
Abstract
The prevalence rates of headache in first-born children were determined at the ages of 6 and 12 years in over 1000 families. A headache questionnaire was mailed to 1132 families when the children were 6 years old, and to 1126 families when the children were 12 years old. Seven hundred and ninety-eight families responded to both questionnaires. The prevalence of headache before the 6 months preceding the questionnaire ('previous headache') was 19% when the children were 6 years of age and 31% when the children were 12 years of age. The corresponding prevalences of headache during the 6 months immediately proceeding the questionnaire ('present headache') were 16% and 19%. Variation in occurrence of headache was high during follow-up years. Maternal frequent headache (≥1/month) was significantly associated with the increase in prevalence of present headache in boys between the ages of 6 and 12 years. Frequent headache in mothers, fathers and siblings, and the occurrence of chronic illness, were also significantly associated with headache in the 12-year-old children.
Keywords
Introduction
Almost everyone suffers from headache at some time during their lives. Headache is one of the most common pain symptoms in children. Although the causes of headaches are rarely life-threatening, adults and children sometimes worry about them (1). Headache can impair life in many areas and daily activities can be adversely affected (2, 3). Migraine is a major cause of absence from school (4).
The reported prevalence rates of headache have been 3% to 6% at 3 and 4 years of age (5, 6), 20% at 5 years of age (7) and 35% to 50% at 7 years of age (8, 9). The lifetime prevalence of headache has been reported to be 70% to 80% in children of 13–15 years of age (8, 10). Ten to twenty per cent of children under 10 years of age and 20% to 35% of those aged 11–16 have been reported to suffer from recurrent headache (11–13). There have been only a few reports of prospective follow-up studies of changes in prevalence of headache during childhood. It has been reported that prevalences of headache and migraine increase gradually from 11 years of age. From the pre-pubertal period on, prevalences in girls have been reported to be markedly greater than those in boys (10, 14, 15).
The aims of our study were to determine whether there were changes in the prevalence of headache between pre-school age and prepuberty, and to assess factors related to the occurrence of headache in children in a population-based group. In particular we sought to answer the following questions:
How does the prevalence of headache change over the first 6 school years?
What factors are associated with any change?
Which factors are associated with prevalence of headache at age of 12 years?
Does reporting headache differ between parents and children?
Study population and methods
Study population
The study is a part of the Finnish Family Competence Study, which began in January 1985. The study focuses on ways of life and health behaviour in young Finnish families, with a view to developing public health services in the areas of health education and socio-emotional support. The study covered the Province of Turku and Pori, in south-west Finland. Subjects were identified on the basis of stratified randomized cluster sampling. Stratification involved division of the study region into two parts, the southern area (Turku University Hospital Region) and the northern area (Satakunta Central Hospital Region). Each cluster consisted of the population resident in a health-authority area, the smallest administrative unit in the Finnish public health-care system. Eleven of the total of 35 health authority areas were selected by lot, with weighting according to stratum. All 67 maternity health clinics and 72 well-baby clinics in the 11 health-authority areas participated in the study. Of 1582 families, 1443 (91%) gave informed consent to participate. The distribution of occupations among the 139 mothers who declined to participate was similar to that among those who agreed to participate (16). The mothers gave birth to 1294 first children. Three children died during birth. Eight children died in infancy, and five moved abroad. One hundred and forty-six could not be traced. The remaining 1132 mothers and children were followed-up from the beginning of pregnancy until the children concerned reached 12 years of age (Fig. 1).

Creation of study population.
At 6 years of age, completed questionnaires were returned by 968 families (86% of 1132), and at 12 years of age by 906 families (80% of 1126). Questionnaires were separately completed by 900 children (79% of 1126). A question relating to child headache during the 6 months before completion of the questionnaire (‘present headache’) was answered by 798 families (79% of 968, 84% of 906) at ages 6 years and 12 years.
Methods
Questionnaires were given separately to mothers and fathers, to be returned in sealed envelopes to the investigators. Questionnaires were issued by nurses during visits to well-baby clinics. When the children were 6 and 12 years of age questionnaires were mailed to the children's homes. Parents, and nurses at well-baby clinics, were asked to complete questionnaires about the health and health-related factors of the parents and their children. When the children were 12 years of age they were also asked to complete their own questionnaire.
