise, Mulder et al. (8) evaluated the cognitive and psychomotor capacity in 10 migraineurs with aura, 20 migraineurs without aura and 30 healthy controls and found similar results in every group.
Considering that psychological factors and/or personality traits could influence the neuropsychological performance, some of the above mentioned authors studied also some of these aspects. It must be stated, in this respect, that many authors have found that neuroticism personality profile is higher among migraine patients than in healthy subjects (9, 10), and that persons with migraine have also been found to be at increased risk for affective and anxiety disorders (10, 11).
Zeitlin and Oddy (1) applied to their patients the Middlesex Hospital Questionnaire and found that migraine patients scored higher in free-floating anxiety, obsessionality and somatic complaints, but there was no correlation between data from these scales and cognitive results. D'Andrea et al. (3) examined the personality profile and anxiety levels among their children, finding that those with migraine had significantly higher anxiety levels. Le Pira et al. (5) administered the Hamilton Depression Scale and, although scores from patients both with migraine with aura or without aura were higher than those of the control group, the difference did not reach statistical significance. Burker et al. (6) found among their patients higher scores in the hypochondria, hysteria and paranoia MMPI scales, but no difference in relation to controls in trait nor in state anxiety levels. On the contrary, in the sample of Leijdekkers et al. (7), migraine patients had higher trait and state anxiety levels, as well as more depressed mood and low vigour scores than controls; there was no correlation between any of these parameters and the results of cognitive tests.
Examining all the data closely, we thought that the main difference existing between authors who found cognitive affectation in migraine and those who did not, was the selection of the sample: the patients of the studies of Zeitlin and Oddy (1), Hooker and Raskin (2), D'Andrea et al. (3) and Messa et al. (4) came from headache clinics, whereas those of Burker et al. (6), Leijdekkers et al. (7) and Mulder et al. (8) were recruited either among the general population or students, respectively. Concluding that cognitive disturbances could be characteristic of a subgroup of patients, perhaps those with more frequent and disabling attacks and/or those with a longer history of headaches, we decide to undertake a study with a wide sample of patients covering the clinical spectrum of migraine: from patients whose migraine was just diagnosed to those who have suffered the disease during most of their life, and from patients with very infrequent headaches to those with near daily headaches.
The authors of the first controlled study about cognitive efficiency in migraine (1) based most of the rationale of their trial on the fact that the proportion of abnormal CT scans in migraineurs seems to be significantly higher than in the normal population, a fact that has been repeatedly acknowledged (12, 13), and postulated that brain damage could lead to permanent and perhaps cumulative neurological deficits. However, they did not perform any kind of neuroimaging technique in their patients, and none of the ensuing publications contemplated the possibility of a possible relationship between neuroimaging abnormalities and neuropsychological performance. As it is not known if potential cognitive abnormalities in migraineurs reflect a persistent neurological deficiency, we thought that it could be interesting to study interictal regional cerebral blood flow (rCBF) in our patients. This can be done either by single photon emission computed tomography (SPECT) or by positron emission tomography (PET); this latter method is extremely expensive and not easily available; to our knowledge, there are not PET studies in migraine during attack intervals. As for SPECT, as it can be seen in Table 1, many of the studies that used it to investigate interictal brain perfusion in migraineurs (14–21) found abnormalities that were categorized as hypoperfusion in many cases and just as ‘asymmetries’ in others; it was even suggested in one of the articles that the observed abnormalities could be correlated with the severity of the disease (19).
