
Abstract
A double-masked randomized controlled study with cross-over design compared the effectiveness of precision ophthalmic tints in the prevention of headache in migraine sufferers. Seventeen patients chose the colour of light that optimally reduced perceptual distortion of text and maximized clarity and comfort. They were later given glasses with spectral filters providing optimal colour under conventional white lighting ('optimal' tint) or glasses that provided a slightly different colour ('control' tint). The tints were supplied in random order, each for 6 weeks, separated by an interval of at least 2 weeks with no tints. Headache diaries showed that the frequency of headaches was marginally lower when the ‘optimal’ tint was worn, compared with the ‘control’. The trial extends to adults with migraine, the results of a previous double-masked study demonstrating, in children with reading difficulty, beneficial effects of precision tints in reducing symptom frequency. In the present study, however, the effects are suggestive rather than conclusive.
Keywords
Introduction
Visual symptoms such as scintillations, scotomata and fortification spectra are a prominent feature of attacks of migraine with aura (1). Photophobia accompanies most (perhaps more than 90%) attacks of migraine, both those with and those without aura (2), and various kinds of visual stimuli can also trigger an attack (3, 4). Wilkins et al. (5) have shown that certain patterns of stripes can be uncomfortable to look at, causing a sensation now known as pattern glare (6). Patients who suffer from frequent headaches report more discomfort and visuo-perceptual distortions when looking at these patterns. The discomfort is manifest by an aversion of gaze rarely demonstrated by those with non-migrainous headaches but common in those with migraine (7). Pattern glare and headaches can also be caused by repeated lines of text, which produce a pattern that resembles stripes (8). Weston (9) reported the possibility of eye-strain caused by repetitive patterns and suggested the use of coloured glasses in order to subdue the glaring effect of the pattern.
There have been several studies of visual function in patients with migraine, some supporting the idea that there exist visual deficits (10, 11), not all of them reliable: Wray et al. (12) vs. Palmer & Chronicle (13). Some of the deficits have been taken as support for the notion of a cortical hyperexcitability (5, 12), disputed elsewhere (14). Whatever the basis for the visual deficits, they are subtle, sometimes related to duration of illness (14, 15) and may involve colour vision (16). This may explain why Chronicle and Wilkins (17) were able to show that people with migraine show consistent preferences for colour of illumination when reading and thereby differ from age- and sex-matched controls.
Meares (18) and Irlen (19) have described a syndrome that includes symptoms of visual fatigue, such as eye-strain, blurring and headache, reduced by the use of coloured filters. A number of studies have reported benefits from using coloured filters (20–22), some in migraine (23), although a well-controlled study, which used only a small range of tinted lenses, failed to show any benefits (24). One difference that tends to separate the studies that have shown benefits from those that have failed to do so is that the former allow for an individual choice of specific tint (precision tint). A double-masked randomized placebo-controlled trial of precision tints in children with reading difficulties found a reduction in symptoms of headache and eye-strain with individually prescribed coloured filters (14).
Wilkins et al. (26) have developed a technique for precision ophthalmic tinting using a coloriser (‘intuitive colorimeter’) that illuminates a page of visual material (text) with coloured light and allows the observer to select a colour by changing the hue and saturation without altering luminance. The effects of the colour on perceptual distortion and discomfort can be assessed subjectively and the colour individually optimized to reduce distortion and improve clarity while the eyes remain colour-adapted. Beneficial effects of precision tints obtained using this technique have been reported on reading, eye-strain and headache (21, 27–29) and users have reported a significant reduction in the frequency of their headaches and epileptic seizures (28, 30), as well as a decrease in severe reading problems (29).
People whose migraine headaches are triggered by light, or who suffer from photosensitivity during their headaches, are routinely prescribed tinted lenses by eye-care professionals and this practice has face validity. The research that has been outlined above suggests that using individually prescribed coloured filters may be more helpful than the conventional practice of using a neutral grey, or sometimes brown, tint. In other words, tints for people with migraine may need to be individually prescribed with some degree of precision. This is the hypothesis that we investigated.
Pilot study
In an initial open trial we followed six males (age range 10–53; mean 27.8 years) and 14 females (age range 15–73; mean 36.6 years) suffering from migraine of various aetiologies for which they had been given precision spectral filters, individually prescribed at the optometric practice of one of the authors (BJWE).