Prevalences of previous and present headache and the change in prevalence of headache were regarded as outcome variables. When the children were 6 and 12 years of age, parents were asked two questions relating to headache:
Has your child had headache disturbing his/her daily activities in the past 6 months? (‘Present headache’)
Has your child had headache disturbing his/her daily activities at some period in his/her life prior to the past 6 months? (‘Previous headache’)
At 12 years of age the children themselves were asked:
Have you had headache disturbing your daily activities in the past 6 months?
Have you had headache disturbing your daily activities at any period in your life prior to the past 6 months?
Data on headache prevalence in the children when they were 6 years of age have been published elsewhere (3).
The following variables were also studied in order to assess their relationship to childhood headache: familial occurrence of frequent headache; sociodemographic and psychosocial factors relating to the family; and each child's state of health.
Familial occurrence of headache was studied by asking both parents about frequent occurrence of headache among parents prior to the mother's pregnancy (‘pre-pregnancy headache’). The same headache questions were asked again 12 years later. If a parent reported at least one episode of headache or migraine attack per month, he or she was regarded as suffering frequently from headache. Also the parents were asked about headache occurrence in the siblings when study children were 12 years of age.
The four sociodemographic variables were maternal age on becoming pregnant (< 25, 25–29 or > 29 years), sex of child, parental occupation (professional, service-sector employee, worker in industry, or other, e.g. primary production employees), and nature of residential location of the family (urban, suburban or rural) (17).
Psychosocial variables were changes in family structure (including divorce or separation of the parents).
The child-health variable included existing illness that had lasted for more than 6 months (not headache), e.g. diabetes mellitus, bronchial asthma or allergy.
Statistical methods
Statistical calculations were performed using the GEE estimation method for logistic regression analysis of correlated binary responses available in the MULTILOG procedure of the SUDAAN statistical program package (18, 19). Associations between variables and occurrence of headache as reported in the questionnaire at 12 years of age were analysed by means of univariate and stepwise multivariate logistic regression analysis (18), using the SAS System for Windows, release 8.1/1999. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated, in the latter case using Wald's formula based on normal approximation: CI = exp(b ± 1.96 SE(b)), where b is the estimate of the coefficient in the logistic model and SE(b) is the standard error. A P-value of < 0.05 was considered to indicate statistical significance.
Results
Characteristics of families
When the children were 12 years old, the mean age of the mothers was 38.8 years (range 29–54 years). Fifty-six per cent of the mothers were in professional occupations, 26% worked in the service sector and 18% in industry or primary production. Seventy-one per cent of the families lived in towns, 17% in suburbs and 12% in rural areas. Seventy-seven per cent of the children lived with their biological parents. Eleven per cent lived in a one-parent family and 9% in a new family. Three per cent of the children lived in other circumstances, e.g. with grandparents. Fifty-three per cent of the study children were girls.
Change in prevalence of headache between 6 and 12 years of age
The prevalence of present headache increased from 16% at 6 years of age to 19% at 12 years of age. The change in prevalence rate is not statistically significant (P = 0.07). Only 6% of children had present headache at both 6 and 12 years of age. More children began to suffer from headache than ceased to suffer from headache between 6 and 12 years of age (12% vs. 9%) (Table 1). The prevalence of previous headache increased from 19% at 6 years of age to 31% at 12 years of age (P < 0.001). The difference in the increase between boys and girls was not statistically significant.