Summary of studies concerning interictal SPECT in migraine
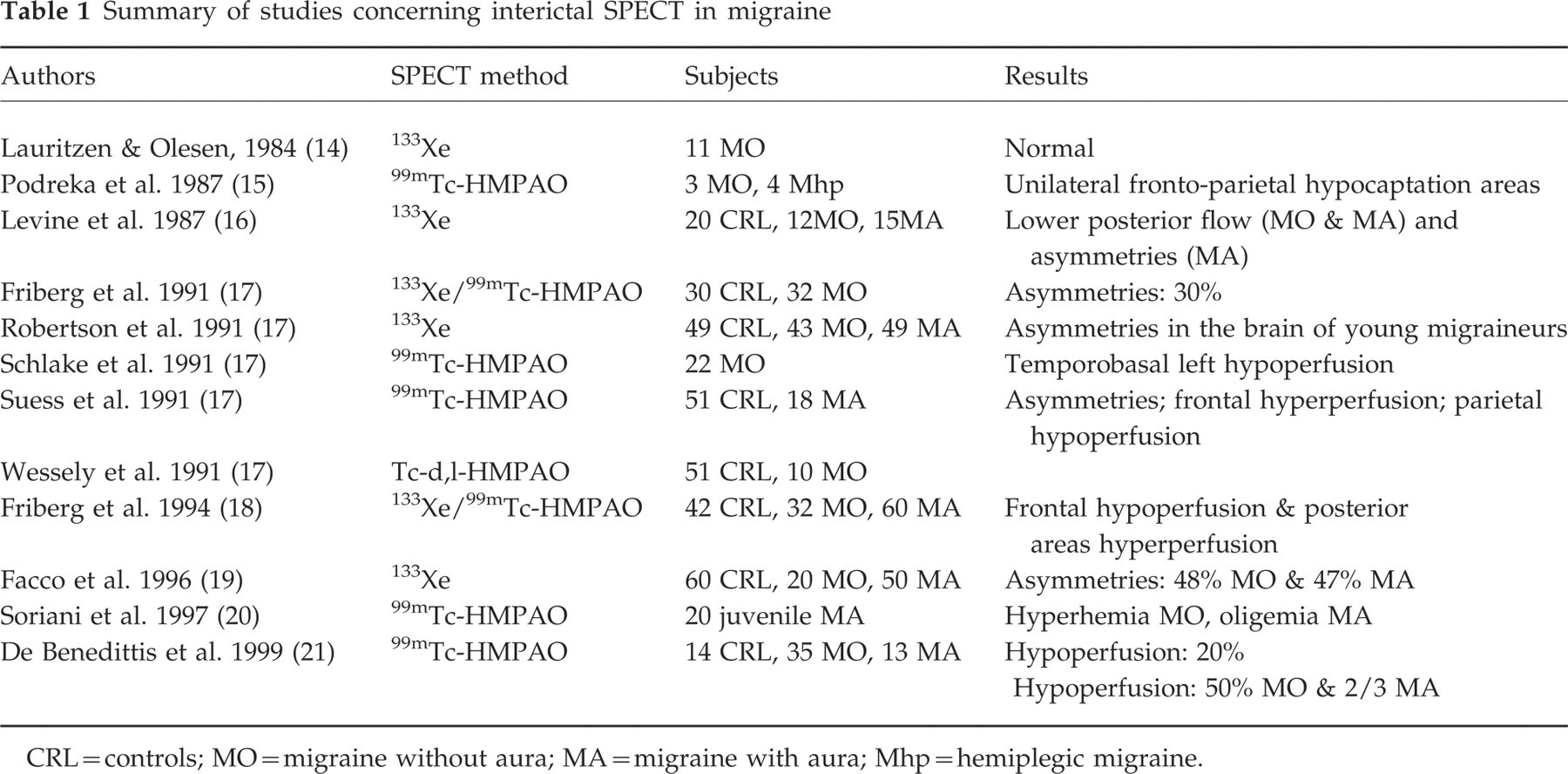
CRL=controls; MO=migraine without aura; MA=migraine with aura; Mhp=hemiplegic migraine.
Therefore, the present work was designed in order to fulfil the following objectives:
To evaluate the neuropsychological performance of migraine patients during headache-free periods, with special emphasis on cognitive and emotional functioning.
To assess interictal cerebral perfusion by applying a 99Tc-HMPAO SPECT.
To investigate if possible abnormalities in any of these evaluated areas could be related to the clinical characteristics of the illness, specifically to the frequency and intensity of the attacks, and the length of migraine history.
Methods
Subjects
The study was carried out in 60 patients with migraine, 38 women and 22 men, aged from 15 to 68 years; 10 of them experienced migraine with aura and 50 migraine without an aura. Most of the patients were recruited among those attending the headache clinic of our Institute; others, specially those with infrequent headaches who rarely sought medical advice, were found from relatives and/or friends of the former group. The exclusion criteria included a migraine history less than 1 year, an IQ≤80, suffering from another coexistent type of headache or any concomitant organic or psychiatric disease which, in the opinion of the investigators, could alter significantly the neuropsychological performance. Migraine diagnosis was established according to IHS criteria (22); the frequency, the length and the severity of their migraine attacks were recorded. Patients' data (MI group) were compared with those of 30 healthy subjects (CRL group), similar in age range, gender distribution and educational status (Table 2 and Fig. 1); subjects included in the control group were also selected from friends and relatives of the patients as this was considered the best way to maintain the homogeneity in relation to the social background and cultural level of the sample.