The procedure for the prescription of precision tinted lenses has been described above and in more detail elsewhere (27, 31). In brief, the clarity and visual comfort of text illuminated by coloured light was determined by alternately varying hue and saturation by small amounts under conditions in which the eyes remained colour adapted. Spectral filters that provided that colour under conventional white lighting (fluorescent, CIE type F3) were then provided.
The patients were followed-up for 4½ years to 8 months after they received the glasses (mean of 2 years 1 month). An assessment of the effectiveness of coloured glasses was made from the patient's report, and in particular, the extent to which they believed use of the glasses had improved the quality of their lives and ability to carry out activities they were previously unable to perform. Sixteen patients (80%) reported that they still used their glasses. Fifteen patients (75%) reported a decrease in the frequency of headaches since they had been prescribed the glasses, four (20%) indicated no change in frequency, and one (5%) said that headaches and migraine had increased in both frequency and severity.
Thirteen patients (65%) reported a significant reduction in their reliance on medication following the use of the glasses. Five (25%) had stopped the medication altogether. These patients were among those who reported most benefit from the glasses.
Four patients reported that they were able to halt the progressing severity of the headache, and even its onset, by wearing the glasses as soon as they felt a headache was about to begin. Eleven patients indicated an absence of photophobia and eye-pain when glasses were worn, but not at other times.
The following study was conducted to assess the extent to which the above findings reflect a direct physiological effect or can best be attributed to a placebo effect.
Double-masked cross-over study
In so far as possible, the design of the study followed the guidelines for drug trials dealing with migraine prophylaxis specified by the International Headache Society (33). The study was a double-blind, randomized, controlled trial with cross-over design. The IHS criteria were used for the selection of patients. Migraine had been present for more than 1 year, usually considerably longer. A 1-month baseline was allowed for, but in the event insufficient data were forthcoming. The treatment period was 6 weeks. This is less than the 3 months recommended for drug trials by the IHS but the effects of tints on indexes such as reading speed are immediate (25). A ‘washout’ period of at least 2 weeks was used, during which glasses were returned for re-glazing. Patients were permitted to take their symptomatic treatment. Patients were not seen except at the beginning and end of the trial in order to maintain the blind. A headache diary was used and the number of days with symptoms was taken as the assessment parameter. The study was submitted to, and approved by, the Ethics Committee of the Institute of Optometry, London, where most patients were examined.