Prevalence of present headache (headache during the 6 months preceding completion of questionnaire) and previous headache at 6 and 12 years of age

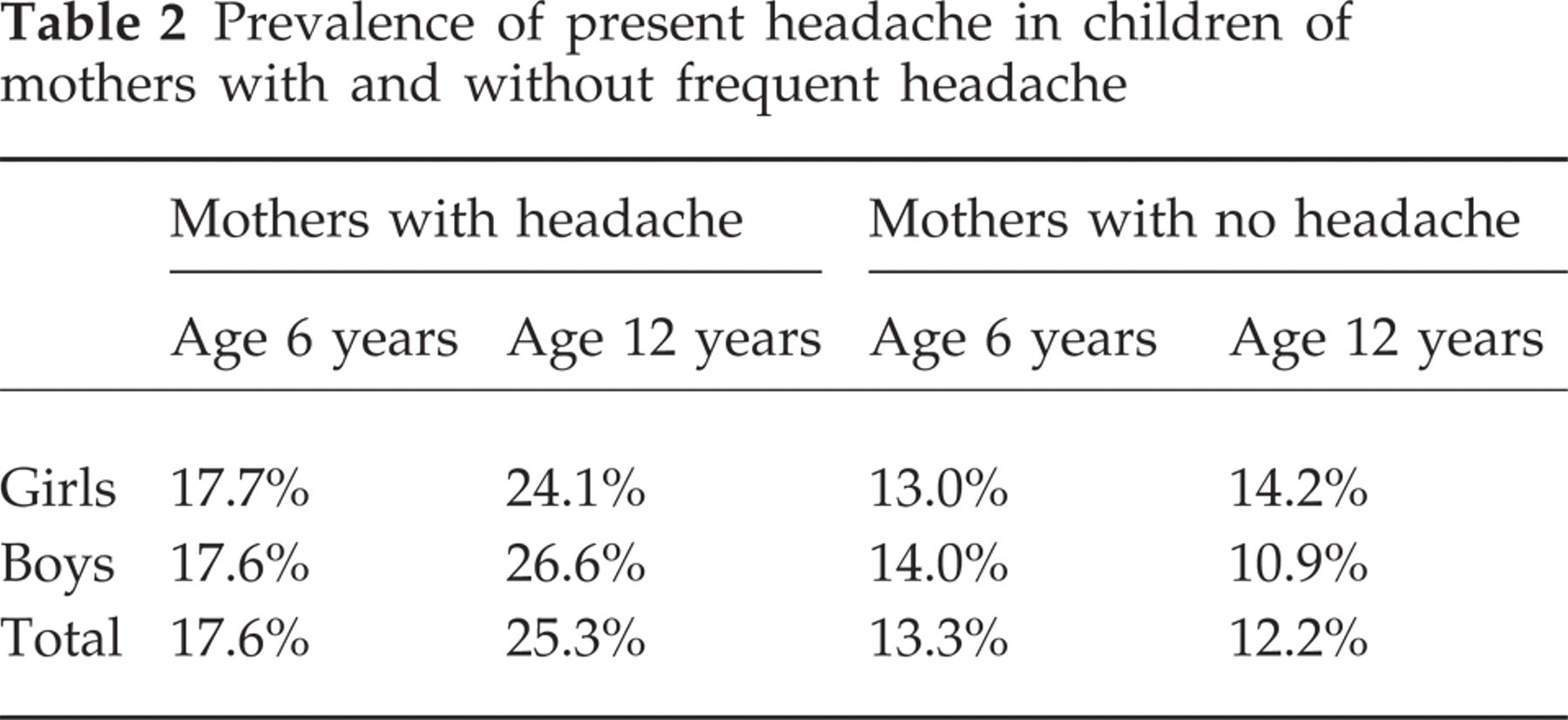
The change in prevalence of present headache between 6 and 12 years of age was statistically significantly greater in relation to children whose mothers reported suffering frequent headache when the children were 12 years of age (P = 0.03; OR 1.7; 95% CI = 1.1–2.9) than in relation to children whose mothers were headache-free. When the data for boys were analysed separately, the difference in the increase in headache prevalence was also statistically significant (P = 0.01; OR 2.5; 95% CI = 1.2–5.0) but for girls the difference was not statistically significant (P = 0.47; OR 1.1; 95% CI = 0.6–2.5) (Table 2). There were no significant differences for boys or girls whose fathers reported suffering frequently from headache in the questionnaire when their child was 12 years old.
Prevalence of present headache in children of mothers with and without frequent headache
A change in prevalence of headache in children was not significantly associated with the mother's or father's frequent, pre-pregnancy headache, siblings frequent headache in the 12-years questionnaire, maternal age, parental occupation, nature of residential location, change in family structure or the child's suffering from chronic illness.
Factors associated with present headache at 12 years of age
Table 3 shows that for mothers who reported in the questionnaire when their children were 12 years of age that they suffered frequently from headache, the odds ratio relating to present headache in the children was 2.2. Father and siblings suffering frequently from headache and the children suffering from any chronic disorder at 6 or 12 years of age, or both, were also significantly associated with present headache in the children.