General data of the sample
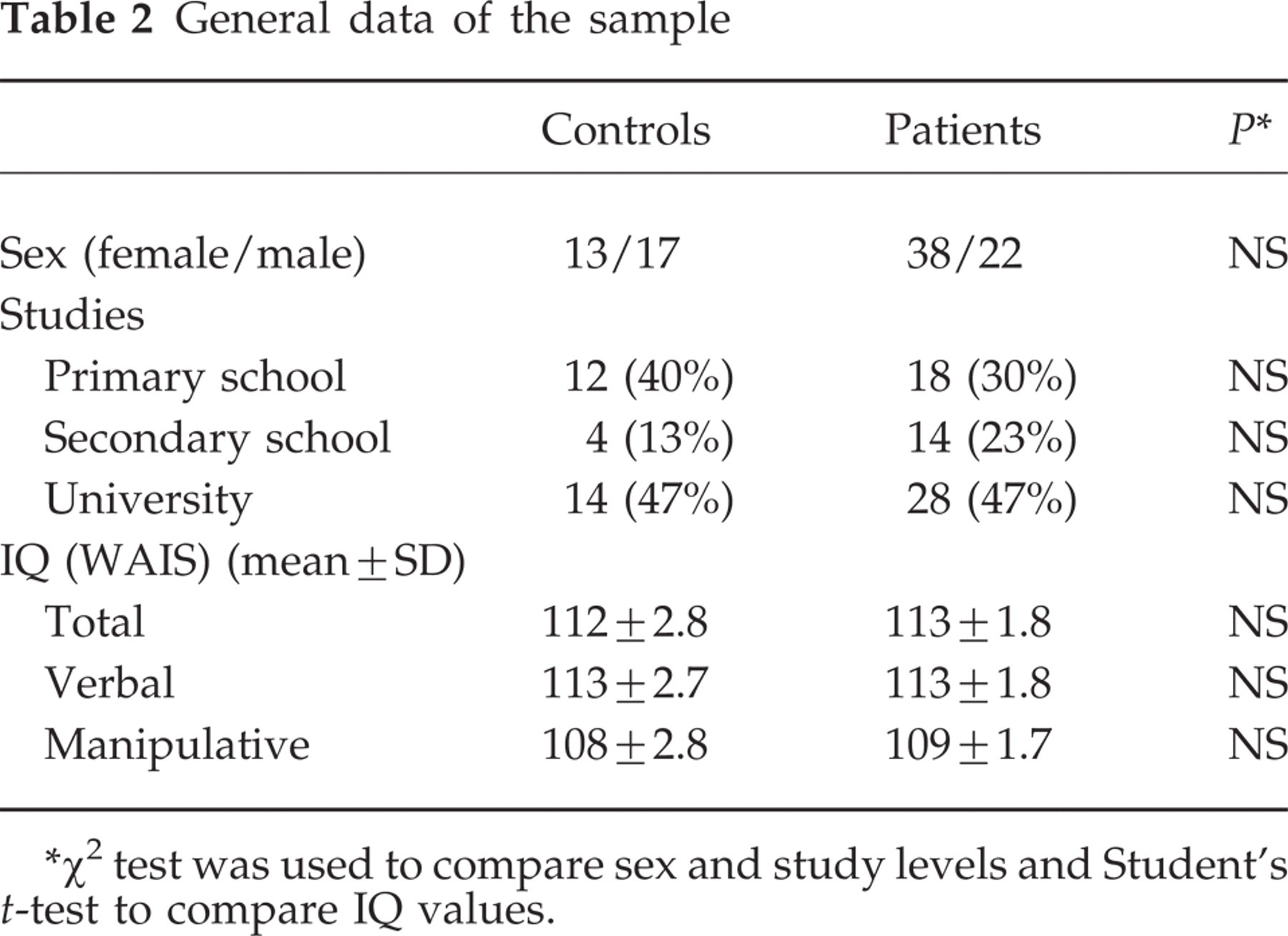
∗χ2 test was used to compare sex and study levels and Student's t-test to compare IQ values.

Age range and mean values in migraine (MI) and control (CRL) groups.
Patients were not receiving any prophylactic medication when they were enrolled in the study; they were treated later, if it was indicated, when either the neuropsychological assessment and the SPECT had been performed; most of them used symptomatic medication, triptans and/or NSAIDs to control their headaches. Although a potential interference of drugs on neuropsychological performance and/or SPECT results was considered unlikely, patients abusing ergotamine or analgesics were not considered for this study.
Procedure
All of the subjects completed an extensive neuropsychological evaluation. As reversible cognitive decline has been observed during migraine attacks (23, 24), in patients the evaluation was always performed during headache-free intervals. The assessment was usually carried out in a single session whose mean duration varied from 120 to 180 min. Nevertheless, if the subject complained about the excessive difficulty of the task, it was done in two sessions on consecutive days; this latter case was, however, the exception. The battery included the following tests, all of them considered of high specificity and sensitivity (25, 26), which are summarized in Table 3:
Neuropsychological battery description

General intellectual functions. Wechsler Adult Intelligence Scale (WAIS).