Methods
Participants
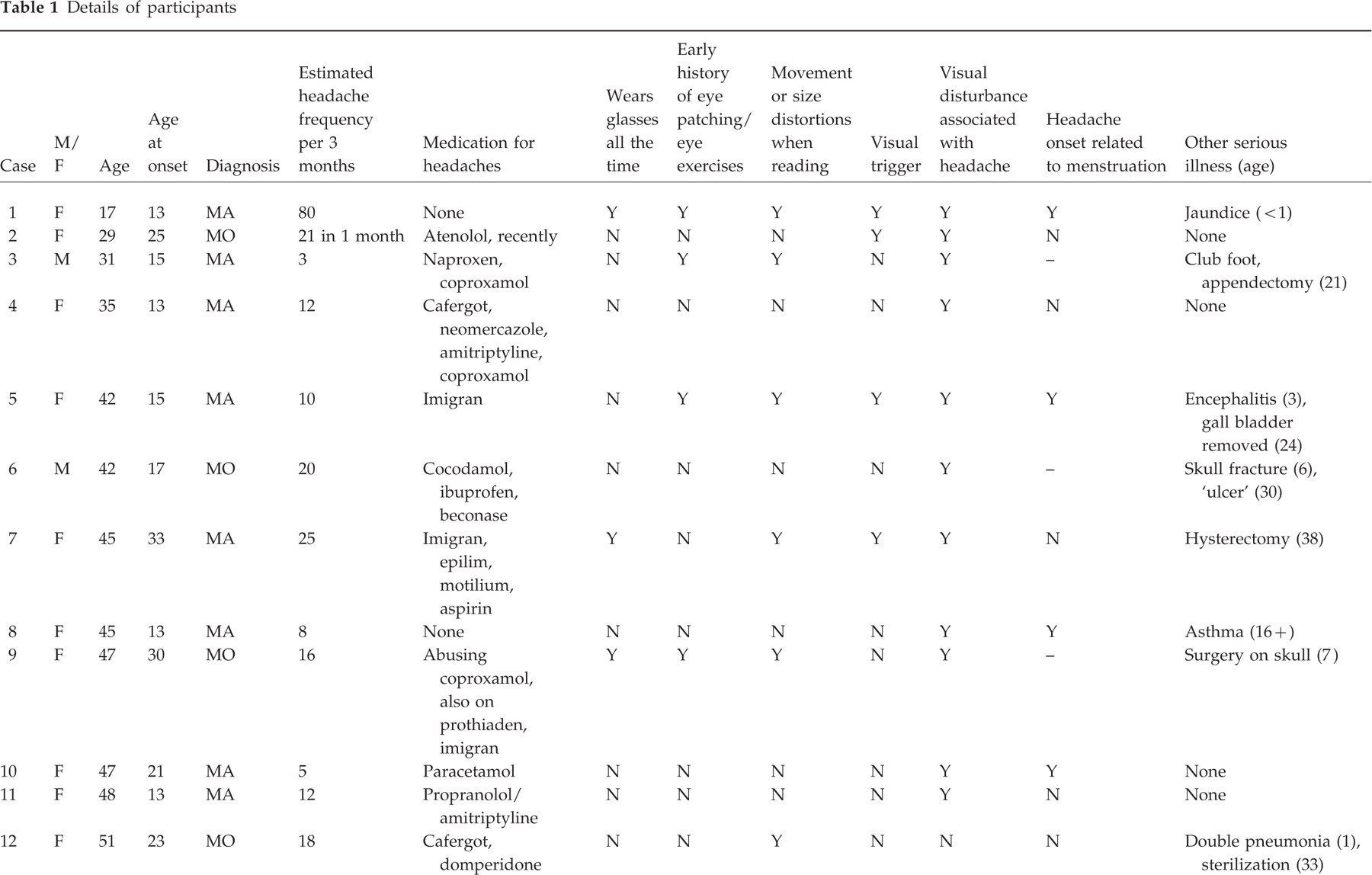
The 21 participants were referred from various sources (neurologist, GP, optometrist). Eighteen were female and the mean age was 44 years (range 17–54 years). Seventeen patients completed the trial and details are given in Table 1. The diagnoses were reviewed by a neurologist. Twelve patients had migraine with aura (MA), and five migraine without aura (MO). All but four had eight or fewer attacks monthly; case 2 had, without any clear explanation, experienced 21 in a recent month and was started on Atenolol just before recruitment; cases 16 and 17 were probably abusing ergotamine; and case 1 had developed continuous migraine-type headache, again without any clear explanation. In addition, case 9 was probably abusing dextropropoxyphene.
Details of participants

The patients were instructed to continue their medication as usual during the trial.
All the patients gave a family history of migraine. None of the patients had a history of epilepsy, although one (case 12) had suffered convulsions as a child. None had undergone eye operations, although four had experienced monocular patching or eye exercises as a child. Eight experienced spatial or chromatic distortion of text when reading, and a further four experienced blurring. All but two experienced perceptual disturbances in association with their headache. All had associated photophobia, and all but two phonophobia. Seven patients reported visual triggers in response to the open question ‘What sort of things do you think bring on your headaches?’. Six patients had had no serious illness. The illnesses experienced by the remaining patients included hysterectomy (3), appendectomy (2), jaundice, mastectomy, gall bladder removal, encephalitis, skull fracture, and possible craniotomy, the last three early in life.
All the participants had been examined using coloured overlays over text. In previous studies (e.g. 26), the response to coloured overlays when reading has predicted the likely response to coloured glasses, although the optimal colour for overlays and lenses is not the same (34). Subjects were eligible for the study if (i) they had used a coloured overlay whilst reading for at least a month and reported that this improved their symptoms of perceptual distortion and eye-strain when reading; and (ii) they did not already wear tinted spectacles (excluding the commonplace use of sunglasses). The latter exclusion criterion was necessary because participants who already wore glasses were provided with clip-over tinted lenses.
Procedure
The examination with overlays (used in the screening of subjects) has been described elsewhere (29). In brief, the subjects were shown 10 differently coloured overlays placed over text and were asked to judge whether any of the colours improved the clarity of the text beneath. Four patients were eliminated on the basis that none of the colours improved the clarity of text.