Variables found to be associated with present headache (headache during the 6 months preceding completion of questionnaire) on stepwise logistic regression analysis (SLRA) in 12-year-old children (OR=odds ratio, CI=confidence interval)
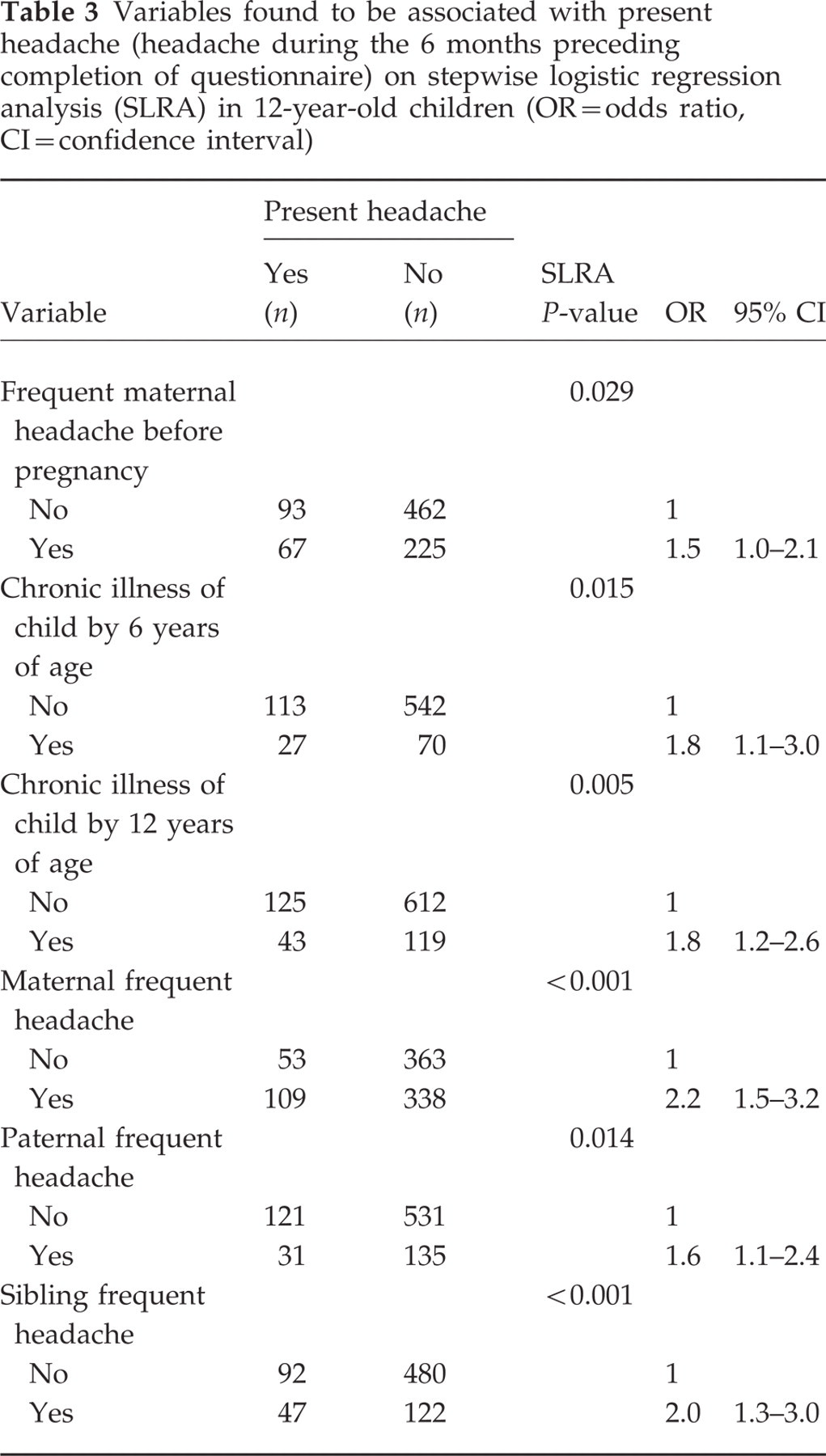
Sex of child, father's frequent headache before the mother's pregnancy, nature of the child's residential location, parental occupation, maternal age and change in family structure were not significantly associated with reports of present headache in the questionnaire when the children were 12 years old.