Attention. Digits backwards (subtest from WAIS): This test consists of a digit series that the examiner reads aloud and the subject repeats in reverse order; the length span increases from two to seven digits. Stroop test: This measures the subject's concentration and his/her effectiveness at inhibiting distractors. The test requires three trials: (i) reading colour words; (ii) naming printed colours; and (iii) reading a printed colour when the ink printed is in a different colour than the name of the colour word. An interference index can be calculated by the number of items read in each trial within a 45-s time limit. Strub and Black letter list: This examines the ability to sustain and focus attention. A sequential auditory letter list is administered, with instructions for the subject to tap only when the examiner reads the letter A. The number of correct answers and errors (omissions, intromissions) are calculated. Trail Making Test (Parts A and B): This measures the subject's ability to mentally follow two sequences and the flexibility to shift between them. The subject must connect consecutively numbered circles (Part A) and then track a number and letter sequence with alternations between sets (Part B). Errors and time to complete each part are recorded. Picture completion (subtest from WAIS): The subject must identify the missing part in a series of incomplete common designs.
Memory. Digits forwards (subtest from WAIS): This consists of the repetition of a digit sequence (in pairs from two up to nine numbers) exactly as the examiner reads it. The test stops when the subject fails a pair of the same sequence. The obtained score is considered as the working memory span. Rey Auditory Verbal Learning Test (RAVLT): Fifteen common words are administered for five trials with recall required after each presentation and after a 30-min delay. It provides a learning curve and a learning index of short-term and long-term memory. Logical memory: This test requires the short-term and delayed (15 min) reproduction of the first history included in The Wechsler Memory Scale. Visual reproduction (subtest from the Wechsler Memory Scale): This is the VI subtest of the Wechsler Memory Scale (WMS). After a 10-s exposure to a card with one or two geometrical figures the subject attempts to draw what he remembers; this is done immediately and again after a 15-min interval. Short and delayed reproduction of Rey-Osterrieth's Complex Figure Test: The delayed recall of Rey's Complex Figure (after 5- and 15-min intervals) is considered as a measure of long-term visual memory. The test assesses the quality of the reproduction (from 0 to 36 points) and the time necessary to complete it. Benton Visual Retention Test (BVRT): Immediate visual recognition memory was investigated using a multiple choice version of the BVRT. After a 10-s exposure to a geometrical figure (target), the subject is required to identify the target stimulus between four very similar designs. Fifteen trials are necessary in order to complete the task.
Visuomotor speed processing. Digit Symbol Substitution Test (subtest from WAIS): A number series (from 0 to 9) is paired with a sequence of nonsense symbols. After a few practice trials the subject matches each digit with its symbol as quickly as possible for 90 s. Visual reaction time: This measures the time that the patient takes to press key when a visual stimulus appeared in either visual field. The mean reaction time over 20 responses is recorded.
Motor coordination. Luria Sequential Motor Tests. (a) Learning and reproduction of a sequence of movements (fist/edge/palm). The subject must learn this movement and do it automatically within a 60-s time limit. (b) Motor programming and inhibition (tap gently when the examiner taps powerfully and vice versa). Rapid alternating hand movements: The subject opens the right hand and closes the left hand simultaneously as quickly as possible for a minute. Rhythm test: The examiner taps on the table a rhythm sequence from two to six hits that the subject must repeat.
Visual perception. Poppelreuter Test: Two cards with five superimposed common objects are shown; the subject must name the overlapping 10 figures. Benton's Recognition Form Test/Visual Form Discrimination: A target set of geometrical stimuli are administered next to four very similar designs. The task consists of recognizing the figure identical to the target. Rotations and distortions can be detected along the 16 trials included in this test. Benton's Facial Recognition Test: We used the 16-item version of this test. The subject matches faces identical to a target face. All of these identical faces belong to the same person photographed with different lighting conditions. From one up to three correct responses are required in each trial.
Abstract reasoning. Similarities (subtest from WAIS): The task consists of explaining what a pair of words (fruits, animals, objects, etc.) have in common. The instructions and corrections norms are included in the WAIS' manual.
Mental calculation. Arithmetic (subtest from WAIS): This test is considered as a measure of arithmetic reasoning problems, although its score is very influenced by difficulties in immediate memory, attention and concentration. The scores are calculated according to WAIS manual norms.
Praxias. Rey's Complex Figure Reproduction: The copy of this picture allows assessment of visuoconstructional abilities. The quality of the reproduction (ranged from 0 to 36 points) and the time necessary to complete it are scored. Block design (subtest from WAIS): Red and white blocks are administered to construct a figure identical to the designs printed on a card. The pictures are graded in difficulty. The corrections' norms are shown in the WAIS manual.