Overlays provide a surface colour and the eyes are adapted to the colour of ambient illumination. In contrast, the eyes are colour-adapted when coloured glasses are selected by varying the colour of light in the intuitive colorimeter. The optimal colour under the two conditions has been shown to differ (34). At the outset of the examination patients were informed that the colour of the overlay they had used was not related to the colour of light they would find helpful.
The subjects underwent a full optometric assessment, the results of which are described by Evans et al. (35). They were then assessed using the intuitive colorimeter, as described above and in greater detail elsewhere (31). Using the standard techniques, the colour that subjectively best reduced the perceptual distortion and maximized the clarity and visual comfort of the text was determined by a process of successive approximation (alternately varying hue and saturation by small amounts) under conditions in which the eyes remained colour adapted (31). A variety of different colours were therefore presented in succession and the patient was not informed which would be chosen as optimal. The ‘optimal’ chromaticity was inferred by the examiner from the patient's responses to successive presentations, and the examiner avoided testing the optimal chromaticity last. A pair of glasses was made with lenses that matched this ‘optimal’ chromaticity under the CIE F3 illuminant, i.e. when worn under conventional ‘white’ halophosphate fluorescent lighting the glasses gave white surfaces a chromaticity matching that selected in the colorimeter. By triangulation, there were two chromaticities that had similar saturation (suv) as the ‘optimal’ tint but differed in chromaticity by a CIELUV colour difference of 78 (about six just-noticeable-differences). One of these was chosen at random and used as a ‘control’ chromaticity. A pair of ‘control’ glasses was made with lenses that matched this chromaticity under the CIE F3 illuminant as closely as possible. The chromaticity of the ‘optimal’ lens and that of the ‘control’ lens are shown in Fig. 1 joined by a line, separate lines for each participant. The identity of each participant is shown by the number beside each symbol. The variation in chromaticity with lighting has been the subject of another study (Wilkins et al., unpublished observations). Suffice it to say here that the variation was unlikely to have been sufficient to have eliminated the beneficial effects of the optimal tint vis-a-vis the suboptimal.

Chromaticities of the tinted lenses used in the study. The chromaticity of each patient's ‘optimal’ tint is shown by a square symbol and connected by a line to the chromaticity of the suboptimal ‘control’ tint. The numbers identify the patients as per Table 1.
Three weeks after the initial appointment the patient was sent a pair of glasses that contained the ‘optimal’ or ‘control’ tint, selected at random by collaborators in the ophthalmic tinting company, without the knowledge of the patient or the examiner. The identity of the glasses was not revealed until all the data had been collected. Owing to colour adaptation, participants were unaware of the exact colour that they selected in the intuitive colorimeter. The adaptation meant that the colour appearance of the lenses necessary to provide the ‘optimal’ colour under conventional lighting was more saturated than participants generally expected.
Subjects wore the coloured glasses as and when they wished for 6 weeks and then returned them to the ophthalmic tinting company. At least 2 weeks later the second pair (‘optimal’ or ‘control’) was posted to the patient and these were also available for wearing for 6 weeks. From the time of the first testing with the intuitive colorimeter to the end of the period when the second tints were worn, patients completed daily symptom diaries detailing any headaches that they experienced.
At the time of the first colorimeter assessment, the subjects were given a range of optometric tests, including visual acuity, refraction, orthoptic tests of binocular function, contrast sensitivity, and an assessment of pattern glare (see below). The optometric assessment was repeated again at the end of the study three times: with the ‘optimal’ tints, with the ‘control’ tints, and without any tinted lenses. The order of this testing was randomized and the examiner remained unaware of the identity of the lenses until the end of the second examination. Further details of the methods and results can be found in Evans et al. (35).
Psychophysical tests
Spatial contrast sensitivity was assessed by the Vistech near test at a distance of 0.3 m, so that the spatial frequencies of the targets were 1, 2, 4, 8 and 12 cpd (35). All three versions of the test were used (35, 36) and the three results at each spatial frequency were averaged. The luminance was about 70 cd.m−2.