Comparison of children's and parents' reports on children's headache
When the children were 12 years of age, 889 pairs of parents and children answered separately and independently questions about the occurrence of headache in the children. Children's headache was reported by 173 (19%) children themselves and 160 (18%) of their parents. The difference was statistically non-significant and showed a good congruity between the two information sources.
Discussion
The main aims of the study were to determine whether there was any significant change in prevalence of headache in the children between 6 and 12 years of age, and to identify factors associated with any changes. The prevalence of present headache increased after the first 6 years of school, but only marginally significantly. Maternal, frequent headache was significantly associated with the change in prevalence of present headache in boys. The present study is, as far as we are aware, first to demonstrate a significant role of maternal headache in such a connection. The finding has obvious practical implications.
The study population was drawn from what had originally been a stratified cluster sample of young Finnish families, highly representative of the population of the region overall, with no significant bias in distribution (20).
The natural course of headache in childhood has been examined in only a few prospective population-based studies. Bille (15) reported that the prevalence of migraine was 1.4% in children of 7 years of age, 5.3% in children of 12 years of age. At puberty 62% of the children with migraine were headache-free (21). In a follow-up study Sillanpää (14) found the prevalence of headache in children of 7 years of age to be 37%. In children of 14 years of age it was almost 70%. For migraine the corresponding percentages were 2.7 and 10.6. In 22% of children, migraine ceased to occur between ages 7 and 14 but in 41% it remained unchanged or became worse. The difference in headache prevalence between the two ages is greater than the difference found in our study. The change in prevalence of present headache (from 16% to 19%) was low, probably, because ‘headache disturbing daily activities’ was carefully defined, as we wanted to study the kind of headache that affects the quality of a child's life. Despite the increase in prevalence of present headache between 6 and 12 years of age that we found was substantial, variation in occurrence of headache was high. Six per cent of the children had permanent, present headache, while others began to suffer from headache or remitted.
Diagnosis and treatment of headache are mainly based on clinical interview and physical examination. The younger the child, the greater the care needed to identify headache. Knowledge relating to a child's headache is usually based on how parents interpret symptoms. Andrasik et al. (22) found no difference of reporting about children's headache between children and parents. This is also what we found in our study. The children seem to be reliable reporters of their symptoms. Children should always be given the opportunity to tell their own stories.
Children suffering from headache have been found to have family histories of headache, usually on the mother's side (3, 23). In a study by Messinger et al. (24), the prevalence of headache was 64% in headache sufferers when neither parent suffered from headache, 85% when one parent suffered from headache and 98% when both parents suffered from headache. In our study the only statistically significant association seen related to the change in the prevalence of headache was occurrence of maternal frequent headache in children, especially in boys at 12 years of age.
Frequent maternal headache before pregnancy was strongly related to the occurrence of headache in children below school age (3). This same association was also found in our study with children of 12 years of age.
Changes in family life are known to influence child's health and to be factors in childhood disease (25). Discontinuity factors (e.g. divorce) have been used to describe negative changes in the family (26). Marital problems, including separation or divorce of parents have been found to be related to recurrent headache in children (27, 28) and adolescents (29). However, there are also conflicting reports (13, 30). In our study, some 20% of the parents were divorced or the children were living in one-parent families. However, we found no association between changes in family structure and child's headache in relation to the pre-pubertal period.
Childhood headache is normally benign, transient and inconsistent in nature, but part of it can develop to become chronic and disabling. Many biological, environmental and social factors can cause headache during early school years. The course of headache attack is difficult to predict in any individual child. The results of the study reported reveal specific points to which attention should be paid during early school years. Children were found to be capable of reporting reliably about their headaches if given opportunity and time to do so. Careful medical examination of each child should be accompanied by enquiry into family history. It is important to pay attention to mother's headache as early as possible, especially in boys suffering from headache. Whether relationship between maternal frequent headache and child's headache is genetic or environmental in origin remains still unclear.
Footnotes
Acknowledgements
Appreciation is expressed to Edmund Gordon MA for revising the English of this report, Mrs Inger Vaihinen for her secretarial assistance, and to Olli Kaleva BSc for skilful computation of the statistical analyses.