Emotions. Beck Depression Inventory: We used a 19-item version of this test as severity of depression measure. Taylor Manifest Anxiety Scale: A 50-item questionnaire was designed by Taylor as an anxiety measure. This scale asks specifically for psychophysiological and somatic symptoms, which are very typical in migraine patients.
To evaluate regional cerebral blood flow, a 99mTc-HMPAO SPECT was performed in 56 patients and in 15 out of the 30 healthy control subjects. The SPECT was scheduled according to the hospital availability, in such a way that it could be done either before or after the neuropsychological evaluation. Patients were instructed to specify if they experienced a migraine attack the same day on which the neuroimaging was appointed in order that the procedure could be postponed; only in one case was this delay required and in this case the SPECT was carried out several days later. The whole time necessary to perform the SPECT was approximately 45 min, including the tracer injection and the tomography completion.
The evaluation of the SPECT was visual, as we had not available any standard computerized method of analysis. This was an important limitation of our study as it implies a substantial degree of subjectivity; to minimize the bias the rater was always the same and was blinded to the identity of the subject, not knowing if he/she was a patient or a control.
Analysis
Global comparison of test scores between controls and migraine patients was done by applying a Student t-test for unpaired data. When the migraine sample was split up according to the frequency of the attacks or the duration of the illness, the comparison between controls and migraine subgroups was carried out by means of an analysis of variance (
All the statistical analyses were two tailed and considered significant when P-value was equal or lower than 0.05; they were performed using the GraphPad Prism version 3.00 for Windows.
Results
Cognitive variables
Global comparison between migraine and control groups
When the results of the tests were compared between migraine patients and controls, a poorer performance was found among patients only in the visuomotor speed processing as measured by the reaction time (mean values: 255 ± 25 vs. 287 ± 54 s, respectively, P=0.0002).
When we compared the neuropsychological performance of patients suffering migraine with and without aura we did not find any relevant difference in their respective scores; it must be stressed, however, that both groups were numerically mismatched, 10 vs. 50 subjects, a factor that did not favour a balanced comparison.
Data related to headache intensity and frequency
The severity of migraine attacks was classified as 1 when patients categorized them as being mostly slight or moderate, and as 2 when they were categorized mainly as severe or unbearable. Only the reaction time showed significant differences among the three groups (mean values: 255 ± 25 for CRL, 288 ± 62 for group 1, and 286 ± 47 for group 2, P=0.0102); however, post-hoc analysis indicated that differences applied only to the comparison between patients and controls but not between both patient groups.
According to the mean frequency of the attacks, the patient sample was divided into the following three groups:
those with less than three attacks per month;
those with three to nine attacks per month; and
those with 10 or more attacks per month who could be considered as suffering transformed migraine according to the classification proposed by Silberstein et al. (27).
As can be seen in Table 4, highly significant differences were found in several tests and subtests, related to verbal memory (RAVLT and WMS logic memory), short- and long-term visual memory (WMS visual reproduction), working memory (digits forwards), visuomotor speed processing (reaction time), and attention (Stroop test and picture completion). In addition, in several of these tests a statistically significant linear trend to show progressively worse scores related to headache frequency was observed among migraine groups (Table 4); the reaction time exhibited the most evident degree of impairment, showing a highly significant positive linear trend among columns, with the quickest values in the control group and the slowest ones in the transformed migraine group (Fig. 2).