Pattern glare was assessed by asking patients about the symptoms of visual perceptual distortions that they experienced when binocularly viewing a four-cycle-per-degree horizontal square-wave grating (5). To control for suggestibility, patients were also asked the same questions whilst they viewed a control grating, spatial frequency 0.5 cycle per degree, that would not be expected to induce pattern glare. The gratings had a Michelson contrast of 0.8 and were circular in outline, diameter 0.1 m, and were viewed at a distance of 0.4 m. The protocol stated that subjects with a history of epilepsy were to be excluded from the pattern glare testing. Although no subjects met this criterion, one experimental subject found that the experimental grating made her feel nauseated so this test was omitted.
To elicit any symptoms of pattern glare the seven questions were asked: Do you see a colour or colours? Do the lines appear to bend? Do the lines seem to blur? Does the pattern flicker? Do the lines wobble or shimmer? Do parts of the pattern disappear and reappear? Do you see any other patterns, shapes, or glare? (patients were asked to specify).
Participants were asked to view each grating for 5 s and to fixate a small dot in the centre of the grating. They were first shown the control grating and asked to answer the first question, then the experimental grating for the first question, then the experimental grating for the second question, then the control grating for the second question, then the control grating for the third question, and so on. Subjects were asked to quantify their response to each question as ‘none’ (scored as 0), mild or ‘a little’ (scored as 1), and severe or ‘a lot’ (scored as 2).
The above procedure was then repeated, but using successively two four-cycle-per-degree gratings of similar hemiradius, one in each lateral hemifield. Subjects were repeatedly reminded to fix the fixation spot to ensure that a hemifield was stimulated. Previous work has shown a link between headache incidence and the number of illusions reported, but not differentially for some illusions more than for others (5). The scores were therefore summed for each patient. After the pair of gratings had been presented for each question the subjects were asked which hemifield grating produced the most illusions.
Results
Chromaticities of tinted lenses
The chomaticities of the tinted lenses are shown in Fig. 1, the ‘optimal’ chromaticities by square symbols connected by a line to the chromaticity of the associated ‘control’. The majority of ‘optimal’ tinted lenses were various shades of blue. The chromaticity of the ‘control’ lens was selected so as to have similar saturation (CIE suv) but to differ by a CIE LUV colour difference of about 80. In Fig. 1 the saturation is represented by the distance of a symbol from (equal energy) white (shown by the cross) and is similar for ‘optimal’ and ‘control’ lenses. The difference in colour is represented by the length of the line joining the points and is similar for all patients.
Although telephone contact with the patients was maintained throughout the study, and all patients completed their diaries throughout, four failed to attend the final appointment, despite prompting.
Optometric data
None of the participants had a strabismus or a vertical heterophoria on cover testing, apart from one subject with monovision contact lenses. None had a vertical fixation disparity or foveal suppression at distance. All participants achieved the test ceiling of 250′ on the Randot random dot test of stereoacuity. The Vistech test of contrast sensitivity revealed impaired contrast sensitivity in only two cases (7, 14) at 12 cpd and 8 and 12 cpd, respectively. At no spatial frequency did the group means differ significantly from those of matched controls (35).
At the follow-up appointment the optometric and psychometric tests were repeated under three conditions: no tint, ‘optimal’ tint and ‘control’ tint, presented in random order (35). The only measure to show a significant difference between the two tints was dissociated heterophoria, a near vision test that assessed the alignment of the visual axes of the two eyes subjectively by presenting a horizontal scale to the left eye and a pointer to the right. The performance of this test was significantly more variable with the ‘optimal’ than with the ‘control’ tint (Wilcoxon P=0.004), and close to the value with no tint. Dissociated heterophoria is known to be a very poor predictor of symptoms (36, p. 49). Other tests of heterophoria (36, pp. 50–64) that are generally more highly correlated with symptoms (including headaches) failed to reveal any significant difference between the two tints (34).
On the pattern glare test participants reported significantly increasing degrees of perceptual distortions in the following order: ‘optimal’ tint, ‘control’ tint and no tint (Friedman test, P<0.001), but the pattern glare with ‘optimal’ tints was not significantly less than with the ‘control’ tints (Wilcoxon test, P=0.62). Only one subject reported any illusions on viewing the control grating; they were mild despite a high score with the experimental grating.
Analysis of symptoms
The headache diaries were analysed by dividing days into those with symptoms and those without, including any symptoms of head pain. (Although the questionnaire asked for symptoms associated with pain, it was not sufficiently detailed to be sure of a classification of the headache as migraine.) In Fig. 2 each point represents a participant, and the position of the points is determined by the percentage of days with symptoms when the ‘optimal’ tinted lenses were worn and when the ‘control’ lenses were worn. As can be seen, there are 11 points above the diagonal, and 6 below, indicating that, on average, the frequency of headache was greater when the ‘control’ tint was worn. The difference was marginally significant for the group by a one-tailed t-test (t(16)=1.417, P=0.08). The log odds for the distribution of points (which took into account the bionomial sampling and the number of observations) gave an overall probability of 0.02. There were four participants for whom the difference between the lenses was individually significant (P<0.05, Fisher's exact test), and these are shown by solid points, three above the diagonal and one below.

Results of the study. Each symbol represents a patient and the position of a symbol is determined by the proportion of days with symptoms when the ‘optimal’ tinted lens was worn (abscissa), and the proportion when the ‘control’ tinted lens was worn (ordinate), neglecting days when no lenses were worn. The symbols above the diagonal therefore represent patients for whom wearing the ‘optimal’ tint was associated with fewer symptoms than the ‘control’ tint. The solid symbols represent patients for whom the difference between the tints was significant for that individual. The triangles represent patients who had migraine with aura and the squares patients who had migraine without aura. The numbers beside each symbol identify the patients, as per Table 1.
Discussion
The findings lend support to the observations of the preliminary open trial in suggesting an effect of tint on headache incidence. Unfortunately the effect is statistically marginal. Nevertheless, the present studies would tend to confirm the role of visual experience in influencing headaches in some sufferers, and show that reduction of headache may perhaps be possible by a simple modification of that experience. As reviewed above, there is increasing evidence for visual involvement in migraine, although the role of visual treatment has seldom been subject to controlled study.
The difference between ‘optimal’ and ‘control’ lenses could have arisen because the ‘optimal’ tint reduced symptoms or because the ‘control’ tint increased them, or both of these. It is impossible in principle to determine which is the appropriate explanation because, even if baseline data had been available, any comparison between baseline and intervention would not have been blind.
Data from the present study cannot be used to predict the benefit of tinted lenses in unselected patients with migraine. The study participants reported benefit from a coloured overlay when reading and were not already wearing tinted lenses. However, only four patients were excluded because they failed to find an overlay helpful.
Mechanism for the visual trigger
Turville (37) noted that lights and patterned stimuli (white railings) can be a headache trigger, and several authors have associated pattern glare with migraine (5, 7, 10, 15, 39). The glare has been attributed to a local and patchy cortical hyperexcitability, cells in hyperexcitable regions firing inappropriately and giving rise to perceptual distortion and associated discomfort (39). Chronicle and Wilkins (40) have linked such discomfort to the benefit from colour by showing that individuals with migraine differ from age- and sex-matched controls with respect to the greater consistency with which they chose certain coloured illumination (generally red) as aversive when viewing text. Cortical cells in V3 responsible for the analysis of shape and those in V5 responsible for the analysis of movement vary considerably in their spectral sensitivity (40, 41) and coloured spectacles should therefore necessarily redistribute the cortical excitation that results from visual processes. It is possible that the ‘optimal’ colour redistributes the cortical excitation that results from the vision of everyday stimuli: ‘comfortable’ tints may redistribute the excitation in such a way as to reduce the excitation in hyperexcitable regions. This might be of particular consequence when the excitation is strong, as in the case of stimuli such as text that evoke pattern glare (8).
In conclusion, individually prescribed coloured filters may perhaps offer an effective treatment for some patients with migraine, although further studies will be necessary to confirm this viewpoint. The mechanism for any such benefit may be related to cortical hyperexcitability. For those individuals who can benefit from colour, a wide range of colours may need to be assessed because the tint may need to be precisely specified, as indicated by the difference in response to ‘optimal’ and ‘control’ filters in this and a previous study (26).
Acknowledgements and declaration of interest
We thank the patients who took part in these studies and their general practitioners. We thank the Medical Research Council for support. We thank Dr R.C. Peatfield of Charing Cross Hospital for a neurological diagnosis of the patients and for advice on an earlier draft of the manuscript. We thank Dr R. Capildeo for referring the patients in the pilot study to BJWE. The Medical Research Council owns the rights to the intuitive overlays and intuitive colorimeter and pays an ‘Award to Inventors’ to AJW.