Neuropsychological assessment in relation to migraine frequency (mean ± SD)
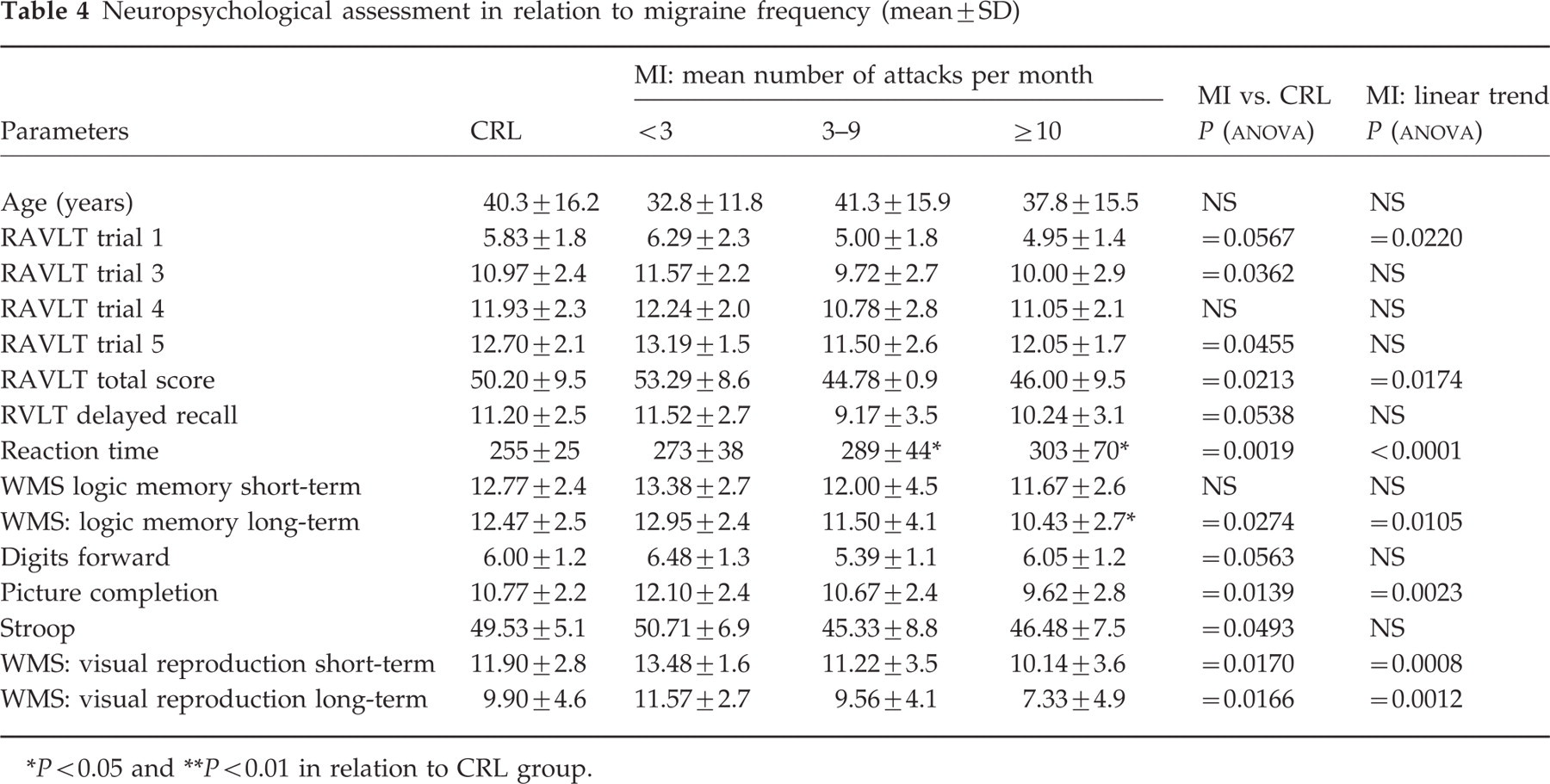
∗ P<0.05 and
∗∗ P<0.01 in relation to CRL group.

Reaction time scores in controls and in migraine patients classified according to attack frequency.
Data related to migraine duration
According to the length of migraine history patients were divided into two groups: those who had experienced attacks for 20 years or less, and those who had experienced attacks for more than 20 years. Table 5 shows that there were significant differences between controls and both patient subgroups, again concerning verbal memory (RAVLT and WMS logic memory), short- and long-term visual memory (WMS visual reproduction and Rey-Osterrieth's Complex Figure Test), visuomotor speed processing (reaction time and digit symbol substitution test), and attention (picture completion, Trail B and Stroop tests); when the duration of the illness was correlated with the test scores in migraine patients, a significant linear relationship was found in most of the cases (Table 5).
Neuropsychological assessment in relation to the lenght of migraine (mean ± SD)

∗ P<0.05 and
∗∗ P<0.01 in relation to CRL group.
Emotional variables
As is shown in Table 6, there were no relevant differences in Beck scores distribution between controls and patients when stratified as no depression (scoring ≤10 points), slight depression (scoring 11–16 points) or overt depression (scoring ≥17 points) (28). In the evaluation of anxiety, on the contrary, we found significantly higher scores in patients than in controls (19.8 ± 1.4 vs. 14.3 ± 1.6, respectively, P=0.0224); additional analysis of the Taylor's test data indicated that the level of anxiety was not related to the duration of migraine but showed a positive relationship with the frequency of the attacks (Fig. 3). The anxiety scores were not correlated with tests results.
Stratification of Beck's depression scores

∗Chi-squared test.

Taylor's test scores in controls and in migraine patients classified according to attack frequency.
Cerebral perfusion
In contrast to the data for the control group, in which only two (13%) subjects had an abnormal SPECT, a heterogeneous distribution of the tracer was found in 25 (43%) of the migraineurs, six of them with aura and the remaining 19 of them without aura, being a significant difference between both groups (P=0.0348, Fisher exact test). In the overwhelming majority of the cases, these abnormalities reflected hypoperfusion, strictly localized in some cases and concerning multiples areas in others; this last pattern was qualified as multi-ischaemic. A brief description of the observed alterations is given in Table 7, and Fig. 4 shows a SPECT from one of the patients exhibiting multiple hypoperfusion areas.
Abnormal SPECT findings

CRL=control; MA=migraine with aura; MO=migraine without aura.

Typical migraine SPECT pattern exhibiting multiple hypoperfusion areas.
In relation to patients with normal SPECT, those with abnormal SPECT had longer duration of disease (22.3 ± 14.6 vs. 18.7 ± 11.3 years), and the proportion of people with more than three attacks per month was higher (73% vs. 54%); however, these differences did not reach statistical significance.
No differences were found in test scores between patients with normal and abnormal SPECT. However, when we compared the results from patients with normal and abnormal SPECTs with those of control subjects significant differences were found in two tests:
The 5 trial of RAVLT: mean values were CRL: 13.2 ± 1.7, MI normal: 12.8 ± 1.8, and MI abnormal: 11.6 ± 2.2; P=0.025. Also, significant poorer performance was found between MI abnormal and CRL groups with a P<0.05 by the Tukeys' and the Newman–Keuls' post-hoc tests.
Short-term visual reproduction: mean values were: CRL: 13.1 ± 2.4; MI normal: 12.6 ± 3.0, and MI abnormal: 10.8 ± 3.4; P=0.044. No differences were found between pairs of groups when applying the post-hoc tests.
Discussion
Cognitive variables
Global comparison between migraine and control groups
The fact that the increase in the reaction time was the only parameter indicative of cognitive alteration in the whole sample of patients suggests that the visuomotor speed processing is the first signal of a dysfunction in the neuropsychological performance of migraine patients. It must be stated that visuomotor speed processing is also usually one of the first cerebral functions altered in cerebral pathologies dealing with white matter abnormalities, such as multiple sclerosis, dementias or Parkinson's disease (25). Although migraine is usually considered a benign disease, as we mentioned earlier in the introduction, white matter hyperdense foci have been observed (12, 13).
Data related to headache intensity and frequency
The deficiencies observed in relation to headache intensity were minimal but it was again the reaction time test in which patients with severe migraine scored worse than control group subjects.
On the contrary, very relevant differences were found when the data were analysed in relation to attack frequency (Table 4). These differences cannot be attributed to discrepancies in the age of the subjects as mean values were similar in every studied group, although patients with infrequent headaches tended to be, as a whole, slightly younger than controls and patients of the other groups. Hence, it seems likely that the impairment in the neuropsychological performance can be related to the presence of repetitive migraine attacks.
The observed cognitive deficiencies were always centred in attention, memory and visuomotor speed processing, without any modification in motor coordination, visual perception, abstract reasoning, mental calculation, nor praxias. The fact that the deficits were observed both in verbal and in visual memory and not only in the acquisition processes but also in the delayed recall, indicates that migraine-associated impairment could be related to both cerebral hemispheres and several cerebral areas; this finding agrees with the multiple locations of the hypoperfusion areas observed in the SPECT.
Our data agree, in general, with those of the authors who also found abnormalities in the neuropsychological testing of migraine patients (1–5), even if it is difficult to establish a good parallelism with their results given the wide variety of tests employed by the different investigators; only Hooker and Raskin (2) found poorer performance, in addition to one subtest of the WMS and in the digit-symbol substitution test, in tests measuring motor performance. Interestingly, impairment in verbal memory has also been recently described by Jorge et al. in patients suffering cluster headache (29). However, none of these authors investigated the possibility that memory and attention deficits were related to the frequency of headache attacks.
Data related to migraine duration
A very important point to consider when analysing the performance deficiencies found in relation to the length of migraine history is the age of the subjects: as cognitive performance deteriorates with age, results from patients with a very long history of headaches could have been related to their age rather than to the duration of the migraine. However, mean age in controls and in patients with more than 20 years of migraine did not differ relevantly (Table 5), so that the impairment detected in attention, memory and visuomotor speed processing should be attributed to migraine not to the process of ageing. Yet, patients with less than 20 years of headache were significantly younger than controls and this difference could have contributed to the fact that only the reaction time was altered in this group of patients.
The possibility of a relationship between cognitive deficits and the clinical manifestations of migraine was also investigated in three publications. Zeitlin and Oddy (1) elaborated a severity index of migraine that did not correlate with patients' scores; however, the IHS has advised recently against the use of headache indexes in migraine that are not considered a meaningful way of evaluation (30); on the other hand, their sample included only 19 patients and 13 controls, a number probably too restricted to allow the evaluation of differences in migraine severity. Leijdekkers et al. (7) did not find any significant relationship between both parameters; their patient sample, 37 patients, was greater than the one of the former authors, although probably not enough to establish a meaningful correlation; in addition, they selected patients with a migraine history of at least 7 years and a maximum age of 50 years old, both conditions that restricted the range of duration of the disease; our sample included 60 patients with a migraine history ranging from 1 to 51 years of illness, with a mean value of 20 ± 13 years, which was higher than the mean value of 18.4 ± 7.8 years of Leijdekker et al. Likewise, Le Pira et al. (5) did not observe any significant relationship between cognitive defects and length of migraine history but their sample, 14 patients, was really limited; they do not mention the range of illness duration in their article.
Emotional variables
The association between migraine and anxiety and/or depression is by no means new: as stated earlier, the prevalence of anxiety and depressive disorders among patients with migraine is high. In a survey examining the prevalence of anxiety and depressive symptoms in migraine patients, Devlen (31) found a markedly higher prevalence of the former in relation to the later, data that agree with our findings. We were not surprised to find that Beck's depression scores were very similar in migraineurs and in controls, given that we did not allow participation in the study of patients with clinically relevant depression; three of our patients have previously experienced major depression episodes but were currently euthymic.
Although none of our patients could be diagnosed with a specific anxiety disorder, many of them can be described as anxiety-prone subjects. The relationship observed between Taylor scores and attack frequency makes sense when considered from a clinical point of view but it is difficult to interpret: on the one hand, stressful events are among the most important precipitating factors of migraine attacks (32, 33), so that higher anxiety scores could act as a trigger for a higher number of attacks; on the other hand, it seems logical than patients with higher frequency of headaches experience also higher levels of anxiety; probably both factors are strongly interrelated and cannot be easily disentangled one from the other. It seems relevant, in this respect, that in the sample of Leijdekkers et al. (7), who found higher anxiety levels among migraineurs, the mean duration of the disease was around 18 years and the mean frequency of attacks was around 30 per year, whereas in the sample of Burker et al. (6), whose patients did not show relevant anxiety, the values of these parameters were significantly lower; the samples of both studies included only females and none of the authors observed significant cognitive deficiencies.
As happened in other studies (1, 6, 7), we did not find any correlation between depression nor anxiety scores and cognitive test scores. It seems therefore that the poorer cognitive performance exhibited by migraine patients was not conditioned by the emotional variables.
Cerebral perfusion
The high incidence of SPECT abnormalities among migraine patients indicates that these are probably related to the disease process; areas of hypoperfusion during headache-free periods have been also described by De Benedittis et al. (21) in almost half of their patients experiencing migraine without aura and in two-thirds of their patients experiencing migraine with aura, percentages that are very similar to those that we have found in our sample; their series included 35 migraineurs without aura, 14 ones with aura and 14 healthy subjects, a number high enough to discard the possibility that interictal rCBF flow anomalies in migraine are just accidental, as has been suggested by previous investigators (17). Friberg et al. (18), examining the cerebral perfusion in a wide sample of patients, found also frequent interictal asymmetries that were not restricted to a particular area; as in our case, they did not find any correlation between asymmetry scores and the duration of migraine nor the frequency of attacks.
It has been postulated that persistent rCBF abnormalities in migraine can be the reflection of vascular factors involved in the pathogenesis of the headache; however, as decreased brain perfusion can be the result either of reduction in brain flow or diminished neuronal activity, an alternative explanation is that these changes could be the consequence of frequently repeated migraine attacks; this last possibility has been previously pointed out by Levine et al. (16), and would be coherent if a link between neuropsychological disturbances and brain hypoperfusion areas can eventually be established. Our data indicate that hypoperfusion is seen preferably in patients suffering chronic and/or severe migraine, a suggestion also stated by Facco et al. (19), but the number of our patients with SPECT abnormalities was not enough to confirm this hypothesis. As publications concerning interictal rCBF in migraine are relatively scarce, further investigations should be carried out to evaluate if persistent regional hypoperfusion is associated with migraine severity and/or chronicity.
The fact that patients with abnormal SPECT scored lower than those with normal SPECT in two tests of memory strongly suggests a relationship between brain hypoperfusion and cognitive defects; however, a wider sample should be necessary to confirm this potential relationship. This would also allow us to study if there is any kind of correlation between the functional deficits and the location of hypoperfused areas observed in migraine patients.